
Abstract
Allergic rhinitis is a common, chronic medical condition affecting millions of people worldwide. Uncontrolled disease has been associated with impairments in quality of life and decreased economic productivity. Proper identification and control of relevant co-morbid conditions is essential for optimal rhinitis control. Management of allergic rhinitis includes identification of relevant allergens, education on avoidance measures, medications and immunotherapy. First-line therapy includes the use on an intranasal steroid. Other treatment options include oral or intranasal antihistamines, decongestants, leukotriene receptor antagonists, mast cell stabilizers or anticholinergic agents. Immunotherapy is an effective treatment option for refractory disease.
Introduction
Allergic rhinitis is an IgE-mediated, type 1 hypersensitivity disorder characterized by nasal congestion, rhinorrhea, pruritis and sneezing after exposure to indoor and outdoor aeroallergens. When accompanied by symptoms of ocular pruritis and tearing the disorder is referred to as allergic rhinoconjunctivitis. As with other atopic diseases the prevalence of allergic rhinitis has been increasing over the last several decades. 1
Allergic rhinitis has been shown to be associated with significant impairments in quality of life in patients of all ages.2,3 Specifically, children with allergic rhinitis perform poorly in school 4 and suffer from sleep disturbances. 5 Associations with attention deficit hyperactivity disorder in children with allergic rhinitis have also been found. 6 Adults with this disorder may suffer from sexual dysfunction, depression, poor quality of sleep and excessive daytime sleepiness.7–10 From an economic standpoint allergic rhinitis has been shown to have a large burden and impact. Estimates have found direct medical expenditures of $5.9 billion dollars yearly attributable to the disease. 11 That does not take into account the substantial impact of roughly 3.5 million works days and 2 million schools lost yearly. 12 Self-reported work productivity has been estimated to fall from 95% to 72% when patients are symptomatic. 13
Traditionally allergic rhinitis has been divided into seasonal allergic rhinitis and perennial allergic rhinitis. Generally patients who suffer from seasonal allergic rhinitis are sensitized to outdoor aeroallergens such as grass, tree and weed pollens while patients with perennial allergic rhinitis are sensitized to indoor allergens like house dust mite, mold and pets. Recently a newer classification scheme has been proposed per the Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines based on severity: mild intermittent, mild persistent, moderate/severe intermittent and moderate/severe persistent. Other types of rhinitis, which are not allergic, may co-exist in patients with allergic rhinitis (Table 1). 14
Types of rhinitis.
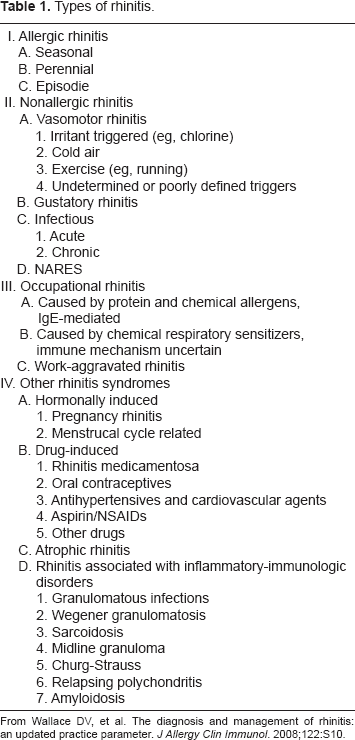
From Wallace DV, et al. The diagnosis and management of rhinitis: an updated practice parameter. J Allergy Clin Immunol. 2008;122:S10.
The diagnosis of allergic rhinitis requires a thorough history and physical examination. Sensitization to indoor or outdoor aeroallergens must be confirmed by skin prick/intradermal testing and/or in vitro testing. While skin prick testing is more sensitive than in vitro testing, certain situations (antihistamine use, dermographism, severe atopic dermatitis, inability to tolerate procedure) may preclude skin testing and make in vitro testing necessary. The presence of serum specific IgE to aeroallergens alone does not confirm the diagnosis of allergic rhinitis; rather it demonstrates sensitization. Patients must reproducibly demonstrate symptoms upon natural exposure to the allergen. Additional diagnostic testing which may be helpful in assessing response to therapy or evaluating for comorbidities includes rhinolaryngoscopy, rhinomanometry, acoustic rhinometry, nasal provocation testing, nasal smear for cytologic examination and computed tomography/magnetic resonance imaging. 15
The differential diagnosis for allergic rhinitis is extensive and includes vasomotor rhinitis, irritant rhinitis, occupational rhinitis, acute or chronic sinusitis, gustatory rhinitis, rhinitis medicamentosa, hormonal rhinitis, nasal polyposis, cerebrospinal fluid leak, non-allergic rhinitis with eosinpholia (NARES), inflammatory/granulomatous disorders (Wegener's granulomatosis, sarcoidosis, Churg-Strauss syndrome) and drug-induced rhinitis (Table 2). Proper treatment of these disorders is necessary for optimal rhinitis management and vice versa.
Differential diagnosis of rhinitis.
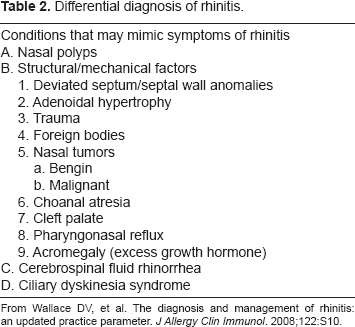
From Wallace DV, et al. The diagnosis and management of rhinitis: an updated practice parameter. J Allergy Clin Immunol. 2008;122:S10.
Patients with simple manifestations usually can be managed effectively in primary care. Those with atypical presentations, comorbid conditions, severe impairment of their quality of life, inadequate responses to initial management, and clear involvement of aeroallergens requiring immunotherapy will benefit from specialty referral. 15
Treatment
Numerous factors should be addressed when considering pharmacologic therapy for patients with allergic rhinitis. These include patient age, side effect profile, cost of therapy, previous medication trials and response and patient preference. Three main treatment categories include avoidance measures, medications and immunotherapy.
Avoidance Measures
Outdoor allergens
While complete avoidance is not practical for outdoor aeroallergens, certain steps can be taken to help minimize exposure. Closing doors and windows during pollen season can help reduce contact with outdoor aeroallergens. Vents should remain closed in cars and homes when air conditioning is being used. Thorough washing and changing clothes when coming indoors may help remove allergens from one's body, thereby reducing exposure.16,17 Sensitive patients may want to track pollen counts and limit outdoor exposure when such counts are elevated. Some investigators have even recommended that highly sensitive patients consider wearing facemasks when going outdoors during peak pollen season. 18
Indoor allergens
On the other hand avoidance measures targeting indoor aeroallergens are more practical to implement and have been studied far more extensively. While they have been shown to be cost-effective, the significance and benefit of each measure depends on a variety of factors as we will see below. 19 The clinician should also keep in mind that while certain environmental modifications may be beneficial, some patients may not comply because of the cost (monetary, emotional) associated with the proposed changes. For example, some patients may refuse to remove their cat from their residence even though they are exquisitely sensitive to cat dander.
House dust mites
Methods to limit exposure to house dust mites include protective mattress and pillow coverings, reducing humidity below 50%, regular washing of bedding in hot water, treating carpet with acarides or removing carpet altogether, removing stuffed animals from the bedroom and regular vacuuming with a high-efficiency particular air filter. Investigators have shown 20 that decreasing exposure to indoor allergens (dust mite and cockroach) in children with allergic asthma leads to improved symptom control. Other studies in allergic asthmatics, however, failed to show similar results. A recent Cochrane review found that the use of acarides and extensive bedroom control measures provided some benefit in improving rhinitis symptoms.21,22 The authors did cite the lack of robust and well-done trials as the reason for not being able to give definitive recommendations on other environmental control measures. In our practice we routinely advise patients allergic to house dust mites to use protective encasings on their mattresses, pillows and box springs. Additionally we instruct them to wash their bedding regularly in hot water. If financially feasible we also recommend replacing carpet in the bedroom with tile or hardwood.
Domestic pets
Domestic pets may be the most common source of indoor allergens in the United States. 23 While the best control measure is removing the pet from the household altogether, many patients are emotionally attached to their pets and refuse to see this as a plausible option. Keeping pets out of the bedroom or exclusively outdoors may reduce allergen exposure. Of note studies have revealed that after removing cats from a residence levels of the major cat allergen can persist for several months. 24 Even cat-allergic children who live in pet-free homes have been shown to develop asthma symptoms upon indirect exposure to cat allergen in schools. 25 The level of cat antigen found in pet-free homes has been shown to cause upper and lower airway symptoms in cat allergic patients as well. 26 Another study investigating the effects of HEPA filters, exclusion of cat from the bedroom and mattress and pillow covers demonstrated reduced levels of cat allergen without improving asthma and rhinitis control. 27 While frequent washing of cats may decrease airborne allergen levels, this finding has not been shown in all studies.28,29 Washing dogs twice a week has been shown to reduce levels of the major dog allergen. 30 For the majority of our patients we encourage them to keep pets outdoors if possible and out of the bedroom altogether. In patients with severe allergic rhinitis or moderate to severe persistent asthma who are cat allergic we ask that they remove pets from the residence altogether. If they cannot part with their pets we generally recommend initiating immunotherapy as our patients have found this to be an effective treatment option.
Cockroaches
Cockroaches are another potential indoor source of aeroallergens and they play an especially important role in inner-city children with allergic diseases. A study of inner-city children with asthma found that those who were sensitized and exposed to high levels of cockroach allergen had more hospitalizations, missed more days of school, suffered more from sleep disturbances and had more unscheduled medical visits than unsensitized and unexposed children. 31 Interestingly, similar patterns were not seen in children sensitized and exposed to high levels of cat and dust mite allergen. Given the difficult socio-economic conditions that many inner-city children live in, implementing control measures to remove cockroaches may be difficult. Even in the absence of these conditions removing cockroach exposure can be challenging and time-intensive. Investigators who looked at the effect of professional extermination and cleaning on cockroach allergen levels found only a transient decrease which was short-lived. 32 A recent taskforce put forth recommendations aimed at reducing allergen exposure. These include using bait and traps, removing potential food sources and eliminating cockroach debris. 33 In our practice we recommend that patients elicit professional pest control assistance in dealing with cockroach infestation.
Pharmacotherapy
Antihistamines
Historically antihistamines were classified according to their structural classes: alkylamines, ethanolamines, ethylenediamines, phenothiazines, piperidines and piperazines. More commonly these agents are divided into first-generation, or sedating antihistamines and second-generation, or nonsedating antihistamines. First-generation antihistamines, including diphenhydramine, chlorpheniramine, clemastine fumarate and bropheniramine, have been used to treat allergic rhinitis for decades. These have been largely supplanted by the second-generation drugs including cetirizine, levocetirizine, loratadine, desloratadine and fexofenadine. Antihistamines are available as single agents or may be combined with other agents.
Mechanism of action
Previously medications in this class were thought to act by directly blocking the H1-receptor. Recently, however, it has been shown that these medications work not as antagonists but rather as inverse agonists. 34 Thus they exert their function by stabilizing the inactive form of the histamine receptor. 35 Additionally, researchers have demonstrated that the first-generation antihistamines chlorpheniramine and diphenhydramine may induce eosinophil apoptosis. First generation antihistamines are lipophilic. 36 Thus they have the ability to cross the blood-brain barrier and block the neurotransmitter effect of histamine in the central nervous system. 37 Second generation antihistamines, on the other hand, do not cross the blood-brain barrier as readily. Thus they are not as sedating as the older, first generation drugs.
Clinical studies
Numerous clinical trials examining the efficacy of antihistamines for allergic rhinitis have been published to date.38–40 However, there have been few studies comparing first and second generation H1-anthistamines. 41 While these medications can be used as needed or daily for the treatment of allergic rhinitis, daily use has been shown more effective than on demand treatment. 42 Numerous studies have shown superiority of intranasal corticosteroids when compared to antihistamines.43–45
Safety
First generation, sedating antihistamines have been shown to cause impairment in driving in adults and the learning ability of children.46–48 Additionally the sedative effects of these medications have been shown to persist during the day even with bedtime use. 49 In addition to their antihistamine effects, first generation antihistamines also have anticholinergic properties which may be particularly troublesome for elderly patients. Their use can lead to urinary retention, dry mucous membranes, confusion, constipation and blurry vision. Recently over-the-counter “cold” medicines which contain antihistamines have been implicated in deaths in young children. 50
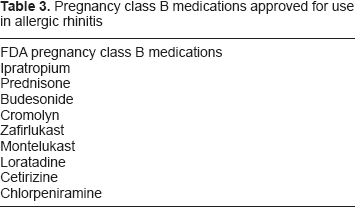
On the other hand, second generation H1-antihistamines have a more favorable side-effect profile and tend to cause less sedation. 51 Cetirizine is often preferred because of greater potency and duration, but it does have a greater incidence of sedation than fexofenadine. 40 Although less common than with the first generation class of antihistamines, anticholinergic effects have been reported in this class as well. 52 A variety of antihistamines have been graded as pregnancy class B (Table 3).
Pregnancy class B medications approved for use in allergic rhinitis
Intranasal Steroids
Intranasal corticosteroids are the most effective medication for the treatment allergic rhinitis. This class of medication includes beclomethasone, budesonide, ciclesonide, flunisolide, fluticasonefuroate, fluticasone proprionate and mometasone furoate.
Mechanism of action
Corticosteroids exert their function by binding to intracellular glucocorticoid receptors found in the cytoplasm of inflammatory cells. This complex then enters the nucleus and both suppresses the activation of inflammatory genes and modifies the expression of numerous inflammatory mediators, enzymes, cytokines and chemokines. 53 Intranasal corticosteroids have been shown to decrease the numbers of eosinophils, Langerhans cells, T cells, mast cells and basophils locally in the nasal mucosal tissue. 54
Clinical studies
A systematic review of randomized controlled trials found intranasal corticosteroids to be superior to oral H1-antihistamines in providing greater relief of sneezing, nasal itching, nasal blockage, postnasal drip and total nasal symptoms. 55 A double-blinded study comparing intranasal fluticasone propionate to monteleukast, monteleukast and loratadine or placebo found intranasal fluticasone propionate to be superior in reducing nasal eosinophilic inflammation and improving nasal symptoms. 56 Another study found as-needed intranasal fluticasone propionate superior to as-needed loratadine in improving Rhinconjunctivitis Quality of Life Questionnaire (RQLQ) and reducing nasal eosinophilic inflammation. 57 To our knowledge, no studies to date have shown one medication to be consistently better than another.58–60
Safety
Common side effects of intranasal corticosteroid use include local irritation, drying and burning. Medications containing alcohol tend to be more irritating than aqueous ones. Epistaxis can be seen in up to 10% of patients using this class of medication. 61 Rarely nasal septum perforation has been seen. This is thought to be the result of improper technique where the medication is directly applied towards the nasal septum. Even with long-term use of nasal steroids, biopsies have failed to demonstrate any detrimental effects of the nasal mucosa. 62
Given the concern of chronic steroid use and its well-known side effects, various studies have examined the effect of intranasal corticosteroid use in both children and adults. Specifically studies have looked at the effect of intranasal corticosteroid use on bone density, the hypothalamic-pituitary-adrenal axis, and ocular pressure.63–67 These studies have failed to show any consistent evidence that chronic intranasal corticosteroid use is associated with these detrimental effects. One randomized, double-blind, placebo-controlled study examining the use of beclomethasone diproprionate in children with perennial allergic rhinitis found a small but statistically significant slow in growth rate in the treatment group. 68 However other studies have failed to reproduce this effect.69–71 Of note, these side effects of corticosteroids can be dose-dependent. Thus care must be taken when using these medications in patients who receive steroids in other preparations for associated disorders (atopic dermatitis, asthma, chronic obstructive pulmonary disease, etc).
Leukotriene Receptor Antagonists (LTRA)
Montelukast, approved for the treatment of allergic rhinitis, works to mitigate the effect of cysteinyl leukotrienes by blocking the leukotriene receptor CystLT1. Cysteinyl leukotrienes have been shown to play an important role mediating both the early and late phase in allergic rhinitis. 72
Mechanism of action
The cysteinyl leukotrienes LTC4, LTD4 and LTE4 have been shown to play a prominent role in promoting local inflammation and causing symptoms of allergic rhinitis. 73 Blocking their effects through medications has been shown to improve symptoms of allergic rhinitis and asthma.74,75
Clinical studies
Montelukast has been shown to be effective in the treatment of allergic rhinitis.76,77 Additionally it has been approved for use in treating allergic asthma, thus making it a good choice for treating patients with both diseases. 78 A recent study comparing fexofenadine alone to fexofenadine with montelukast demonstrated the combination of the two to be superior to fexofenadine alone in both objective and subjective outcomes. 79 However not all data regarding montelukast is favorable. A recent meta-analysis of 20 studies found both intranasal corticosteroids and antihistamines to be superior to montelukast in the treatment of allergic rhinitis. 80 Another systematic review and meta-analysis found leukotriene receptor antagonists to be superior to placebo but inferior to intranasal corticosteroids in the treatment of allergic rhinitis. 81
Safety
Common side effects include headaches, elevated liver transaminases, dizziness, angioedema, rash and fatigue. There has been some concern about an association of montelukast use with depression and suicidal thoughts. A recent review compared the frequency of suicidal (completed, attempted, ideation) adverse events in over 20,000 patients receiving montelukast to over 9000 placebo and 8000 active control patients found no difference in the incidence of these events between the 3 groups. 82 Other reports have failed to show a link as well.83,84 Thus a joint report from the American Academy of Allergy, Asthma and Immunology and the American College of Allergy, Asthma and Immunology stated that patients should continue taking the medication unless they experience suicidal thoughts or exhibit suicidal behavior. 85 If so they should immediately consult their physician. Additionally there have been concerns and reports of leukotriene receptor antagonist use “unmasking” underlying Churg-Strauss syndrome in asthmatics. 86 Whether this association is a direct causal effect, however, is still not clear. 87 Montelukast is pregnancy risk category B.
Intranasal Antihistamines
Azelastine and olopatadine are topical nasal antihistamines which have been approved for the treatment of allergic rhinitis.
Mechanism of action
Similar to oral anthistamines, topical nasal antihistamines act locally to mitigate the effects of histamine on the local nasal mucosal tissue. Additionally, azelastine has been found to have mast-cell stabilizing and anti-inflammatory properties. 88 Intranasal antihistamines have a rapid onset of action (15 minutes), making them candidates to use for as needed and rapid relief of allergic rhinitis symptoms. 89
Clinical studies
Intranasal antihistamines have been shown to be effective in treating patients with seasonal and perennial allergic rhinitis. A recent meta-analysis found azelastine to be more effective than placebo in treating allergic rhinitis. 90 Additionally the same review found a trend favoring treatment with azelastine when compared to oral anthistamines as monotherapy. Another randomized-controlled trial comparing azelastine to cetirizine found that azelastine significantly improved Rhinoconjunctivitis Quality of Life Questionnaire scores. 91
While some trials have shown azelastine to be superior to intranasal corticosteroids in providing relief of specific allergic rhinitis symptoms, a meta-analysis of 9 studies including over 640 patients found intranasal antihistamines to be inferior to intranasal corticosteroids.92,93 No difference was found regarding relief of ocular symptoms. Studies have shown combination therapy with intranasal antihistamine and intranasal corticosteroid to be more effective than either agent alone.94,95
Safety
Intranasal antihistamines have been associated with local irritation, burning and headaches. Additionally, azelastine use has been associated with a bitter and metallic taste. In an attempt to counteract this affect a new formulation containing sucralose and sorbitol has been made.
Oral Decongestants
Phenylephrine, pseudoephedrine and phenylpropanolamine are alpha-adrenergic agonists used to relieve symptoms of nasal congestion.
Mechanism of action
These medications exert their action through their alpha-adrenergic properties. They act as vasoconstrictors and provide local relief by reducing nasal congestion.
Clinical studies
A randomized, double-blind, placebo-controlled trial of 874 patients demonstrated that pseudoephendrine plus loratadine was superior to either medication alone or placebo in controlling symptoms of seasonal allergic rhinitis. 96 A similar trial examining the efficacy and safety of an extended release formulation of the two found the combination to be superior to the individual components in treating seasonal allergic rhinitis. 97
Safety
The potential of significant side effects have limited the use of these medications in allergic rhinitis. Common effects include hypertension, insomnia, irritability, headache, tremor and palpitations. These medications should be used with caution in patients with hypertension, hyperthyroidism and coronary artery disease due to their sympathomimetic properties. 98 The FDA has recalled products containing phenylpropanolamine due to concerns of hemorrhagic strokes. 99 Additionally the use of pseudoephedrine has been restricted because of its use in the production of methamphetamines. Given the possible link between oral decongestants and death in infants, the use of these agents in children under the age of 6 has been greatly restricted. 100
Topical Decongestants
Topical decongestants, including phenylephrine, oxymetazoline, xylometazoline and naphazoline may be used in allergic rhinitis to relieve symptoms of nasal congestion.
Mechanism of action
Medications in this class are adrenergic agonist agents that exert their effects on alpha-1 and alpha-2 receptors locally in the nasal tissue. Their use leads to vasoconstriction of local blood vessels, resulting in improvement of nasal congestion and rhinorrhea.
Clinical studies
One study found intranasal xylometazoline to be superior to mometasone furoate in treating allergic rhinitis. 101 Another trial recently showed the combination of oxymetazoline and fluticasone furoate to be more effective than either agent alone in improving symptoms scores in patients with perennial allergic rhinitis. 102 Interestingly there was no evidence of rhinitis medicamentosa at the end of the 4 week trial.
Safety
Topical decongestants may be used for up to three days the relief of significant nasal congestion/obstruction, especially if the congestion is severe enough to preclude the use of topical nasal medications. Use for longer periods may lead to rebound nasal congestion and rhinitis medicamentosa. Additionally, these medications may lead to local stinging/burning, dryness or sneezing. Because these medications are applied topically they have less absorption and systemic side effects than oral decongestants. Nevertheless their use is not without risk. As stated above, prolonged use is associated with rhinitis medicamentosa. Reports linking these medications to anterior ischemic optic neuropathy, branch retinal artery occlusion and stroke have been published.103–105 Concurrent use with monoamine oxidase inhibitors is prohibited.
Oral Steroids
Systemic steroids are not routinely indicated for the management of allergic rhinitis. In certain circumstances, however, they may be used in short courses to provide relief of severe symptoms. 106 A double-blind study comparing oral prednisone (7.5 mg daily) to a depot injection of betamethasone found no significant difference in symptoms score or nasal peak flow between the 2 groups after 3 weeks of treatment. 107 However, the oral prednisone group had significant adrenal gland suppression in contrast to the depot injection group. Therefore even a few weeks of oral steroids may be associated with systemic side effects, thus limiting their routine use in allergic rhinitis. In our practice we do not administer intramuscular or depot steroids for the management of allergic rhinitis, and we rarely prescribe oral steroids for greater than 5 days in duration.
Mast cell stabilizers
Mechanism of action
Cromolyn sodium acts by stabilizing the membrane of mast cells and preventing local mediator release in response to allergen challenge. 108
Clinical studies
Intranasal cromolyn sodium has been shown to be effective in the treatment of allergic rhinitis. 109 However, other studies have shown intranasal corticosteroids and intranasal antihistamines to be more effective.110–113 Unlike other therapeutic options, intranasal cromolyn sodium is not very effective for as-needed or on-demand therapy. This is because cromolyn stabilizes the mast cell membrane prior to allergen challenge. Thus, once the patient inhaled the allergen and the mast cell degranulates, cromolyn is no longer effective in treating symptoms. Additionally, intranasal cromolyn sodium must be administered frequently throughout the day, making compliance difficult when compared to once-a-day medications.
Safety
Cromolyn sodium has been found to be very safe. Known side effects include local stinging or irritation, unpleasant taste, headache and sneezing. Intranasal cromolyn sodium is pregnancy class B.
Anticholinergic Agents
Ipratropium bromide is a nasal anticholinergic medication used to treat symptoms of allergic rhinitis.
Mechanism of action
The autonomic nervous system, via parasympathetic nerves, innervates the nasal mucosa. Acetylcholine acts upon M1 and M3 receptors in the nasal mucosa to stimulate mucus secretion from serous and seromucous glands. Ipratropium bromide acts locally to block the effects of acetylcholine.
Clinical studies
Ipratropium bromide has been shown to be very effective in treating cases of allergic rhinitis in which rhinorrhea is the predominant symptom. Specifically it has been shown to improve rhinorrhea in children and adults.114–117 Ipratroprium bromide has also been shown to be effective when combined with an intranasal corticosteroid. 118
Safety
Because it is a quaternary amine, ipratropium has less absorption and systemic side effects than tertiary anticholinergic amines. In a clinical trial assessing the efficacy and safety of ipratropium bromide nasal spray in children with the common cold, its use was associated with higher rates of blood-tinged mucus and nasal dryness than seen in placebo. 119
Omalizumab
Omalizumab is a recombinant humanized monoclonal antibody which binds to circulating IgE, thereby preventing it from interacting with mast cells and basophils. It has been approved for the treatment of allergic asthma in adults and children over 12 who are not optimally controlled with inhaled corticosteroids and have proven sensitivity to at least one perennial aeroallergen.
Mechanism of action
Omalizumab works by binding to IgE and clearing it from the circulation. Omalizumab is specific for IgE and prevents it from binding to mast cells and basophils, which play integral rolls in mediating the symptoms of allergic rhinitis. Additionally omalizumab has been shown to decrease the expression of the Fc-epsilon Receptor-I to which IgE binds on both mast cells and basophils.120,121
Clinical studies
Omalizumab has been shown to be efficacious and safe in treating children with allergic rhinitis. 122 Additionally it has been shown to be effective in treating adolescents and adults with allergic rhinitis.123–125 Despite the data from these trials and others, omalizumab is currently not approved for the treatment of allergic rhinitis. This is partly due to the high costs associated with this treatment.
Safety
In addition to local irritation at the site of administration, Omalizumab has been associated with anaphylactic reactions. 126 Additionally there have been some recent concerns regarding the use of omalizumab and possible association with cardiovascular disease and malignancy.
Surgery
The vast majority of patients with allergic rhinitis can be well-managed medically. Patients with marked inferior turbinate hypertrophy, significant nasal septal deviation or refractory nasal polyposis may benefit from referral to an otolaryngologist for surgical evaluation.
Traditional Subcutaneous Immunotherapy
Subcutaneous Immunotherapy, or SCIT, involves administering gradually increasing amounts of allergen in an attempt to desensitize the patient.
Mechanism of action
While the exact mechanisms by which immunotherapy leads to desensitization and tolerance are still being elucidated, over the last several years there has been a substantial amount of research dedicated to this field. A detailed review of the proposed immunologic changes and mechanisms associated with allergen specific immunotherapy are beyond the scope of this review. We will, however, highlight important themes that may of be interest to the practicing clinician.
Within days to weeks of initiating allergy immunotherapy there is an increase in CD4+CD25+ regulatory T cells. 127 These cells have been shown to secrete the inhibitory cytokines TGF-Beta and IL-10, whose anti-inflammatory effects are thought to play a key role in immunotherapy. 128 A subsequent phenomenon is the deviation away from a Th2 response towards a Th1 response.129,130 Th1 cells tend to blunt allergic reactions while Th2 facilitate it. This increase in Th1 lymphocytes is correlated with protection against allergic rhinitis.
Investigators have revealed that early on in immunotherapy there is an increase in specific IgE levels followed by a fall after a few years. 131 Interestingly patients may clinically respond to immunotherapy even as their specific IgE levels rise early on. Additionally increases in specific IgG have been seen with immunotherapy. 132 These “blocking antibodies” have been shown to inhibit the binding of IgE to B cells and thus preventing allergen processing by antigen-presenting cells.133,134 However the elevated allergen-specific IgG levels do not always correlate with the improvement of symptoms.
Clinical efficacy
Numerous double-blind, randomized, placebo-controlled trials have shown SCIT to be effective in the treatment of allergic rhinitis.135–137 A recent Cochrane review of 51 randomized, double-blind, placebo controlled trials of SCIT in allergic rhinitis found statistically significant improvement in both medication use and symptom scores. 138
Systematic reviews have also show SCIT to be beneficial in patients with allergic conjunctivitis and allergic asthma.139,140
Investigators have shown persistent benefit even 12 years after discontinuing immunotherapy in children. 141 Specifically these children had lower symptom and medications scores in addition to a reduction in the onset of new sensitization when compared to controls. Other studies have shown similar results with SCIT preventing new sensitizations in children monosensitized to aeroallergens.142,143 Additionally 3 years of SCIT has been shown to prevent the development of asthma in children with allergic rhinitis. 144
Prior to initiating immunotherapy one needs to demonstrate elevated levels of specific IgE, either by skin prick testing or in vitro testing. Additionally patients must demonstrate symptoms of allergic rhinitis after exposure to these allergens. Immunotherapy is indicated for patients who do not wish to take daily medication, who have persistence of symptoms despite adequate medication use, or who cannot tolerate side effects (sedation with antihistamines, epistaxis with intranasal corticosteroids) of medication. Despite the perceived high costs associated with SCIT, data has consistently shown immunotherapy to be more cost-effective when compared to conventional therapy.145–147
At this time different dosing schedules exist (conventional, cluster, rush and ultrarush). While cluster, rush and ultrarush protocols can build patients up to maintenance levels more quickly, they are associated with more systemic reactions.
Side effects
In general SCIT is a safe and effective method for treating, and potentially curing, allergic rhinitis. Common side effects include local reactions at the site of injection. One report found that 71% of patients undergoing SCIT had local reactions. Systemic reactions occur much less frequently. 148 Two recent reports found the rate of systemic reactions during SCIT to be 0.1% to 0.2% per injection.149,150 While fatalities have been reported they are very rare. Large surveys have found the fatality rate to be 1 to 2 in 2.5 million injections.151,152 Risk factors for fatalities during immunotherapy include poorly controlled asthma, use of a new vial, concurrent beta-blocker use and dosing errors. 153
Other Forms of Immunotherapy
SL Immunotherapy
An alternative form of immunotherapy is to administer the allergen sublingually. This permits most of the treatment to be done at home with daily administration of antigen.
Mechanism of action
In sublingual immunotherapy the antigen is taken daily, held under the tongue for several minutes and then swallowed. It is believed that dendritic cells in the oral cavity take in the allergen and present it to lymphocytes centrally. 154 Studies examining the immunologic changes that occur with SLIT have demonstrated changes similar to those seen with SCIT. Specifically increases in allergen-specific IgG4 and a blunting of the allergen specific IgE response have been reported.155,156 Other studies have shown an increase in suppressor regulatory T cells. 157
Clinical studies
A variety of randomized, double-blinded, placebo-controlled trials have shown SLIT to be efficacious in the management of allergic rhinitis. A Cochrane review of 49 randomized, double-blind, placebo controlled trials of SLIT in adults and children found SLIT to be a safe and effective treatment of allergic rhinitis. 158 Currently SLIT is being marketed and used in a variety of European countries. Practice guideline documents list SLIT as a viable and effective alternative to SCIT.159,160
A randomized, placebo-controlled, double-blind and double-dummy trial compared SLIT to SCIT in 71 adult patients with birch pollen allergy found no statistically significant difference in symptom and medication scores between the two groups. 161
While not yet FDA approved, recently investigators have been examining the use of SLIT in treating patients in the US. Recently a phase 1 trial looking at the safety and tolerability of cat hair, ragweed, house dust mite and timothy grass extracts in adults with allergic rhinitis found maximal dosing to be well tolerated. 162 Optimal dose for maintenance therapy, duration of treatment and efficacy of combination therapy with multiple aeroallergens need to be further clarified.
The vast majority of SLIT trials have evaluated a single allergen. However, the practice in the United States is to administer multiple allergens to patients during SCIT. It cannot be concluded that giving multiple allergens sublingually would be effective. For the present this route of immunotherapy should be considered experimental.
Safety
Common side effects with SLIT include local oral pruritis or swelling, throat irritation and gastrointestinal discomfort. In general SLIT is accepted as having a better safety profile than SCIT. 163 A recent Cochrane database review concluded that SLIT was a safe and efficacious treatment for patients with allergic rhinitis. 164 Another recent review examining the safety of SLIT in 60 studies did not find any serious systemic side effects or anaphylaxis and there were no reports of epinephrine administration. 165 However there are case reports of patients who have had anaphylaxis associated with SLIT administration, thus it is not without risk.166,167 Additionally the safety of SLIT administration with multiple concurrent antigens has not been widely examined.
Approaching a patient
After a thorough history and physical examination each patient should be assessed for both allergic sensitization to relevant indoor and outdoor aeroallergens in addition to co-morbidities. Proper therapy for control and resolution of a patient's symptoms often requires treatment of both allergic rhinitis and underlying co-morbidities which may exist (nasal polyposis, chronic sinusitis). After skin test or in vitro IgE testing results are available we review treatment options with our patients.
First, we discuss with our patients the difference between seasonal and perennial allergens and how this difference impacts their life. For example a patient who is only allergic to ragweed needs to vigilant during the fall season, while a patient who is allergic to house dust mite and indoor molds may experience symptoms year-round. Second, we discuss relevant avoidance measures based upon their testing results. This is followed by a thorough discussion of medication use. We carefully review all medications that the patient has tried in the past. We discuss the efficacy, cost, tolerability and side effects experienced with each individual medication. Based upon these factors we decide how to treat a patient.
First-line therapy generally includes the use of a nasal steroid. For patients with marked or complete nasal obstruction we frequently recommend 3 days of oxymetazoline or a short prednisone “burst”. This allows for quick resolution of obstruction and permits proper administration and deposition of the nasal steroid onto the nasal mucosa. For refractory symptoms we will add an oral antihistamine. We prefer cetirizine as we have found this to be affordable, well-tolerated and efficacious. If patients cannot tolerate a nasal steroid because of side effects or lack of efficacy we will then consider either using montelukast or an intranasal antihistamine. For patients who have profound rhinorrhea as a major symptom we will also use intranasal ipratropium.
We generally reevaluate our patients for response to therapy in one to two months. If they continue to have symptoms or cannot tolerate medications we will discuss initiating subcutaneous immunotherapy. While patients may require treatment with medications early in their immunotherapy course, we have found that the majority of patients are able to greatly reduce or discontinue medication use once they build up to maintenance immunotherapy dosing.
Most of these recommendations can be provided in primary care. With increasingly complex patients who have significant impairment, a specialist with graduate training in allergy-immunology can provide the patient considerable assistance in optimizing their management long term. 15
Conclusion
Allergic rhinitis is the most common chronic disease. Therefore effective management in primary care is essential, and this has been outlined above. Frequently there is a fundamental need for specialty referral for assistance in diagnosing complex patients, identifying comorbid conditions, and in planning safe and effective treatment. 15 Generally significant improvements can be achieved with avoidance measures, safe and effective drugs, and well planned allergen immunotherapy.
Disclosure
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.