
Abstract
Attention deficit hyperactivity disorder (ADHD) is a common condition and important for the affected individual, their family and society. It manifests with pervasive symptoms of hyperactivity, impulsivity and inattention. In many children with ADHD these symptoms persist into adolescence and adulthood. Drug treatment with psychostimulants, including methylphenidate, is an important part of a comprehensive treatment plan for children with severe ADHD that includes psychosocial, behavioural and educational advice and interventions. Methylphenidate is a central nervous system stimulant, whose mechanism of action is thought to be due to an increase in catecholamines in areas of the brain concerned with motivation and reward. Methylphendiate is available in short acting (immediate release) and longer acting (modified release) forms. Pharmacotherapy for ADHD is in three stages: initiation, maintenance and termination. The efficacy of methylphenidate in terms of reducing core symptoms is 70% as compared to placebo. This efficacy is maintained for at least 24 months. Methylphenidate generally has a favourable side effect profile. The most significant side effects include appetite suppression with an initial deceleration in height velocity, cardiovascular side effects that are not clinically significant in children with no adverse cardiac history, and tics. Methylphenidate is generally well tolerated and liked by children and adolescents with ADHD, who appreciate the benefits that medication has on their behaviour.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a common and important childhood condition, affecting many areas of a child's life. It manifests in early childhood with pervasive symptoms of hyperactivity, impulsivity and inattention that are inappropriate for the child's developmental stage. The core symptoms are based on observations about how children behave: “impulsivity” signifies premature and thoughtless actions, such as running out into a busy road; “hyperactivity” is restlessness and shifting with an excess of movement, for example being unable to stay in a chair during school lessons; and “inattention” is a disorganised style preventing sustained effort, for example making careless errors in schoolwork, or appearing not to listen. 1 The manifestations of the disorder change as the child becomes older; as the individual matures and the environmental requirements for sustained self control increase. 1 For example, hyperactivity in an adolescent may present as excessive fidgetiness rather than the whole body movement seen in hyperactive younger children.
ADHD is an important disorder to recognise and treat because these symptoms affect the child or adolescent's academic, behavioural, emotional and social functioning, with increased rates of delinquency, road traffic accidents and substance misuse in adolescence.1–4
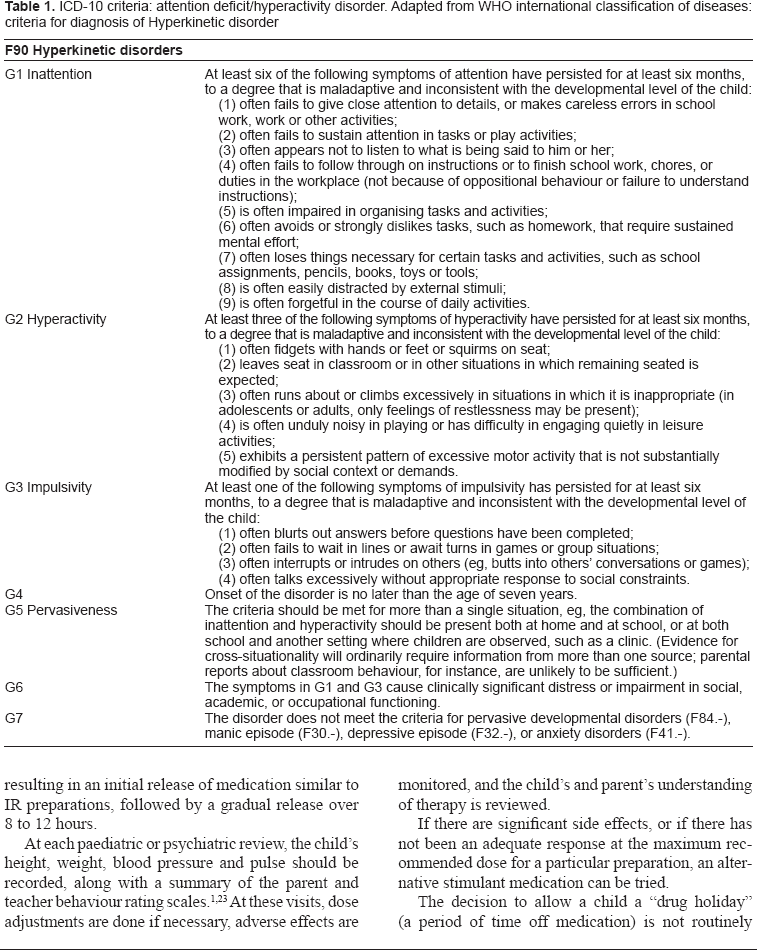
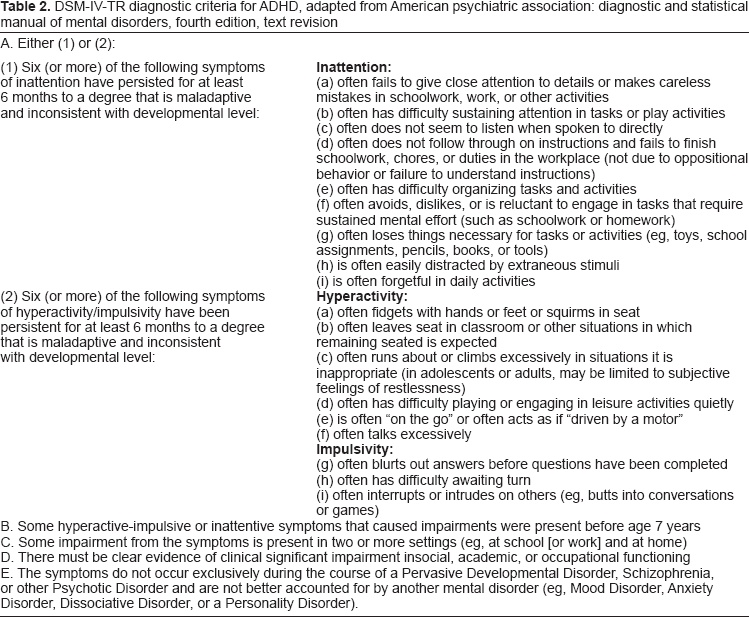
The American Psychiatric Association's diagnostic scheme (DSM-IV-TR) 5 and the World Health Organisation's classification of diseases (ICD-10) 6 use a description of the behaviour patterns seen in ADHD to classify and diagnose the disorder. North American and European practice diverged in previous years: in North America moderate and severe patterns of disease were recognised and termed “ADHD”, in Europe only severe forms of the disorder were recognised, and termed “hyperkinetic disorder”. The terminology in Europe has now changed, with clinicians using the term “ADHD”, even when more strict criteria are applied for diagnosis.
Prevalence estimates of ADHD vary depending on the population sampled, the method of ascertainment and the diagnostic criteria applied. 2 The prevalence estimates vary between 1.7% and 17.8% depending on the criteria used, with most estimates lying between 5% and 10%. 2 Generally prevalence estimates from North America where the looser DSM-IV-TR criteria are applied are higher than those from Europe, where the more restricted ICD-10 criteria are used. 7 Usually, ADHD is a persisting disorder. A review of longitudinal studies found that 15% of children with ADHD will continue to have symptoms as an adolescent and into adult life, and 65% of adults who had ADHD as a child will fulfil the diagnosis of “ADHD in partial remission” (a term for individuals who no longer fulfil the full criteria for a diagnosis of ADHD). 8 In addition, a large proportion of children with ADHD will subsequently develop a personality disorder or a substance misuse disorder in adulthood.9–11
Diagnosis of ADHD requires that the ICD-10 (hyperkinetic disorder) or DSM-IV-TR (ADHD) criteria are met, and that there is educational, psychological or social impairment in multiple settings (for example at home and at school) as assessed by a psychiatrist or paediatrician. This often requires the help of a multidisciplinary team and direct observation of the child in different settings.
ADHD causes significant morbidity, and must be treated. Available treatment modalities include medication, psychological interventions and educational interventions. 2 In the United Kingdom, the National Institute for Health and Clinical Excellence (NICE, a group that develops clinical practice guidelines) 1 and the Scottish Intercollegiate Guidelines Network (SIGN, part of the National Health Service for quality improvement in Scotland) 2 recommend that drug treatment for ADHD in children and young people should be reserved for those children with severe symptoms and impairment only, and should always form part of a comprehensive treatment plan that includes psychosocial, behavioural and educational advice and interventions.1,2
There are three types of drug licensed to treat ADHD; methylphenidate hydrochloride and amphetamine sulphate, which are psychostimulants, and atomoxetine. When a decision has been made to treat children or young people with ADHD with drugs, either of the psychostimulants should be considered first line based on a long record of safety and efficacy.1,2,12–14 This review will consider only methylphenidate.
It is more than 70 years since the fortuitous observation that stimulant drugs can improve hyperactive behaviour in children. 15 Methylphenidate has been available since 1955 in the US, and since 1995 in the UK. Since then the level of drug prescribing for ADHD has increased markedly in the developed world. Methylphenidate is a controlled drug in the UK. 16
Mechanism of Action, Pharmacokinetic Profile and Metabolism
Methylphenidate is a central nervous system (CNS) stimulant drug whose mechanism of action in ADHD is not completely clear. Methylphenidate is believed to work by affecting the dopaminergic and noradrenergic systems, causing an increase of these catecholamines at CNS synapses.17,18 This is achieved by blocking the presynaptic membrane dopamine transporter, thereby inhibiting the re-uptake of dopamine and noradrenaline into the presynaptic neuron. 1 These catecholamine storage sites are present throughout the CNS, but it is thought to be the increased amounts of noradrenaline and dopamine concentrations in the brainstem, midbrain and frontal cortex that are responsible for the increased attention span and concentration that occur when children with ADHD take stimulants, because these brain regions are associated with motivation and reward.18,19
Methylphenidate is a sympathomimetic, meaning that it belongs to a group of drugs that mimic the sympathetic nervous system by increasing catecholamines at CNS synapses. Due to its mechanism of action, there are several pharmacodynamic interactions with similar or antagonistic drugs. Methylphenidate antagonises the hypotensive effects of adrenergic neurone blockers. There is a risk of a serious hypertensive crisis when given with a monoamine oxidase inhibitor (MAOI), and some manufacturers advise not to prescribe methylphenidate within two weeks after taking a MAOI. There is also a risk of a hypertensive crisis when given volatile liquid general anaesthetics. Methylphenidate possibly inhibits the metabolism of selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants. Methylphenidate possibly increases plasma concentration of phenobarbital and phenytoin, and may increase side effects from risperidone. 16
Methylphenidate is quickly and almost completely absorbed from the gastrointestinal tract and easily passes to the brain. 20 Due to its pronounced first-pass metabolism, the absolute bioavailability is low at only 30%. 1 Maximum plasma concentration after oral administration occurs at about 2 hours, but is variable between individuals so careful dose titration is necessary. 20 Significant reduction in core symptoms (ie, hyperactivity, impulsivity and inattention) usually occurs at doses between 0.3 and 0.6 mg/kg. Methylphenidate is a short-acting stimulant with a duration of action of 1 to 4 hours and a pharmacokinetic half-life of 2 to 3 hours in the immediate-release (IR) preparations. This means that if the IR preparations are used, 2–3 daily doses are required. For this reason, methylphenidate is available in both modified-release (MR) preparations, as well as the immediate release preparations. These are used for dose titration and maintenance therapy respectively.
Pharmacotherapy for ADHD is in 3 stages: Titration, Maintenance and Termination.
Titration
Titration can be done with a MR preparation, but is more often done using an IR formulation, normally started at a dose of 5 mg twice or three times a day at 4 hourly intervals. Dosage and frequency are titrated according to symptom response to a maximum recommended dose of 60 mg per day. 16 The optimal dosage is when ADHD symptoms are improved with at the lowest dose with minimal side effects.
During the titration stage, the child's response to the medication should be monitored using standardised rating scales (such as the Connor's questionnaire) on a regular basis, and the child should be seen regularly during this phase. 21 The rating scales used for assisting in diagnosis and monitoring of ADHD are based on the DSM-IV (ADHD) or ICD-10 (hyperkinetic disorder) diagnostic criteria, and ask the parent or teacher to subjectively rate the child's behaviour in each of the domains of inattention, impulsivity and hyperactivity.
Maintenance
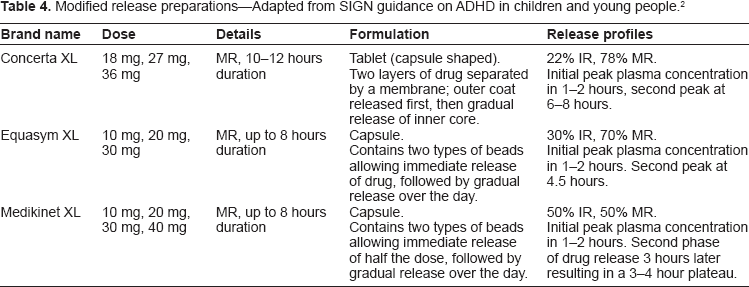
Children can be maintained on the IR formulations, but the multiple dose regimen has difficulties for the child or adolescent such as administration of the drug at school, storage of a controlled drug at school, stigma and poor compliance.1,22 These problems led to the development of sustained or modified release formulations (see Tables 3 and 4). These medications are taken once daily in the morning, resulting in an initial release of medication similar to IR preparations, followed by a gradual release over 8 to 12 hours.
ICD-10 criteria: attention deficit/hyperactivity disorder. Adapted from WHO international classification of diseases: criteria for diagnosis of Hyperkinetic disorder
DSM-IV-TR diagnostic criteria for ADHD, adapted from American psychiatric association: diagnostic and statistical manual of mental disorders, fourth edition, text revision
Immediate release preparations–-Adapted from SIGN guidance on ADHD in children and young people. 2

Modified release preparations–-Adapted from SIGN guidance on ADHD in children and young people. 2
At each paediatric or psychiatric review, the child's height, weight, blood pressure and pulse should be recorded, along with a summary of the parent and teacher behaviour rating scales.1,23 At these visits, dose adjustments are done if necessary, adverse effects are monitored, and the child's and parent's understanding of therapy is reviewed.
If there are significant side effects, or if there has not been an adequate response at the maximum recommended dose for a particular preparation, an alternative stimulant medication can be tried.
The decision to allow a child a “drug holiday” (a period of time off medication) is not routinely recommended, 1 and should only be done on a case by case basis. The effects of a drug holiday were evaluated by Martins et al 24 in 2004 in a placebo controlled trial when they randomly assigned 40 children to receive methylphenidate 7 days a week, or for 5 days a week with weekend doses of a placebo. The weekend parent rating scales or Monday teacher rating scales showed no significant difference between the two groups, but the drug holiday group had significantly less insomnia.
Termination
Methylphenidate should be continued for as long as it is clinically effective for the child or adolescent. The decision to terminate methylphenidate must be made jointly with the child or adolescent, their parents, and the health care professionals involved. Clinical need, benefits and side effects must be taken into account. The decision to stop methylphenidate should take into account the behavioural effects of missed doses and drug holidays. 1 When the decision has been made to stop methylphenidate, abrupt withdrawal is safe.
In addition to the oral forms of methylphenidate, there is also a patch available in the US (at the time of writing it is not available in Europe). There are four strengths available in the patch, including 10 mg, 15 mg, 20 mg and 30 mg immediate release methylphenidate. The patch should be applied 2 hours before the effect is needed, and removed after 9 hours. The effect can last up to 12 hours. 25
Before starting a child or adolescent on methylphenidate for ADHD, a pre-drug assessment must be completed. NICE recommends that this must include: 1
Full mental health and social assessment
Full history and physical examination, including:
assessment of history of exercise syncope, undue breathlessness and other cardiovascular symptoms
heart rate and blood pressure (plotted on a centile chart)
height and weight (plotted on a growth chart)
family history of cardiac disease and examination of the cardiovascular system
Electrocardiogram (ECG) if there is past medical or family history of serious cardiac disease, a history of sudden death in young family members or abnormal findings on cardiac examination
Risk assessment for substance misuse and drug diversion (where the drug is passed on to others for non-prescription use)
Children and adolescents with ADHD who are taking methylphenidate require regular monitoring to review adherence to the treatment plan, adverse effects, and response to methylphenidate.1,2,12 Medication adherence can be monitored by noting the dates of prescription requests. Core symptoms can be monitored through ADHD rating scales, or through reports from the child's teacher.
Efficacy
Methylphenidate reduces core symptoms of ADHD and improves quality of life in children and adolescents diagnosed with ADHD.1,26 The efficacy of methylphenidate in terms of reduction of core symptoms as determined by a parent or teacher using rating scales is 70% as compared to a placebo. 28 Approximately 80% of children will respond to at least one type of the methylphenidate preparations. 27 Because of the clinical effectiveness of methylphenidate, the National Institute for Health and Clinical Excellence (NICE), 1 the Scottish Intercollegiate Guidelines Network (SIGN) 2 and the American Academy of Pediatrics (AAP) 3 recommend methylphenidate as the first line drug treatment for children or adolescents with ADHD.
The short-term effectiveness of methylphenidate in children and adolescents with ADHD was assessed in a large meta-analysis completed in 2001. 62 placebo-controlled randomised trials involving a total of 2897 children and adolescents (median age 8.7 years) with a primary diagnosis of ADD (attention deficit disorder with or without hyperactivity) were reviewed. Most of the studies used a cross-over design and were short in duration (average three weeks). Each primary outcome demonstrated a significant effect of methylphenidate as measured on hyperactivity scales or indices: effect size (ie, standardised mean difference) reported by teacher 0.78, 95% (confidence interval 0.64–0.91); effect size reported by parent (0.54, 95% CI 0.40–0.67). 28
The long term effectiveness of methylphenidate in children and adolescents with ADHD has been assessed in a large, high quality study over 14 months, the Multimodal Treatment Study of Children with ADHD (MTA Study), conducted in 1999. 29 his was a randomised controlled trial of 579 children with ADHD designed to assess the effectiveness of long term medication and behavioural therapy. The children were allocated to one of four groups over 14 months. The groups included medication management (titration followed by monthly visits); intensive behavioural treatment (parent, school, and child components, with therapist involvement gradually reduced over time); the two combined; or standard community care (in which 2/3 of the children received medication prescribed by community care providers). Results demonstrated a reduction in ADHD core symptoms over time for all four groups. Children in the combined treatment and medication groups showed significantly greater improvements than the children in the community care or intensive behavioural treatment groups; the improvement in ADHD core symptoms was not significantly better in the combined treatment group compared to the medication only group. At this point, randomisation ended. In a naturalistic follow-up study, consistent use of stimulant medication for 24 months was associated with maintenance of effectiveness, albeit with a reduced effect. 30
Safety
Methylphenidate has been used for many years to treat the symptoms of ADHD, and is generally thought to have a favourable side effect profile.
General side effects
The most common side effects associated with methylphenidate are mild and of short duration. The commonest side effect is appetite suppression (80% children taking methylphenidate), with only a small proportion (10%–15%) losing weight. 3%–85% children suffer from sleep disturbances. Other reported side effects include tachycardia, increased blood pressure, headache, social withdrawal, rebound irritability and abdominal pain.31–33 Rare but more severe adverse events can include psychotic symptoms and sensitivity reactions requiring discontinuation of the medication. 1
The consequences of many of these adverse effects can often be overcome by adjusting the dose, timing or formulation of the methylphenidate.1,3 For example, appetite suppression can be improved by administering the dose after or just before a meal, and sleep disturbance can be improved by prescribing a shorter acting preparation.
Weight and growth
A systematic review of the effects of methylphenidate on weight and height found reduced growth velocities in some children during initial treatment with methylphenidate, with some studies finding a later acceleration in linear growth with continued medication use. There was no good evidence to suggest that final adult height was affected. 31 Data from the 36 month follow-up of children in the MTA trial did suggest an adverse effect on growth, but there is no data on final adult height. 32
Seizures
ADHD is common in children with epilepsy (40% prevalence). 33 There is no good evidence to suggest an increase in seizure frequency in a child with well controlled epilepsy and ADHD who is prescribed methylphenidate. However, the small number of trials that evaluated the use of methylphenidate in children with epilepsy were generally of small sample size and short study duration, and performed on children with well controlled epilepsy.34–36 It would therefore be prudent to closely monitor seizure frequency when starting a child with epilepsy on methylphenidate. 37 It is noted in the literature that patients with seizures are generally excluded from the majority of studies regarding treatment for ADHD. 38
Cardiovascular risks
There have been rare reports of adverse cardiac events, including sudden death, in children and adolescents taking methylphenidate. However, a causal relationship has never been established, and there is no evidence to suggest that there is an increased risk of sudden death in adolescents taking methylphenidate as compared to the general population. Methylphenidate has small cardiovascular effects, including a small but clinically non-significant effect on blood pressure in short-term use (average increase 5 mmHg), 39 with a slight increase in pulse rate (average 5 bpm). 40 Research looking at ambulatory blood pressure monitoring of boys who had been receiving methylphenidate for at least 2 months indicated statistically significant increases in systolic and diastolic blood pressure when the child was awake and a decrease in sleep. 41
The advice from guidance bodies in the UK and the US (NICE, SIGN and the AAP) is that it is safe to start a child on methylphenidate, provided that there are no risk factors in the history, and they have a normal cardiovascular examination.
Psychiatric symptoms
There are rare reports of psychiatric side effects in children and adolescents taking methylphenidate, including psychosis and mania. One study found that there were a total of 11 events of psychosis or mania occurring during 743 person-years of double blind treatment with CNS stimulants. 42 It is recommended that methylphenidate is discontinued in the unlikely event that the child or adolescent experiences psychotic symptoms.
Tics
Tics are stereotyped, involuntary, purposeless repetitive movements typically of facial or proximal muscles that cause motor or sonic phenomena. Children with Tourette syndrome have multiple motor and at least one vocal tic for more than a year. Over half of all children with Tourette syndrome have symptoms of ADHD. A meta-analysis of studies evaluating the treatment of children with Tourette syndrome and ADHD showed that methylphenidate does not tend to increase the frequency or severity of tics, although this result remains controversial and the effect on individual patients is difficult to predict. 43 In one study of children with Tourette's syndrome, tics increased only with high doses of stimulant medication and were observed to diminish over time in some of those treated with methylphenidate. 44 In children without premorbid tic disorders treated with methylphenidate for ADHD, 15%–30% will develop motor tics, which usually resolve spontaneously. 12
Misuse or diversion of methylphenidate
Diversion of methylphenidate involves giving away or selling the drug to those for whom it was not prescribed. Misuse involves taking excessive doses of methylphenidate. Methylphenidate is misused or diverted either to enhance performance (for example during school examinations) or for subjective effects (to achieve a “high”). There is a paucity of evidence for this in Europe. People with ADHD carry a higher risk of drug abuse compared with their peers without ADHD. This may be related to their impulsive behaviour or a concomitant conduct disorder. In the US, Wilens et al systematically reviewed studies looking at diversion and misuse of ADHD medication. 5%–9% of school age and 5%–35% of college age children disclosed that they had used non-prescribed stimulants in the previous year. 16%–29% of children and adolescents who were themselves prescribed methylphenidate had been asked to sell or give away their medication. 45 Diversion and misuse was more common with immediate rather than delayed release preparations. To reduce methylphenidate diversion and misuse, it is important to keep a record of prescription dates and to prescribe long-acting methylphenidate formulations, 1 as well as educating parents and adolescents about the need to avoid misuse and diversion.
Patient preference
Methylphenidate is recommended as first line drug treatment for children and adolescents with ADHD becauseit is known to be safe and effective. Duration of action and preparation of the drug are important considerations when helping the child or adolescent choose between the different formulations of methylphenidate.
There has been a paucity of research looking at the experiences of children and young people with ADHD taking stimulant medication. Available qualitative studies suggest a “trade-off” between the positive and negative experience of stimulant medications.46–48 While the children in these studies reported that medication helped to control hyperactivity, increased concentration, improved grades and helped behaviour,46,48 negative aspects such as the taste of the medication and side effects of stomach aches and headaches 47 were also mentioned, along with psychological side effects of feeling less sociable and a sense of not feeling authentically themselves. 46
There was also considerable concern from the young people interviewed about the stigma of having to take medication to control their behaviour. They were worried that other children would laugh at them, or they were concerned with the changes in personality they experienced in themselves. 47 There was also concern from the children at having to leave the classroom to be given medication. 46
A study used by the group writing the NICE guidance on ADHD 1 by Singh et al found that children generally had positive experiences of stimulant medication: they were prepared to put up with taking tablets for the perceived benefits. The children had a reasonable understanding of the benefits and limitations of medication. While children understood that there may be benefits to their school work, the main perceived benefits of the medication was to help improve their disruptive behaviour, and therefore improve relationships with peers. Side effects were noted by the study participants, but these did not make up a major theme. All children interviewed felt that they needed to take their medication. 49
Reassuringly, the diagnosis of ADHD and taking of medication were not listed as important worries by children or adolescents at any age group in the study by Singh. Results from this study suggest that children have relatively more positive experiences of medication, as compared with more negative experiences of ADHD diagnosis and behavioural symptoms. 49
Conclusions
ADHD is a common and an important disorder for the affected child or adolescent, for their family, and for society as a whole. It must be recognised, correctly diagnosed and treated. Treatment for ADHD must involve the adolescent or child, family and school. Effective treatment will include behavioural, psychological or educational interventions as well as drug treatment in selected cases. Decisions regarding initiation of drug treatment must be made on a case by case basis in collaboration with the family.
Since the mid-1990s the level of drug prescribing for ADHD has increased markedly in the developed world. The increase in prescribing can be attributed to changes in regulatory frameworks and the introduction of MR preparations, but also because clinicians are increasingly aware of this important disorder. If drug treatment is to be used, guidelines suggest that methylphenidate should be tried first in most cases. This is due to the knowledge that methylphenidate is effective at reducing the inattention, poor concentration and hyperactivity of ADHD, and most importantly because the children and adolescents with ADHD have generally positive experiences of taking it.
Disclosure
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.