
Abstract
Multiple sclerosis (MS), a chronic inflammatory-degenerative illness of the central nervous system (CNS), remains at the moment a treatable but incurable disease. Currently available disease-modifying agents (DMA-s), the majority of which are being injected, mainly relieve the inflammatory phase of MS with little beneficial effect, if any, in halting neurodegeneration. Cladribine is an immunosuppressive agent that can be administered orally and by cycles of short-course dosing as opposed to continuous administration. Cladribine has been shown to be effective in reducing inflammatory activity of MS but much remains unknown regarding its potential beyond the control of CNS inflammation. In addition, knowledge on the safety profile of cladribine in MS is limited. Data from on going clinical studies and registries on its safety profile will shed more light on the actual benefit/risk ratio of cladribine.
Keywords
Introduction
Multiple sclerosis: a chronic disease of young adults
Multiple sclerosis (MS) is a chronic inflammatory-degenerative illness of the central nervous system (CNS), affecting mainly young adults in their most productive years. 1 The disease starts with an inflammatory component sustained by blood brain barrier (BBB) leakage. This promotes the passage of inflammatory mediators and immune cells from the periphery which, in their turn, amplifies inflammation within the CNS tissue. 2
Active lesions by gadolinium contrast enhanced T1-weighted (T1-w) magnetic resonance imaging (MRI), termed contrast-enhancing lesions (CELs), are believed to be the radiological correspondent of this inflammatory process. Inflammation triggers the occurrence and maintains the symptoms of clinical flares.
If left untreated, CELs by MRI would last approximately one month. 3 However, symptoms and seqeuelae of clinical relapse and consequential changes in disability may take longer to disappear or stabilize. The use of steroids induces a prompt recovery and promotes faster and better CEL resolution. 4 Inflammation spans over a limited time window but almost invariably evolves into the formation of chronic lesions visible by T2-w MRI and, in approximately 20% of the cases, in chronic black holes (cBHs) by T1-w MRI. Histopathological studies indicate that different degree of demyelination and axonal loss may subtend those chronic lesions. 5 In a subset of patients, an ultimate culmination of lesions into fluid-filled cavities is seen by cerebrospinal fluid tissue specific imaging (CSF-TSI). 6 Intuitively, depending upon their underlying pathology and topographical distribution in the brain and the spinal cord, chronic lesions may have different impact into the physical disability of patients with MS.
This phase of MS, prevalently characterized by inflammation and lesion formation, is known as relapsing-remitting (RR) MS. As time progresses, a slow but ominous degenerative process advances whereby white matter (WM) and grey matter (GM) tissues are lost at the advantage of CSF volume expansion and in the absence of visible inflammatory lesions. This pathological process leads to a substantial and irreversible accretion of brain and spinal cord atrophy. 7 Although its pathogenetic mechanisms are unknown, it is certainly undoubted that MS-induced atrophy has an important role in determining the physical, cognitive and emotional disability seen in patients. Atrophy development mainly characterizes the secondary progressive (SP) MS stage. In approximately 10% of the patients, the disease starts and invariably progresses towards accumulation of disability in the absence of clearly evident clinical relapses. This type of disease is denominated Primary Progressive (PP) MS.
Presently, MS is a treatable but incurable disease. Seven partially effective agents are available as preventive therapies in MS. These disease-modifying agents (DMA-s) mainly relent the inflammatory phase of RRMS with little beneficial effect, if any, in PPMS and SPMS. Moreover, six out of seven DMA-s suffer the limitation of being injected intravenously (iv), subcutaneously (sc) or intramuscularly (im), thus negatively affecting patient compliance. 8 As a consequence, clinical scientists are devoting their effort towards the study of therapies which can be effective in patients with MS while administered orally (po).9,10 Cladribine is one of such therapies. On March 2011, cladribine was not approved by the U.S. Food and Drug Administration (FDA). The FDA requested additional information concerning the drug's safety.
This purine analog is only available in the US for parenteral administration marketed under the trade name Leustatin for cancer-related applications. The oral formulation for MS is approved only in Australia and Russia. In late summer 2010, the European Medicines Agency (EMA) rejected the new drug application for the oral formulation in the EU, citing unfavorable risk-benefit ratio.
Cladribine, an emerging oral therapy for MS?
Cladribine (chemical name: 2-chlorodeoxyadenosine, C10H12CIN5O3, molecular weight 285,69kD) is a purine analogue, competitive inhibitor of the adenosine desaminase enzyme. Physicians treating immune mediated conditions are familiar with another purine nucleoside analogue, azathioprine. Cladribine and azathioprine have similar chemical structures to purine nucleosides with noticeable differences. In neuro-immunology, azahtioprine is commonly used in the treatment of neuromyelitis optica. 11 Before the 90s and prior to the availability of the currently used DMA-s such as interferon beta (IFNβ) and glatiramer acetate (GA), azathioprine was frequently utilized to prevent new disease flares and to relent disease progression in MS as well. Today, azathioprine is used off-label to treat MS refractory to commonly used DMA-s. 12
Cladribine, officially launched in the United States in February 1993, is currently approved by the Food and Drug Administration (FDA) for the treatment of hairy cell leukemia. 13 Cladribine has also been used to treat acute myelogenous leukemia, chronic lymphocytic leukemia, chronic myelogenous leukemia, cutaneous T-cell lymphoma, and non-Hodgkin's lymphoma. 14 Furthermore, cladribine is used off label in treatment of resistant cases of histiocytosis.15–17 The effects of cladribine have also been studied in rheumatoid arthritis and glomerulonephritis.18,19 Presently, cladribine is under investigation for B cell leukemias and lymphomas, such as mantle cell lymphoma. 20
The history of cladribine dates back to discoveries made by Dr. Carson and colleagues in a genetic condition known as adenosine desaminase (ADA) deficiency. This rare disorder is associated with drastic reduction of lymphocyte populations and severe immunodeficiency. 21 The characteristic lymphopenia in ADA deficiency is caused by the accumulation of deoxyadenosine nucleotides within lymphocytes.22,23Based on these observations, Dr. Carson's team synthesized several therapeutic purine nucleoside analogs with immunosuppressive effects, including cladribine. 19
Perhaps not unexpectedly, it has been a rocky road towards the potential approval of cladribine in MS. 14 Ortho Biotech and The Scripps Research Institute have been the key developers of this medication as an MS-related DMA. Following the early trials at the Scripps Clinic, Ortho filed a new drug application with the FDA in 1997 for the use of cladribine in the treatment of RRMS and SPMS. An FDA drug advisory committee meeting was planned to take place in January 1999. However, Ortho Biotech had to cancel this meeting: following an FDA inspection between December 1998 and January 1999, the Scripps Clinic received a warning letter from the FDA in April 1999 regarding violations in the early clinical studies of cladribine in MS. As a result, the new drug application was withdrawn with the conclusion that additional clinical studies would be necessary. More than a decade later, the drug is still in the approval process.
In the present review we aim at highlighting the current role of cladribine in the MS clinical arena. After reviewing the drug mechanisms of actions, we will discuss key clinical studies performed thus far related to the drug effectiveness and safety. We will then conclude by addressing the ideal patient candidates for cladribine treatment and its place in therapy.
Mechanism of Action, Metabolism and Pharmacokinetic Profile
Mechanisms of action
Cladribine enters its target cells via purine nucleoside transporters and undergoes phosphorylation intracellularly. 24 The drug is metabolized to 2-chlorodeoxyadenosine triphosphate. Triphosphate nucleotides are trapped intracellularly. Dephosphorylation by 50-nucleotidase is required to prevent such intracellular accumulation. 25 However, lymphocytes have low levels of 50-nucleotidase and are therefore particularly vulnerable to cladribine's effects. The resulting accumulation eventually disrupts DNA synthesis and repair and leads to sustained reduction of lymphocyte numbers via apoptosis. 26 In vitro studies have shown that cladribine has numerous actions on the immune system. Those actions ultimately confer potent immunsuppressive properties to the drug which may be responsible of the beneficial effect seen in MS.
Effect of immune system effectors
In addition to reduction of proliferating lymphocyte populations (as in leukemias and lymphomas) cladribine causes a relatively rapid and long-lasting reduction in quiescent lymphocyte populations. 27 Such action is important from the standpoint of treating autoimmune and inflammatory diseases. The ability of cladribine in reducing quiescent lymphocyte populations is likely explained through the induction of accelerated DNA strand breaks, which leads to the consumption of Nicotinamide Adenine Dinucleotide (NAD) for poly-ADP-ribose synthesis, which could induce critical depletion of ATP. This mechanism of action is observable not only in actively proliferating, but also in resting lymphocytes. 27
It is particularly relevant to MS that cladribine is thought to cross the BBB. 24 Cladribine preferentially targets and decreases the number of T cells (both CD4 and CD8+ cells, but mainly CD4+ cells). It also depletes B cells, but has only minor effects on natural killer (NK) cells.26,28 The relative preservation of key innate immunity cell types may explain the lower than expected incidence of infections despite a substantial reduction in lymphocyte numbers,28,29 although increased frequency of opportunistic infections and perhaps increase in autoimmune complications like autoimmune hemolytic anemia have been seen with parenteral use in hematological conditions. 27
In a study conducted by a Polish group 30 10 RRMS patients received cycles of five consecutive daily iv infusions at five-week intervals (clustered dosage) while 10 other RRMS patients received one infusion weekly (nonclustered dosage). The clustered dosage produced a decline in granulocyte count, a delayed decrease in monocyte count, and a transient decrease in red blood cell (RBC) count. The nonclustered dosage caused a larger and persistent decline in RBC count, a smaller decrease in monocyte count, and no change in granulocyte count. Both regimens reduced NK and B-cell subsets (by 40%–60% and >80%, respectively) but only transiently. The treatments caused long-lasting declines, >50%, in CD4+ T-cell subsets, without a significant change in CD8+ T-cell subsets. Overall, the nonclustered dosage was less toxic to myeloid precursors and more toxic to erythroid lineage precursors.
Effects on leukocyte migration
Drugs that inhibit leukocyte, especially lymphocyte migration via the BBB are expected to be effective in MS, as demonstrated in the case of natalizumab. 31 Based on in vitro observation in a Boyden chamber assay, cladribine decreases the migratory capacity of CD14+ monocytes as well as of CD4+ and CD8+ T-lymphocytes, with T-lymphocytes being more affected than monocytes. No difference in this effect could be demonstrated when comparing mononuclear cells from MS patients with cells from healthy controls. Therefore, cladribine might achieve its clinical and paraclinical efficacy by inhibiting the migration of inflammatory cells into and within the CNS. 32
Effects on cytokine profile
In addition to the well known effects of lymphocyte depletion, cladribine may also have complex effects on cytokine profiles in MS. Significantly lower serum interleukin-2 (IL-2) levels, reduced CSF levels of the chemokine CXCL8, and serum and CSF levels of CCL5 (RANTES) have been reported following cladribine treatment.33,34 Therefore, while the main effect of cladribine is likely to be related to actual lymphocyte depletion, it is reasonable to hypothesize that at least part of the observed immunomodulatory effect is related to alterations of cytokine levels.
Potential epigenetic properties of cladribine
Newer observations have highlighted that in addition to immune cell depletion and changes in cytokine levels, cladribine also possesses epigenetic properties: it inhibits the enzyme S-adenosyl homocysteine hydrolase and DNA methylation. This may contribute to its observed efficacy in MS. 35
Metabolisms and pharmacokinetic profile
In discussing the topic of cladribine pharmacokinetics, it is important to highlight the fact that therapeutic drug concentration and metabolism remain not well defined yet.
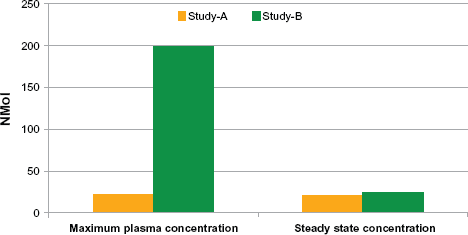
Cladribine has a half-life (t½) of 5 to 7 hours and 18 to 19 hours depending upon the elimination phase. 36 The drug has an oral availability of approximately 40%, which is in part affected by food intake 37 and depends upon route of administration. 36 Cladribine is eliminated via the kidneys without an extensive metabolism. Following po administration, cladribine is rapidly absorbed. It has a wide, ie, 9 l/kg, volume of distribution and a relatively low plasma binding, ie, 20%. 36 Dosing of 0.28 mg/kg (double of the typical iv dose) po reaches equivalent bioavailability, volumes of distribution and excretion profile compared with an equivalent dose by two-hour bolus and sc administrations. 36 In their turn, two-hour bolus and infusional cladribine produce comparable areas under the curve. 37 However, sc administration may yield a 2-fold greater mean peak concentration than continuous iv 2-hour bolus administrations. 36 A pharmacokinetic analysis of hair cell leukemia patients without leukemic cells showed that their area under the concentration versus time curves of plasma cladribine increases dose-dependently. 39
We report examples on the variability of pharmacokinetic parameters (ie, maximum plasma concentration) observed in studies on different patient populations, ie, hairy cell leukemic and lymphoid malignancies of different ethnicity and treated with different dosages of cladribine in Figure 1.37,39 As stated earlier, cladribine penetrates the BBB, reaching a CSF/plasma concentration of approximately 25% of plasma level. 24
Cladribine has been evaluated in patients with other malignancies and a number of inflammatory conditions. Nevertheless, little is known about its pharmacokinetics in these disease states. 35
Clinical Studies
The number of phase-II and phase-III clinical studies evaluating safety and tolerability as well as testing effectiveness of cladribine in patients with MS is limited. At the time of the present review, the results of four studies have been published.28,40–44 Two of these studies report on safety, tolerability and efficacy of cladribine sc administered; one on iv infusions and one on po administrations. While in two studies the drug effect was investigated in RRMS patients, two others considered patients with progressive MS. In addition, while in two studies a limited number (ie, <100) of patients was included, two others considered an extensive number of patients and provide phase-IIb and phase-III clinical evidence.
It is important to highlight, however, that at the time of the present report, the investigation of cladribine tablets as a first-line DMA in patients with MS is still ongoing. Currently three large phase-IIb or phase-III clinical trials are being performed. Briefly, the first study 45 is an extension of the CLARITY (CLAdRIbine Tablets treating multiple sclerosis orallY) study in RRMS patients. 42 The investigators are evaluating if the effect and the safety profile of cladribine vs. placebo is sustained beyond a 96-week time period in RRMS patients.
The second study, the ONWARD (Oral cladribine added oN to rebif new formulation in patients With Active Relapsing Disease) clinical trial is evaluating the effect of adding cladribine tablets or placebo to IFNβ therapy, in terms of both safety, tolerability and efficacy in RRMS patients. 46
Last, safety and efficacy of monotherapy with cladribine tablets vs. placebo is being evaluated in patients with a first clinical demyelinating event at high risk of developing MS. Goal of this phase-II placebo controlled clinical trial, ORACLE (ORAl CLadribine in Early MS), is to evaluate the drug's ability in preventing conversion to clinically definite MS. 47
Safety
General issues
In general, an increased frequency of opportunistic infections and perhaps increase in autoimmune complications, including autoimmune hemolytic anemia, were observed with this product. 25 Very few infections have actually been documented but they do occur. 42 These infections are largely responsible for the 3% mortality rate associated with cladribine therapy in hairy cell leukemia treatment. Fever is a common adverse effect with parenteral administration of cladribine. A key issue related to this is the obvious fact that immunosuppression can lead to fever due to actual infections; however, this drug can cause fever that lasts for up to 48 hours without actual infections. Neutropenic fever is not unusual among chemotherapy drugs, however, neutropenia is not a common adverse effect of this medication with the doses utilized in MS treatment. Existing studies in hairy cell leukemia estimate that from 18% to 42% of patients will experience fever in this manner. This transient fever can be treated with medications like acetaminophen (paracetamol in Europe). If fever was a complication in MS cases, it may lead to pseudo-exacerbations and Uhthoff phenomenon, which were not reported in any of the MS trials to date. In addition to fever, cladribine increases the risk of herpes virus infections in hairy cell leukemia case; particularly shingles was very prominent from this standpoint.
When treating hematological malignancies, many patients experience fatigue while on cladribine, even in the absence of anemia. Since fatigue may also be a common symptom of these diseases (including MS), ascertaining to what extent is caused by the underlying disease instead of the drug remains difficult.
Cladribine does not cause hair loss, vomiting, or other adverse effects (AE) that are commonly associated with “old style” alkylating chemotherapy drugs, even in high doses.49,50 However, peripheral neuropathy has been reported occasionally after repeated doses of cladribine in the treatment of hairy cell leukemia, and the signs and symptoms related to this may be erroneously attributed to MS. Overdose can also cause kidney damage. Unusual pathologies including lachrymal gland, retina, and extrabulbar optic nerve pathology were also observed in animal models, but only with high dose treatment required for hematological malignancies.51–53 These potential AE were not reported among MS cases, but are important to know of for future monitoring.
Significant bone marrow suppression was reported even with the early trials of cladribine. There was also one active hepatitis case in the early trial, which led to mortality. This was not thought to be directly related to the medication, although it is hard to conclusively prove that. As always, clinical vigilance and surveillance will be very much needed when this drug becomes available for clinical use.
Safety related issues in patients with MS
In patients with MS, cladribine has been generally safe and well tolerated, regardless of its route of administration and the type of the treated MS patient. AE tend to be dose-related. Table 1 summarizes the relative incidence of the AE related to cladribine administrations as reported in the major clinical trials.28,42,44 Interestingly, in each of these studies, despite the expected decrease in white blood cells (WBC) counts, the overall incidence and severity of infections tended to be similar across groups (ie, treated vs. untreated patients). As seen for patients with hair cell leukemia, an increased risk of herpes zoster, but without dissemination, was reported in both RR and progressive MS patients. This was observed even in the early trials by the Scripps team.44,54,55 Nevertheless, drug discontinuation and patient withdrawn due to occurrence and severity of AE were rarely observed. Although few patients presented with solid malignancies during therapy with cladribine, none of these cancers could be unambiguously ascribed to the therapy.
Reported adverse events (AEs) with cladribine therapy.
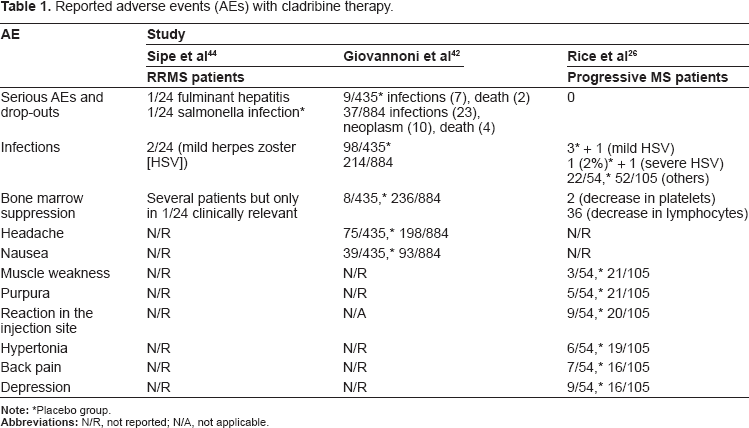
In general, no major treatment-related effects on hepatic, renal function tests, other serum chemistries, vital signs, body weight, physical findings, and cardiac activity were seen. Most of the drug-related AE such as pain, urinary tract infection, muscle weakness, hypertonia, purpura, rhinitis, and ataxia were judged as mild to moderate in severity. WBC, RBC and platelets decreases were observed, although none of such decreases reached worrisome values. A dose-dependent decrease was observed in the number of CD3+, CD4+, CD8+, CD16+, CD56+ T cells subset and, to some extent, CD19+ lymphocytes.
A recent detailed analysis of cladribine-related AEs confirms that AEs tend to be dose related in RRMS patients 56
Recently, the results of detailed analysis of AEs related to cladribine administration in RRMS patients of the CLARITY study 42 became available. 56
Overall the analysis showed that at least some of the AEs related to cladribine tend to be dose dependent, occurring twice as frequently in patients treated with higher doses of the drug. The most common reason for study discontinuation was abnormal lymphocytes counts that involved 0.9% of the patients in the cladribine 3.5 mg/kg (low-dose) group and 3.5% in the 5.25 mg/kg (high-dose) group. Also, 0.7% patients in the high-dose group withdrew from the study due to leukopenia. However, if one does not take into account patients withdrawn because of leukopenia, the proportion of patients interrupting the study was similar across the three groups. Irreversible lymphopenia was observed in 11% of the patients, ~70% of whom in the high-dose group. The incidence of neutropenia and leukopenia was much lower, ranging around 1%. Decrease in platelets counts and increase in creatinine levels could be doubtfully ascribed to cladribine therapy and changes in liver enzymes levels were comparable between treated and untreated patients.
Infections occurred in a proportion of patients ranging from 42.5% (ie, placebo group) to 49.7% (high-dose group). Herpes zoster without dissemination was the most common infection, and it was only observed in the treated groups. Interestingly, 70% of the patients who developed herpes zoster had normal lymphocyte counts or grade 1–2 lymphopenia. One patient died for reactivation of pre-existing tuberculosis, pointing towards the importance of screening patients for tuberculosis infection at the time of therapy start.
Although three patients developed malignancies during therapy with cladribine once again, no increased risk of neoplasm can be attributed to the drug at the present time.
Clinically mild AEs were reported in most organ systems. Of note, commonly reported AEs involved the nervous system (ie, ~1% hypesthesia, syncope, somnolence, paresthesia, migraine and radiculopathy), the skin (ie, ~3% alopecia, rash, dermatitis allergic and acne), and the cardiovascular system (ie, ~1% angina pectoris).
Such detailed analysis represents and important step towards the understanding of the safety profile of cladribine. To address and monitor safety concerns related to the increased risk of infections and potential malignancies, a safety registry detaining long-term safety data related to cladribine use, has been initiated. 57
It is indeed important to highlight the fact that more work is needed to properly address the safety profile of this drug in patients with MS. Clearly the AE rate seen in patients with cancer is unlikely to be accepted for MS patients, given the fact that, although the MS population has an increased disease mortality, as opposed to cancer, MS reduces the life expectancy only minimally. 58 In addition, it is important that while assessing the benefit of cladribrine in relation to its risk, one takes into account the benefit/risk ratio today assessed for commonly employed DMA-s 59 and guarantee an equal, if not higher, safety profile of new medications compared to approved therapies. The latter is especially true when the therapeutical efficacy of a new product is not expected to be radically improved compared to available alternatives.
Efficacy
Studies in patients with RRMS
The first evidence of cladribine efficacy in RRMS patients dates back 1999
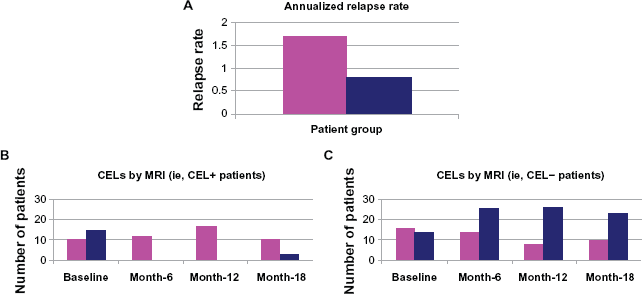
Cladribine efficacy in RRMS patients has been first assessed in a phase-II double-blind, placebo-controlled randomized clinical trial. 43 Fifty-two RRMS patients were randomized to receive either cladribine 0.05 mg/kg/day for five consecutive days, monthly for six months with the intent to reach a cumulative dose of 2.1 mg/kg/day or an equivalent volume of saline solution, iv. Twenty-seven patients received cladribine, whilst 25 were treated with placebo.
The study design included: monthly clinical and MRI (ie, CELs counts) assessments over the first 12 months of therapy followed by 3-month-interval evaluations during the second year of the study, up to month 18. Primary aim of the study included number and severity of clinical relapses. To this end, it was calculated that 25 subjects per arm would be sufficient to detect a 50% decline (ie, from 1 in the placebo arm to 0.5 in the treated group) in the mean number of clinical relapse after one year of therapy, while securing an alpha error ≤5% (study power not specified by the authors). An additional primary aim was given by the frequency of CELs by MRI. Specifically, the authors postulated that 50% of the patients in the placebo group and 10% in the treated group would have at least 1 CEL at year one of therapy. With respect to this primary aim, a sample size of 25 subjects per arm secured an alpha error ≤5% with a study power = 90%.
Changes in physical disability assessed by the Expanded Disability Status Scale (EDSS) 60 and the Scripss Neurological Rating Scale (SNRS) 61 although rated, were not part of the outcome metrics of the clinical trial. No other clinical and imaging measures were included.
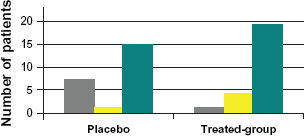
Of the 52 enrolled patients, 44 (84.6%) completed the study, 25 in the drug-cohort and 19 in the placebo-cohort. A significant reduction in the frequency and severity of clinical relapse was found in the treated group compared to the placebo group starting by month 7 and up to month 18 of the study (Fig. 2A). Patients with lower EDSS at the baseline and fewer relapses in the year preceding the study had a better study therapy outcome. Throughout the same time period, patients treated with cladribine had a substantial reduction in the frequency of CELs at month-12 and month-18 of therapy compared to baseline. This reduction in CELs was not visible in the placebo group. A smaller number of patients with active lesions were seen in the treated group compared to the untreated one (Fig. 2B and 2C), although no clear predictors of MRI outcome could be identified. No changes in measures of physical disability (ie, EDSS and SNRS scores) were seen.
The first evidence of cladribine efficacy in RRMS patients dates back 1999. 43
In 2010, clinical efficacy of cladribine in RRMS patients is confirmed
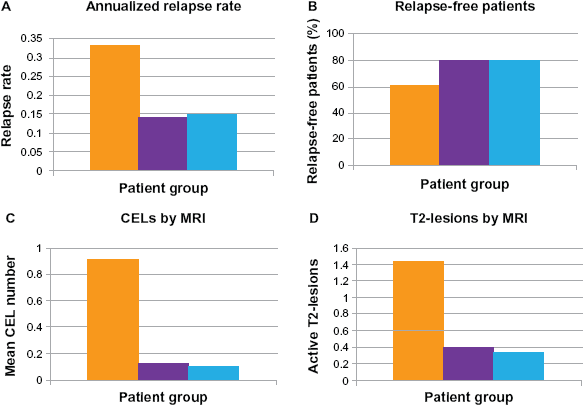
In the CLARITY study, a more recent a phase-III double-blind, placebo-controlled randomized clinical trial lead by Dr. Giovannoni 42 1,326 RRMS patients were randomly assigned to three treatment arms for a time-window of 96 weeks. The drug was administered po as short courses. During the first 48-week trial, the first treatment arm received two courses of cladribine 3.5 mg/kg followed by placebo; the second arm received four courses of cladribine 5.25 mg/kg and the third arm received four courses of placebo. In the second 48-week trial period, both treatment arms received two courses of cladribine and the placebo group was treated with two courses of placebo.
Neurological examinations, rating disability by the means of the EDSS score, were performed at baseline (pre-therapy), at day 1, week 13, 24, 36, 48, 60, 72, 84, 96. MRIs, which allowed the measurement of CELs, active T2-lesions and combined unique lesions, were obtained at baseline (pre-therapy), at 24, 48, 60, 72, 96.
The number of clinical relapse at week-96 provided the primary endpoint. To this end, on the basis that a mean number of 2.1 of clinical relapse would occur in the treated group with a standard deviation of 2.02 in each group, it was computed that a sample size of 1,290 patients was sufficient to detect a significant decrease by 25% in the number of clinical relapses in the cladribine-group, while ensuring a study-power of 90% and a type-I error of 2.5%. Secondary study endpoints were given by the three MRI measures.
Overall, 1,184 (89.3%) patients completed the study. As illustrated in Figure 3, compared to placebo both treated groups had a significantly lower number of relapses (Fig. 3A), higher proportions of relapse-free patients (Fig. 3B), longer time-interval before a clinical relapse occurred during the study period (data not shown), lower CELs (Fig. 3C), active T2-lesions (Fig. 3D) and combined unique lesions (data not shown).
In 2010, clinical efficacy of cladribine in RRMS patients is confirmed. 42
Studies in patients with progressive MS
Early studies in the 90s seem to suggest a positive effect of cladribine on measure of physical disability in chronic progressive MS patients
Cladribine efficacy in progressive MS patients has been initially evaluated in a double-blind, placebo-controlled randomized cross-over clinical trial initiated by Dr. Sipe and co-workers44,61 in 1992. Fifty-one patients with “chronic progressive MS” for longer than two years were randomized to receive either four monthly of weeklong courses of cladribine 0.7 iv or an equivalent volume of saline solution. Twenty-four patients received cladribine, 24 patients matched by age, sex and severity of disease received placebo. As a result, the likelihood of sustained progression to disability was significantly lower in each treated group when compared to placebo.
Primary endpoint was neurological improvement as provided by the decreases in SNRS scores. To this end, it was calculated that a decrease by 15% would be seen in treated patients compared to “no change’ in untreated ones would be clinically relevant. To detect such a change while ensuring a study power of 90% and an alpha error of 5%, 22 subjects per arm would be sufficient. Every patient was evaluated monthly and disability assessed using the EDSS and the SNRS scores and imaged every six months.
Over the 1-year observational period, progressive deterioration in both EDSS and SNRS scores was seen in the placebo group while in treated patients a modest amelioration was seen. Mean paired differences in EDSS and SNRS scores were: 0.6 (0.3) and 8.9 (2.2, respectively at month-6 and 1.3 (0.3) and 12.5 (2.0), respectively at month-12. 44 Confidence intervals (CI) showed statistically relevant differences only for the SNRS score. Proportions of patients showing worsening, or improvement in the EDSS score, presented in Figure 4, favored the treated group. MRI data showed that paired differences in WM lesion volume in T2-w images between patients injected with cladribine and those treated with placebo were not significant at baseline and became so at the month-6 and month-12 MRI scan (data not shown). The analysis of the proportions of patients showing persistence or disappearance of CELs at month-12 MRI favored the treated group.
Early studies in the 90s seem to suggest a positive effect of cladribine on measure of physical disability in chronic progressive MS patients. 44
Since clinical improvement was seen after one year, the study was discontinued as originally planned after 12 months. During months 12–24 of the study, patients who received placebo in the first year were administered with half the dosage of cladribine, while patients who received cladribine were treated with placebo. Drug was administered in week-long monthly courses. Patients continued to be evaluated monthly with the EDSS and SNRS scores and imaged every six months. This part of the study was carried in a non-blinded manner.
At the end of year-2, patients treated with cladribine, had a significant high effect in the EDSS and SNRS changes over time. Moreover, when defining worsening in the EDSS score as a gain by 0.5 to 1.5 and in SNRS as a gain of 10 to 15, it was seen that treated patients presented with significantly longer time to failure. MRI saw no group-differences seen in the volume of chronic lesions between treated and untreated patients. Conversely, the majority (95%) of the patients treated with cladribine the first year and placebo the second year were CEL-free at the end of the 24th month. The authors interpreted the finding as related to a carry-over phenomenon of the effect seen during the first year of therapy. Of the patients treated with placebo the first year and half-dose of cladribine the second year, 50% were CEL-free at the 24th month.
Year-2000: a large multicenter study in PP and SPMS narrows the efficacy of cladribine to CELs resolution
In a double-blind, parallel-group, placebo-controlled study 159 patients with progressive MS (70% SPMS and 30% PPMS) were randomly assigned to receive either placebo (n = 54) or cladribine 0.07 mg/kg/day for five consecutive days every four weeks for either two (n = 53) or six cycles (n = 52) (total dose, 0.7 mg/kg or 2.1 mg/kg, respectively), followed by placebo, for a total of eight cycles of sc injections.26,40,41 The study was comprehensive of a 4-week screening phase, a 1-year double-blind therapy phase, and a 6-year open extension. Primary outcome measure was mean change in EDSS score. To this end, on an assumed standard deviation of 1.7 for change from the baseline EDSS score, it was computed that a sample size of 50 patients per arm would allow detecting a difference of 1.0 in change from the baseline EDSS score between the cladribine, 2.1 mg/kg, and placebo groups while achieving a statistical power of 80% based and two-sided alpha of 0.05. Each patient underwent EDSS and SNRS assessments every other month and an MRI exam every six months during the 1-year double-blind phase. Subsequently, over the course of the first year of the post-double-blind follow-up phase, EDSS scores were measured at 3-month-interval whilst MRI scans were obtained twice (months 18 and 24). In addition to clinical measures, although not as primary outcome measures, a number of imaging metrics were computed and analyzed. Specifically, the novel aspect of this study compared to previous ones, was provided by the more extensive analysis of MRI metrics indicative of both acute (ie, CELs 26 ) and chronic disease (ie, WM lesion volume in T2-weighted image, 26 cBHs and brain atrophy).40,41
All the randomized patients terminated the study. The results indicated that during the 12-month double-blind phase and the subsequent 24 months, there were no group-differences in terms of clinical exacerbations, mean changes in EDSS and SNRS scores from baseline to final evaluation and time to progression to disability assessed by Kaplan-Meier estimate for all patients.
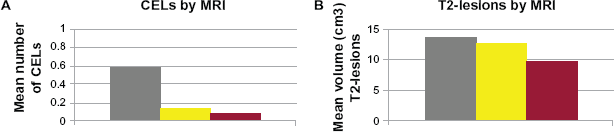
MRI data analysis related to CELs, showed the significant positive effect of cladribine. In particular, difference between the cladribine and placebo groups in the proportion of patients with CELs was statistically significant by month 6 and persisted as such until month 18 for the 0.7 mg/kg dose and through month 24 for the 2.1 mg/kg dose. As we report in Figure 5A and 5B, cumulatively, both treated groups had significantly lower mean number of CELs as well as mean volume of CELs and lesion in T2-w image. However, no treatment effect was seen in reducing brain atrophy progression and cBH accumulation (data not shown).
Patient Preference
From the standpoint of all the DMA-s currently available for use in MS, the question of “which one to use” will always be influenced by patient preferences in addition to the “hard data” that clinical trials and scientific publications offer. Whether to treat and what to treat with should be determined via a decision making process weighing all the pros and cons of the available treatments in each individual case. This process includes a well-trained and highly prepared neurologist familiar with all available treatment options, who should be willing and able to give appropriate education to patients and family members and help them understand the available avenues without any commercial or other perceived bias. This patient education and decision making process is often lengthy. All the available treatment options are only partially effective, none of them can effectively halt disease progression, and none have obvious properties that would result in increased tissue repair. 62
Patient preference is influenced by the interactions with the caregiver team, and recently, preference is also heavily influenced by abundant information available online through patient groups, websites of patient advocacy organizations, and of pharmaceutical companies. While patients may develop a preference based on these media channels, they often feel overwhelmed by the amount of contradictory information they encounter, and it is rare that patients would have a very clear preference over one drug or the other. Even when they do, the choice may have been influenced by erroneous interpretation of data available through public media outlets online. The decision making process must include a complete assessment of the actual MS type the patient has, with special attention to the inflammatory profile as assessed by MRI, which in addition to the clinical profile is the most informative paraclinical information in the decision making process.
From the standpoint of cladribine, the oral administration will certainly be a major “selling point” to many patients. This is coupled with the potentials for short-course dosing in cycles as opposed to continuous administration. The ease of administration will certainly be important to many patients and physicians, but continued observations and monitoring will be prudent with this new medication. The safety profile of this medication is clearly not as well established as it is for the currently available injectable DMA-s, and similarly to several past experiences with DMA-s, it is not unexpected that more or more obvious side effects will be observed during “real” clinical use compared to the controlled environment of clinical trials.
Place in Therapy
A major “gaping hole” in the armamentarium of the MS clinicians is how to meaningfully address the slow progressive phase of MS. While early studies at the Scripps Clinic suggested that cladribine may play a role in this patient population, the answer remains unclear.16,43,54,63
Evidence thus far suggests that cladribine is most effective in reducing the frequency of newly forming lesions, which is not at all unexpected given its overall mechanism of action. Therefore, it is expected that cladribine will be effective in MS patients with some disease activity. In addition, as already documented in the literature cladribine can be highly effective even at lower doses in the treatment of unusually active MS cases. 64 In this group of patients, this form of therapy may be more convenient and potentially less frequently associated with life threatening AE compared to currently used FDA approved treatments including mitoxantrone and natalizumab, although the exact safety profile especially for long term use remains unclear.
From the standpoint of clinical utility of new treatment approaches, in addition to the expected effectiveness and safety profile as established in clinical trials, other parameters are also of relevance. These include the AE profile and issues related to the actual administration of the drug (route, frequency, required monitoring). For its currently approved indication in hairy cell leukemia, cladribine can be given by iv infusion or subcutaneous injection. The same total doses are given regardless of route of administration, and the two routes have the same overall outcomes. 65 The total required doses are calculated by skin surface area in hematological applications. Of all the potential new oral MS agents in development, cladribine is the only therapy with the potential for short-course dosing, which is of importance from the standpoint of adherence to therapy and overall patient preference.
Since cladribine crosses the BBB, it may have effects even in disease stages that are not characterized by high frequency of CELs; in other words, it may work in the classically observed slowly progressive forms of SP and PPMS, where CELs are rarely observed. However, the studies by the MS group in Milan seem to contradict that. The length of observation period may not have been effective to capture this properly. It is also possible that neurodegeneration at these chronic, burnt out stages are no longer driven by the most focused targets of cladribine, CD4 lymphocytes.
Presently, given the limited knowledge and ongoing uncertainties related to its safety profile, defining an actual place in therapy for cladribrine would be premature. Notwithstanding this consideration, the most obvious clinical use of cladribine will be in highly active RRMS cases, and in those cases of progressive MS where new lesion formation as captured by post-contrast MRI is still observed. Both subgroups of patients should have been demonstrated to be refractory to commonly employed DMA-s.
Conclusions
MS is a treatable but incurable disease, which requires the patient to have chronic therapy, SC-, IVor IM-injected from once monthly to daily. Therapeutic regimens of this kind may severely hamper patients’ quality of life, ultimately interfering with patient adherence to prescribed therapy. The use of oral therapy has the potential to dramatically impact patient compliance. In addition, cladribine has the advantage to being administered in short-course dosing, hence reducing the challenge of frequent dose-regimen.
Nevertheless, at the present time, as seen also for other FDA approved DMA-s, much remains unknown regarding the actual potential of cladribine and its role beyond the control of CNS inflammation as captured by gadolinium enhancing lesions. One could argue that clinical trials longer than the ones performed thus far26,40–45 would have allowed for a better assessment of a potential protective effect. Short term pseudo-atrophy related to the potentially effective inhibition of inflammatory infiltration may have contributed to the negative effect seen in brain atrophy, for instance. 35 Hence, clinical trials designed and statistically powered with the specific aim of identifying the effect of the drug in affecting MRI measures of neurodegneration are advocated.
It is also desirable that studies with combined imaging and immunological outcome measures are conducted to investigate and clarify the effects of this DMA. Such studies should ultimately address the issue of whether a putative neuroprotective effect of cladribine is consequential on or independent from the reduction of inflammatory activity. In the study by Filippi and coauthors, 41 for instance, the significant treatment effects seen in cBHs were related to a decrease in mean volume and number of actively inflamed, newly forming CELs. Not unexpectedly, this effect segregated largely with the SPMS group, where inflammation is more commonly seen compared to PPMS. Evidence thus far does do not seem to ascribe a role to cladribine as a neuroprotective agent in MS. Relenting neurodegeneration and/or promoting repair are the most important challenges the current generation of clinical and basic scientists are mandated to overcome in an effort to more meaningfully influence the outcome of MS. Investigations of drug potential beyond BBB resolution will be warranted but will necessarily need to be postponed until studies assessing the actual safety profile of cladribine. The drug is indeed still awaiting approval from both the European EMA and the US FDA. It is expected that the data from on going clinical studies/and registries on safety profile will shed more light on the actual benefit/risk ratio of cladribine.
Disclosure Statements
Dr. Istvan Pirko has no affiliation of any kind with pharmaceutical companies. At the time of reviewing this manuscript, Dr. Francesca Bagnato works as consultant for reading and interpretation of scans in a six-month MRI initiative project with Biogenidec.
Neither Dr. Istvan Pirko nor Dr. Francesca Bagnato serve on speakers bureaus and their research is not sponsored by pharmaceutical companies.
No pharmaceutical company was involved in writing this manuscript and/or designing/planning its content. The paper solely expresses the opinion of the authors in accordance with the reviewers suggestions. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgments
Dr. Francesca Bagnato's contribution to this work was sustained by the intramural program of the NINDS, NIH.