
Abstract
For decades allopurinol has been used as a xanthine oxidase inhibitor for treatment of hyperuricemia and gout. Although effective in many patients, some experience sensitivity to the drug. In some cases, this sensitivity may lead to allopurinol hypersensitivity disorder, which if untreated can be fatal. Recently the Food and Drug Administration has approved the use of febuxostat as an alternative therapy for hyperuricemia and gout. Febuxostat is a new xanthine oxidase inhibitor, but is not purine based and therefore decreases adverse reactions due to patient sensitivity. This review is a comprehensive look at the background of hyperuricemia and gout treatment with allopurinol compared to recent clinical studies with febuxostat. Each clinical study is evaluated and summarized, identifying the advances in treatment that have been made as well as the concerns that still exist with either treatment.
Introduction
Over half a century after the development of allopurinol, it continues to be the first line drug in the treatment of hyperuricemia and gout. Although patient sensitivities to the drug, most commonly skin rashes, are of concern, only an estimated 0.1% of the patients treated with allopurinol develop the potentially life threatening condition known as allopurinol hypersensitivity syndrome (AHS). 1 It is for these patients, in addition to those with renal impairment, organ transplants, or hepatic failure, that the development of a new xanthine oxidase inhibitor was undertaken. Now, for the first time since the arrival of allopurinol in 1946 and trials with the alternative purine-based structure, a non-purine based xanthine oxidase inhibitor, febuxostat, has been approved by the Food and Drug Administration (FDA). Febuxostat is indicated for patients with hyperuricemia and gout that have exhibited sensitivities to allopurinol. This review presents the pathophysiology of hyperuricemia and gout and discusses the use of allopurinol and febuxostat as treatments of these metabolic disorders.
Hyperuricemia is defined as high levels of uric acid in the blood. Although often patients with hyperuricemia develop gouty arthritis, some patients live decades with elevated serum uric acid levels without ever developing the condition.2,3 In most cases where elevated serum uric acid is noted without inflammatory response, patients are asymptomatic and treatment is not advised. However, in the cases where painful inflammation around the crystallized urate in the joint has already formed, the patient is generally diagnosed with gout and treatment is indicated. Gout, resulting from crystallized monosodium urate in the joints, is an inflammatory arthritic disease with growing incidence. 4 Gout was originally associated with individuals consuming a high fat diet, purine rich foods and a relatively inactive lifestyle, but it is now considered a metabolic disorder and is linked to a variety of other disease states. In recent years the condition has been implicated in conditions such as hypertension, obesity, kidney disease, hyperlipidemia, metabolic syndrome and cardiovascular disease.1,2,4–22 Most patients exhibit elevated serum uric acid levels for years before symptoms arise. Gout is most commonly observed in males over fifty years of age.
Although the physical accumulation of sodium urate in the joints is the definitive cause of gouty arthritis, variable conditions lead to the increase in serum uric acid beyond the 0.42 mmol/L (6.8 mg/dL) limit of solubility.4,23 The causes of increased serum uric acid levels fall into two categories: decreased renal clearance and increased uric acid production. The decrease in renal clearance of uric acid accounts for 90% of the known cases of gout.6,24 The primary cause of impaired renal clearance of uric acid is idiopathic, but is likely the result of an inherited kidney disease. Hypertension, chronic renal failure, sarcoidosis, preeclampsia, and metabolic abnormalities offer secondary causes for renal impairment and therefore decrease uric acid clearance.25–30 Secondary cause of hyperuricemia include drugs such as cyclosporine, pyranzinamide, levodopa, or tacrolimus which have a tendency to decrease renal clearance of urate due to changes in nephron handling. Other, commonly used drugs have been identified as potentially causing decreased uric acid excretion including diuretics, ethanol, low-dose aspirin, and laxatives (when used excessively).31–41 Decreased uric acid excretion is particularly troublesome for gout patients treated with allopurinol, as this agent has been associated with renal impairment during treatment.
Although allopurinol (categorized as a xanthine oxidase inhibitor, XOi) is recognized as a first line drug of choice for gout, several other drug categories are and have been used for several years. These alternative approaches include anti-inflammatory drugs and uricosuric agents. The anti-inflammatory drugs include both non-steroidal compounds (NSAIDS) as well as steroid based therapy. In fact during acute gout attacks, the primary goal is control of inflammation, rather than a decrease in the serum uric acid levels. Uric acid clearing drugs, such as probenecid, are often co-prescribed with an anti-inflammatory during a flare in gouty arthritis. This combination therapy is particularly common for patients with a known impaired uric acid clearance, corresponding to approximately 9 out of 10 gout patients.6,32,34,35,42
Currently, many renal impaired patients are treated prophylactically with XOis such as allopurinol to prevent recurring gout related joint attacks. This method, although often effective, should be carefully considered as these patients are already likely suffering some degree of renal impairment. Although allopurinol, or more specifically its metabolite oxypurinol, is not readily excreted by patients with renal failure, many studies have been completed that carefully address dosing changes for patients with deficiencies in renal function.9,43–51 Despite the well characterized studies of allopurinol therapy, many patients did not receive the optimal dose as determined via titration for that particular patient; this discrepancy extends to both ends of the spectrum ranging from low ineffective doses chosen due to concern over renal clearance to excessively high doses given the patient's “normal” creatinine level.51–53
As certain therapeutics are chosen based on the decrease in clearance of uric acid, XOi drugs such as allopurinol or the newer febuxostat are typically selected for patients whose gout is likely caused by an increase in uric acid production. Unfortunately the primary cause of increased uric acid production is often unknown or results from a number of inherited enzyme deficiencies such as hypoxanthine-guanine phosphoribosyl transferat (HGPRT) deficiency, phosphoribosyl transferase (PPT) deficiency, or glucose-6-phosphate phosphotase deficiency. Oftentimes even if an enzyme defect is suspected, tests are not completed to identify which defect is exhibited. These tests are especially neglected if the patients have been responsive to allopurinol therapy without side effects. Use of the XOi's for reduction of uric acid is appropriate in most cases where the patients have normal renal function provided that the accumulation of uric acid is not related to excessive purine nucleotide degradation from unknown disease states.
The goal of therapy for hyperuricemia and gout is the same regardless in which of the two categories (decreased clearance or increased production) the cause falls. The goal is a decrease in accumulated uric acid and therefore prevention of urate crystallization in the joints. Although the resulting symptom is often the same, careful consideration should be given to the cause prior to administration of treatment. A description of available treatment options will be reviewed providing topics essential for consideration as we explore how far we have come in the development of gout therapeutics.
Therapies for Gout and Hyperuricemia
Current practice in gout therapy is to treat the pain and inflammation initially, then begin therapy to prevent recurrent attacks. Common therapies are divided into three categories depending on the severity of the attack. Treatments for acute gout offer quick relief but are generally non-specific. These treatments include NSAIDS and glucocorticoids such as oral prednisone, methylprednisolone, and cosyntropin. Patients with acute gout are treated with an anti-inflammatory, and often supplemented with oral colchicines to decrease crystal deposition. Although the exact mechanism of action of colchicine is not known, it has been shown to decrease leukocyte lactic acid production, therefore decreasing uric acid crystallization. It has also been shown to inhibit neutrophil and endothelial cell adhesion molecules, thereby functioning to decrease inflammation.54,55
Intercritical gout, defined as intermittent attacks with asymptomatic phases in between, and prophylactic treatments also include oral colchicine, often supplemented with various NSAIDs. Colchicine does not prevent uric acid formation, but functions well as a prophylactic due to the decrease in uric acid deposition. For this reason, the drug is also commonly used initially if a previously diagnosed patient reports increased joint stiffness, pain, or swelling. Although colchicine is effective at decreasing the severity of an up-coming attack, it is usually only effective if administered within the first 10–12 hours after the onset of an attack.56,57 Colchicine reaches a steady state plasma concentration of 0.5 to 3.0 ng/ml following therapeutic dosing, however, toxicity can occur with concentrations in the upper end of the therapeutic range.58,59 Gastrointestinal symptoms, usually diarrheal, are the most common toxic effect of colchicine and pose a serious threat to patients with renal insufficiency due to the diarrhea induced dehydration posing even more strain on the renal system.47,58,59
Agents for chronic gout offer greater specificity and may also be used prophylactically in patients with recurrent attacks. These chronic gout therapies are categorized into xanthine oxidase inhibitors and uricosuric agents such as probenecid. Probenecid is a renal tubular-blocking agent which inhibits tubular absorption of urate resulting in increased renal excretion and decreased serum uric acid. The xanthine oxidase inhibitor oxypurinol is the active metabolite of the commonly prescribed allopurinol. Allopurinol has been utilized for gout treatments since the early 1960s and is still regularly selected for patients that show no signs of allopurinol sensitivity. Allopurinol is a purine based drug that inhibits the last two steps in purine breakdown without affecting biosynthesis of purine nucleosides. The drug binds in the active site of xanthine oxidase and is hydroxylated to oxypurinol, also called alloxanthine, which is effectively the active form of the drug. Despite the successful use of allopurinol for gout, some patients do suffer side-effects ranging from a minor rash to the more serious and life-threatening allopurinol hypersensitivity syndrome which may include worsening renal function, hepatitis, toxic epidermal necrolysis, fever, leukocytosis or any combination of these symptoms. It is important to note that diagnosis of allopurinol hypersensitivity syndrome usually requires at least two of the fore mentioned symptoms. One study suggested that an estimated 30% of the patients that take allopurinol report side-effects while only 5% choose to stop taking the drug. 56 Another study looking at the dosing of allopurinol for renal impaired patients indicates the presence of a rash in 2% of the patients. 1 The Boston Collaborative Drug Surveillance program suggests that approximately 0.38% of inpatients treated with allopurinol developed the life-threatening allopurinol hypersensitivity syndrome. 60
The number of patients being limited in allopurinol dosage due to renal impairment is presumed much larger. The average dose of allopurinol is 300 mg/day while the approved dosages range from 50 to 800 mg/day. 56 Patients with renal impairment require dosage adjustment of allopurinol, 1 however, modified dosing may still result in uric acid concentrations that are too high. 61 Clearly patients that are not able to tolerate adequate amounts of allopurinol due to renal impairment would benefit from an alternative therapy which is available and effective in lower doses as well as one that has not shown decreases in renal function when used therapeutically. Although the estimated percentage of patients that exhibit adverse effects to allopurinol treatment is relatively small, patients that exhibit allopurinol hypersensitivity syndrome would have no treatment options without newer therapies, and would therefore benefit from additional therapeutic choices.
The Food and Drug Administration (FDA) has recently approved febuxostat for the treatment of hyperuricemia and gout. This drug is classified as a xanthine oxidase inhibitor, but unlike its counterpart allopurinol, it is not purine-based and can be used in most patients exhibiting sensitivity to allopurinol reactions. 62 Mechanistically the drug functions very similarly to oxypurinol. Febuxostat binds tightly to the active site of xanthine oxidase, thereby inhibiting the breakdown of purines to uric acid. One major difference in the mechanism between the two drugs is that febuxostat binds tightly to both the oxidized and reduced forms of the enzyme, while allopurinol binds only to the reduced form of the enzyme. The consequence of this difference is that allopurinol needs active xanthine oxidase enzyme in order to produce oxypurinol, which then in turn inhibits the xanthine oxidase via a so-called suicide-inhibition. This xanthine oxidase dependent activation of its own inhibitor results in slower availability of oxypurinol, the active inhibitor. In terms of binding, this enzyme dependent activation requires that the enzyme be reduced in order to bind its inhibitor, thus limiting the rate of inhibition. Febuxostat, on the other hand, can bind either the oxidized or reduced form of xanthine oxidase, which means that febuxostat will bind and begin effective inhibition as soon as it comes into contact with xanthine oxidase, regardless of the oxidation state of the enzyme. Essentially, this difference in binding allows febuxostat to begin inhibition and thus stop uric acid production faster than allopurinol. This difference in rate of inhibition, also to some extent, allows the use of lower doses. The fact that febuxostat is not a purine is also beneficial because it does not affect activity of other purine metabolic enzymes, which may be particularly useful for patients with Lesch-Nyham syndrome or HPGRT deficiency. Approved doses of febuxostat (80–120 mg) have demonstrated efficacy in several patients at these levels.63–71
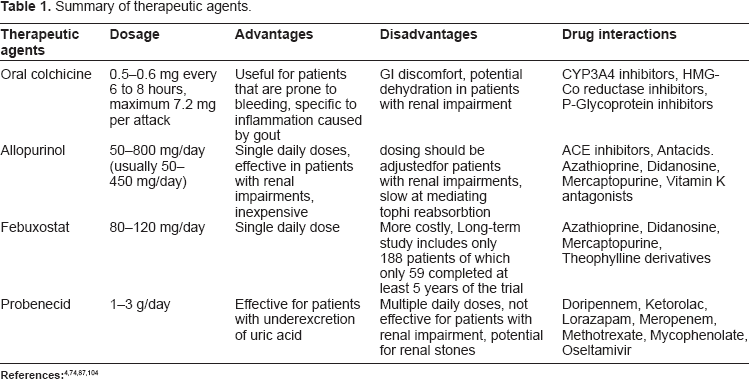
Table 1 describes commonly used therapeutic agents for gout with dosage comparisons as well as some advantages and disadvantages of each treatment. Major drug interactions are also included for each of the drugs colchicine, allopurinol, febuxostat and probenecid.
Pharmacokinetics and Pharmacodynamics of Xanthine Oxidase Inhibitors
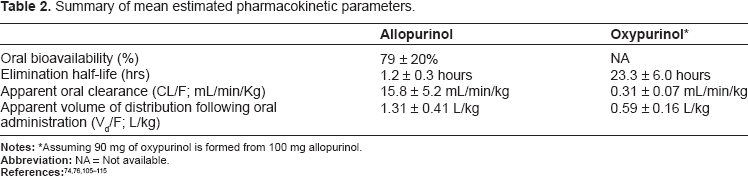
Allopurinol is a weak acid (pKa 9.4) which remains non-ionized at physiological pH. The octinol:water partition coefficient is 0.28 indicating marginal lipid solubility. 72 Allopurinol functions as a substrate for the enzyme xanthine oxidase forming the more active form of the drug, oxypurinol. Oxypurinol is more lipid soluble than allopurinol with an octanol: water coefficient of 14. 72 Oxypurinol is present in plasma partially ionized due to its increased acidity (pKa 7.7) as compared to allopurinol. These measures indicated that oxypurinol will more easily diffuse across cell membranes. In general it is thought that oxypurinol is the more active form of the drug for three reasons: First the complex between oxypurinol and xanthine oxidase is very stable, binding strongly to the reduced form of the enzyme. 73 Second, formation of oxypurinol is thought to occur from both xanthine oxidase and aldehyde oxidase activity with allopurinol, therefore leading to increased availability. 73 Third, Oxypurinol also has a longer half-life than allopurinol making it the more functional inhibitor for the enzyme. 73 Despite the extensive use of allopurinol, very few detailed pharmacokinetic studies have been published. The majority of the available studies report plasma concentration–-time data and elimination half lives. Using these available data, Day et al published a review estimating apparent oral clearances (CL/F) and apparent volumes of distribution (Vd/F). 74
Maximum plasma concentrations occur at different times for allopurinol and oxypurinol. Allopurinol is absorbed rapidly following an oral dose of 300 mg, reaching a maximum plasma concentration of 2 mg/L after 1.5 hours. The mean half-life of allopurinol is 1.2 hours. In comparison, the maximum concentration of oxypurinol, 7 mg/L, are reached 4 hours following 300 mg of oral administration of allopurinol and increases linearly with the allopurinol dose. The half-life of oxypurinol is longer, approaching 23 hours.75–77
Plasma urate concentrations reach a maximum decrease approximately 6 to 24 hours following oral administration of 300 mg allopurinol. A study exploring the effect of allopurinol dosing on plasma urate concentrations indicated that following a week long treatment of 200 mg/day of allopurinol, the mean plasma urate concentration was 62% ± 12% of pretreatment values whereas patients given 300 mg/day of allopurinol for one week exhibited a mean plasma urate concentration that was 56% ± 13% of pretreatment values. 78
Metabolism of allopurinol occurs primarily by enzymatic conversion to oxypurinol which is excreted in the urine. However, given that the product of xanthine oxidase reacting with allopurinol is the tight binding inhibitor of xanthine oxidase, oxypurinol, it seems that production of oxypurinol primarily through xanthine oxidase enzyme action would be self-inhibiting and limit the plasma availability of the active drug oxypurinol. This mechanistic observation suggests that xanthine oxidase is not the only enzyme producing active oxypurinol from allopurinol. However, the fact that the steady-state plasma concentration of oxypurinol is proportional to the dose of allopurinol, suggests that self-inhibition does not occur, again suggesting additional metabolic pathways.75,79,80 A likely enzyme candidate supplementing xanthine oxidase in the conversion of allopurinol to oxypurinol is aldehyde oxidase. Support for the involvement of aldehyde oxidase in allopurinol metabolism is demonstrated by patients which lack the enzyme xanthine oxidoreducase.73,81–83 Following an intravenous dose approximately 12% ± 6% of the allopurinol was excreted unmodified in urine, whereas 76% ± 8% was excreted as oxypurinol. 84 Also, approximately 10% of allopurinol is metabolized to allopurinol-1-riboside.85,86 Dosages of allopurinol must be adjusted for patients with renal impairment due to the primary urinary excretion of uric acid and are often based on the patient's creatinine clearance. Guidelines for these dosage adjustments are discussed in the special conditions section of the review.
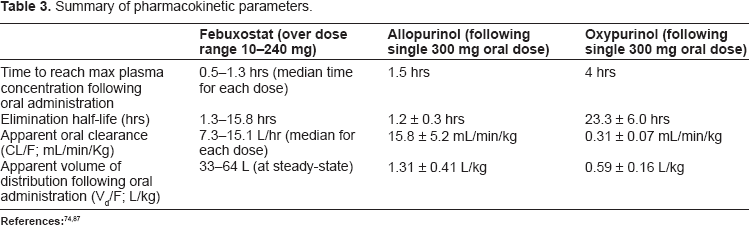
The pharmacokinetics and pharmacodynamics of febuxostat have been evaluated in healthy subjects during a dose escalation study with doses ranging from 10 to 240 mg. 87 Results for this study in addition to the allopurinol and oxypurinol data are summarized in Table 3.
With respect to pharmacodynamics, healthy subjects administered single doses of febuxostat ranging from 10 to 240 mg exhibited a decrease in serum uric acid concentration ranging from 27 to 76% over 14 days. The resulting serum uric acid concentrations ranged from 1.34 to 3.88 mg/dL. Likewise, a decrease in urinary excretion of uric acid of 76% over the 14 day trial. 87
Febuxostat is primarily metabolized by the uridine diphosphate-glucuronosyltransferas (UGT) enzymes UGT1A1, UGT1A3, UGT1A7, UGT1A8, UGT1A9, UGT1A10, and UGT2B7. Cytochrome P450 (CYP) enzymes CYP1A1, CYP1A2, CYP2C8 and CYP2C9 also play a small role in metabolism of CYP2D6, but did not show any significant inhibition on CYP1A2, CYP2C9, CYP2C19 or CYP3A4. However, the inhibition of CYP2D6 was not determined to be clinically significant. 88
Summary of Clinical Trials
There have been four main trials evaluating the safety and efficacy of febuxostat in the management of hyperuricemia and gout. The Febuxostat versus Allopurinol Controlled Trial (FACT), 67 the Allopurinol-Placebo-controlled Efficacy study of febuxostat (APEX), 71 and the Febuxostat Comparative Extension Long-term study (EXCEL) compared febuxostat to allopurinol, 66 which is the standard of care for decreasing uric acid production in gout patients. In addition to allopurinol, APEX also compared febuxostat to placebo. Patients with moderate renal insufficiency were included in APEX and EXCEL to assess the safety and efficacy of febuxostat in this patient population. The Febuxostat Open-label Clinical trial of Urate-lowering efficacy and Safety (FOCUS) 69 and EXCEL were conducted to assess long-term outcomes with febuxostat treatment. Researchers were interested in the ability of febuxostat to lower serum uric acid (sUA) concentrations and to reduce clinical manifestations of gout (tophi formation and gout flares). Adverse events (AE) were also assessed to determine the patients’ ability to tolerate febuxostat in the long-term management of gout. The efficacy and safety of febuxostat, as determined in the following trials, may provide evidence to support febuxostat as an important pharmacological option for patients with gout.
Febuxostat versus Allopurinol Controlled Trial 2005 67
The Febuxostat versus Allopurinol Controlled Trial (FACT) was a 52 week randomized, double-blind, multicenter clinical trial that compared the safety and efficacy of febuxostat with allopurinol. The researchers randomized 760 patients to 1 of 3 study groups: febuxostat 80 mg/day, febuxostat 120 mg/day, and allopurinol 300 mg/day. For the first 8 weeks, prophylaxis for acute gout attacks was provided (naproxen 250 mg twice daily or colchicine 0.6 mg mg/day). Patients were monitored at 2 weeks and 4 weeks and monthly thereafter. Researchers measured serum uric acid (sUA), laboratory tests, assessed renal function, compliance, concomitant medications, gout flares, tophi size and number (if applicable), and adverse events. Patients were included in the study with sUA ≥ 8.0 mg/dL and if they met the criteria for gout as defined by the American College of Rheumatology. Reasons for exclusion included serum creatinine (sCr) > 1.5 mg/dL; pregnancy/lactation; the use of urate-lowering agents, azathioprine, 6-mercaptopurine, thiazide diuretics, aspirin (.325 mg/day) or other salicylates; body mass index (BMI) > 50 kg/m2; history of xanthinuria, active liver disease, hepatic dysfunction; prednisone >10 mg/day; change in hormone replacement or oral contraceptive therapy within 3 months prior to the study; history of alcohol abuse; and alcohol intake >14 drinks/week.
The primary endpoint was sUA < 6.0 mg/dL at each of the last 3 monthly visits. This endpoint was achieved to a greater extent by patients taking febuxostat compared to patients taking allopurinol (53% of patients in the febuxostat 80 mg/day group, 62% in the febuxostat 120 mg/day group, and 21% in the allopurinol 300 mg/day group;
This study has several strengths. Several factors contributed to the study's design including double-blind, active-control, 2 week washout period for those previously taking urate-lowering agents, and randomization. The sample size was large, power was met, study was institutional review board (IRB) approved, informed consent was obtained, confidence intervals (CI) and
Although the study results are promising for treatment of hyperuricemia and gout with febuxostat, there are a few limitations to its clinical application. First and foremost, the study showed no difference in clinical outcomes between febuxostat and allopurinol. So, even though the study shows a greater reduction in sUA using febuxostat, there is no benefit to the patient clinically to use febuxostat over allopurinol in this study. Secondly, the high dropout rate is concerning, and longer periods of prophylaxis may be required. Therefore, the significance of this study is questionable, and long-term studies need to be conducted to find a clinical advantage to justify febuxostat's use over allopurinol.
Allopurinol-Placebo-controlled Efficacy study of febuxostat 2008 71
The Allopurinol-Placebo-controlled Efficacy study of febuxostat (APEX) was a 28 week randomized, double-blind study comparing the safety and efficacy of febuxostat, allopurinol, and placebo. There were 1067 patients randomized to 1 of 5 groups in a ratio of 2:2:1:2:1 (febuxostat 80 mg/day, febuxostat 120 mg/day, febuxostat 240 mg/day, allopurinol, and placebo). Allopurinol dosing was dependent on renal function (patients with sCr ≤ 1.5 mg/dL received allopurinol 300 mg/day and patients with sCr > 1.5 mg/dL received allopurinol 100 mg/day). Prophylaxis was provided for acute gout flares for the first 8 weeks (naproxen 250 mg twice daily or colchicine 0.6 mg/day). Every 4 weeks, researchers measured sUA, laboratory tests, gout flares, adverse events, concomitant medications, and tophi size and number. Inclusion criteria consisted of sUA ≥ 8.0 mg/dL, sCr ≤ 2.0 mg/dL, and history of gout defined by the American College of Rheumatology. Patients were excluded who had an intolerance to allopurinol, naproxen, or colchicine; history of renal calculi; alcohol intake ≥14 drinks/week; hepatic dysfunction (ALT and AST > 1.5 times the upper limit of normal); and any other significant medical conditions.
The primary endpoint was the proportion of patients with the last 3 monthly sUA levels < 6.0 mg/dL. A significantly greater proportion of patients taking febuxostat at any dose reached the endpoint compared to allopurinol and placebo (48% of patients taking febuxostat 80 mg/day, 65% of patients taking febuxostat 120 mg/day, 69% of patients taking febuxostat 240 mg/day, 22% of patients taking allopurinol, and 0% of patients taking placebo;
This study has several strengths. The study's design is appropriate (double-blind, active and placebo controlled, randomized, 2 week washout period for those previously taking urate-lowering agents, IRB approved, and informed consent obtained). The study had a large sample size. An intent-to-treat analysis was performed, power met,
Like FACT, this study shows promising results for sUA-lowering potential with febuxostat; however, a clinical difference between febuxostat and allopurinol was not seen. This warrants longer studies to find a clinical advantage to use febuxostat over allopurinol. There were a small number of patients in the study with impaired renal function; therefore, to study the effects of febuxostat on these patients, more studies need to be done. Similar to FACT, the dropout rate is high, which presents questions about tolerability.
Febuxostat Comparative Extension Long-term study 2009 66
As a result of the need for long-term studies, the febuxostat Comparative Extension Long-term study (EXCEL) was an open label 160 week extension study for patients completing FACT and APEX. The study's aim was to determine long-term efficacy in sUA lowering, clinical benefits, and safety of febuxostat or allopurinol. One thousand eighty-six patients were randomized to febuxostat 80 mg/day, febuxostat 120 mg/day, or allopurinol 300 mg/day (patients with renal impairment took allopurinol 100 mg/day) and therapy could be changed based on patient response during months 1 through 6. By the end of month 6, patients remained on a stable treatment dose. (Patients not achieving sUA < 6.0 mg/dL by 6 months were discontinued from the study.) Prophylaxis (naproxen 250 mg twice daily or colchicine 0.6 mg/day) was provided for the first 8 weeks of the study. Every 2 months, researchers monitored patients by assessing sUA, laboratory tests, gout flares, number and size of tophi, AE, and concomitant medication. Patients were included in the study if they previously completed the FACT and APEX trials. Exclusion criteria included pregnancy/lactation, serious drug-related AE in either of the previous studies, other significant medical conditions interfering with treatment safety or compliance, intolerance to allopurinol, and exclusion from FACT or APEX.
The primary endpoint was the proportion of patients with sUA < 6.0 mg/dL at each visit. More patients reached this endpoint in the febuxostat groups compared to allopurinol by the first month (81% of patients taking febuxostat 80 mg/day, 87% of patients taking febuxostat 120 mg/day, and 46% of patients taking allopurinol). By 12 months, 82% of patients on allopurinol reached this endpoint; however, only 63% of patients remained on allopurinol, while the nonresponders switched to febuxostat. The secondary endpoints included percent decrease in sUA from baseline, decrease in gout flares, and decrease in size and number of tophi. Reduction in sUA was greater in febuxostat patients compared to allopurinol (47% decrease with febuxostat 80 mg/day, 53% decrease with febuxostat 120 mg/day, and 32% decrease with allopurinol). After 18 months, <4% of patients across treatment groups reported acute gout attacks. Tophi size and number were decreased from 50 to 60%, and complete tophi resolution occurred in 30 to 45% of patients across treatment groups. There was no difference in gout flare incidence and tophi reduction between the groups. Similar rates of adverse events were reported across treatment groups, including serious adverse events. The most common adverse event was LFT abnormalities, and the most frequently reported serious AE was cardiovascular related. Researchers concluded that long-term maintenance of sUA < 6.0 mg/dL in both febuxostat and allopurinol resulted in near elimination of gout flares and reduction in tophi size and number.
The study has various strengths. Inclusion and exclusion criteria are appropriate, as well as primary and secondary endpoints. The study was IRB approved and informed consent was obtained. The study contained a large sample size, active control, and was conducted over a long study period. The researchers reported withdrawals, performed intent-to-treat, measured compliance, and explained limitations and unexpected results. Like every study, there are some limitations to its application. Prophylaxis was only given for 2 months, which may have contributed to the large dropout rate. Allopurinol dosing was not titrated, and patients taking allopurinol 300 mg were analyzed along with patients taking 100 mg. The effects of allopurinol were also possibly skewed due to the fact that the majority of patients were taking febuxostat. The study population was not similar to the general population (majority of patients were white males). Many patients had comorbidites and multiple medications. The study was performed at multiple sites (174), there was no blinding, no randomization, no
This study demonstrates the ability of febuxostat to decrease sUA levels, which eventually leads to decreased clinical manifestations of gout. More patients responded to febuxostat than allopurinol, but for all patients responding to either treatment, clinical endpoints were met. The lack of a statistical difference in clinical outcomes between febuxostat and allopurinol is a notable result to this trial because febuxostat does not present a clinical advantage to patients over allopurinol. However, the fact that more patients responded to febuxostat, including those who failed to respond to allopurinol, indicates febuxostat has a role in treatment for many patients with gout.
Febuxostat Open-label Clinical trial of Urate-lowering efficacy and Safety 2009 69
The Febuxostat Open-label Clinical trial of Urate-lowering efficacy and Safety (FOCUS) was a 5 year non-comparative extension of a Phase II dose-response trial to assess safety and efficacy of long-term febuxostat therapy. Patients (116) were initially given febuxostat 80 mg/day. Over 28 weeks, a maximum of 3 dose titrations to 40 mg/day, 80 mg/day, or 120 mg/day could be done to achieve therapeutic outcomes. After 28 weeks, the dose was maintained. Colchicine 0.6 mg was given twice daily for prophylaxis for the first 4 weeks. Patients were monitored at weeks 2 and 4, then every 4 weeks through week 56, and then every 8 weeks during years 2 through 5. Inclusion criteria (pulled from the original dose-response study) included sUA ≥ 8.0 mg/dL and a history of gout as defined by the American College of Rheumatology. Exclusion criteria (pulled from the original dose-response study) include sCr > 1.5 mg/dL; pregnancy/ lactation; use of urate lowering medication, azathioprine, 6-mercaptopurine, aspirin (>325 mg/day) or other salicylates; BMI > 50 kg/m2; history of xanthinuria, active liver disease, hepatic dysfunction; change in thiazide or steroid therapy within 1 month prior to the study, change in hormone replacement or oral contraceptive therapy within 3 months prior to the study; history of alcohol abuse; and alcohol intake ≥14 drinks/week.
The primary endpoint was the proportion of patients achieving and maintaining sUA < 6.0 mg/dL. For patients remaining in the study at the end of 5 years, 93% had sUA < 6.0 mg/dL. Overall, 83% of patients reached the primary endpoint at their final visit. Secondary endpoints included the percent reduction in sUA from baseline, the proportion of patients reaching sUA < 5.0 mg/dL and <4.0 mg/dL, the proportion of patients needing treatment for acute gout flares, and the resolution of tophi. At the final visit, percent decrease from baseline was similar among the different febuxostat doses (49.2% for febuxostat 40 mg/day, 47.1% for febuxostat 80 mg/day, and 50.7% for febuxostat 120 mg/day). The proportion of patients reaching sUA < 5.0 mg/dL ranged from 47%–66% and sUA < 4.0 mg/dL ranged from 11%–28%. The percent of patients requiring treatment for gout flares dropped to zero by year 5. Resolution of tophi occurred in 69% of patients by the final visit. Throughout the trial, adverse events were reported by 91% of the patients (a majority being mild or moderate in severity including LFT abnormalities, diarrhea, headache, joint, musculoskeletal, and connective tissue signs and symptoms). Serious adverse events were reported by 18% of patients, with atrial fibrillation being the most common. The authors concluded that lowering sUA to a level < 6.0 mg/dL by febuxostat was demonstrated in this trial, and that continued therapy resulted in decreased incidence of gout flares and resolution of tophi.
Strengths of this study include being IRB approved, having informed consent, and lasting 5 years. Inclusion and exclusion criteria, primary endpoints, and secondary endpoints are appropriate. The study included a large number of patients with renal insufficiency to assess febuxostat safety and efficacy in this patient population. The researchers reported withdrawals, presented data clearly, performed intent-to-treat analyses, and accounted for confounding variables. However, some limitation existed. The background did not describe the dose-response trial that FOCUS stemmed from. The design was not appropriate (no blinding, no control, no randomization). The study was conducted at 23 different sites, which may introduce investigator error. Statistical tests were not mentioned and power was not calculated. Treatment of acute flares was done at the discretion of the investigator, which may have influenced results. The dropout rate was high, with the majority of patients discontinuing treatment due to “personal reasons” (which may or may not have to do with the treatment). The study population does not reflect the general population, prophylaxis was only given for the first 4 weeks, a possible funding bias existed, data collection for tophi was not accurate, and a majority of patients were taking other medications for a variety of co-morbid conditions.
Although this study demonstrates the ability of febuxostat to lower and maintain sUA at goal levels, it does not compare febuxostat to anything else to assess efficacy and safety. The results of this study would be more reliable with careful design and fewer potential factors of interference with treatment. As with the other trials, the dropout rate is large. This questions the tolerability of febuxostat. This trial would have been useful if febuxostat was compared to allopurinol.
Trial conclusions: efficacy and safety of febuxostat
All 4 main febuxostat trials (FACT, APEX, EXCEL, and FOCUS) demonstrated the drug's ability to lower uric acid production so that serum concentrations were below tissue saturating levels. Not only does febuxostat lower sUA to goal levels, but it does so in a greater proportion of patients and to a greater extent than allopurinol. Clinically, febuxostat demonstrated a decreased incidence of gout flares, reduction of size and number of tophi, and eventual resolution of tophi. Therefore, by maintaining sUA < 6.0 mg/dL, febuxostat has the potential to reduce the clinical manifestations of gout. For patients, reducing gout flares and tophi is desirable, and for patients who have failed allopurinol therapy, this is a viable option.
However, the limitations of these trials are important and worth mentioning in regards to the efficacy of febuxostat. None of the trials were able to demonstrate a statistical difference in clinical endpoints between febuxostat and allopurinol. Although febuxostat can lower sUA more robustly than allopurinol, there is no benefit to the patient if no difference is observed clinically between the two drugs. In addition, the trials cite that the allopurinol dose can be titrated up to 800 mg/day based on patient response. This means that some patients may have received a sub-therapeutic dose, and consequently, positive effects were not observed. However, in practice allopurinol is most commonly prescribed at 300 mg/day, so this limitation may not have a great impact in the general population. A few of the researchers have mentioned that the method for collecting clinical data was not very accurate, and may leave room for subjective error. By determining a better approach to collecting clinical data, a significant difference between febuxostat and allopurinol may be found.
Febuxostat is very effective at lowering sUA and decreasing clinical manifestations of gout in many patients. Future studies should be aimed at comparing febuxostat with allopurinol to find differences in clinical endpoints to determine whether or not febuxostat holds a clinical advantage over allopurinol.
Across the 4 trials, patients experienced similar adverse events, most of which were categorized as mild to moderate in severity. The most commonly reported events include LFT abnormalities, diarrhea, headache, musculoskeletal, connective tissue, and joint signs and symptoms. LFT abnormalities were the most common adverse events that led to discontinuation. In 3 of the 4 studies, cardiovascular related serious adverse events were reported. Researchers deemed these events unrelated to the study drug; however, the fact that more than one trial has observed this phenomenon questions the safety of febuxostat in patients with pre-existing cardiovascular disease and/or risk factors.
The incidence of gout flares increases initially when beginning urate-lowering therapy. This is thought to be because of excessive uric acid mobilization. Another common reason for study discontinuation was gout flares. Prophylaxis with naproxen or colchicine may need to be provided over a longer period of time in order to decrease the dropout rate due to acute gout flares. If future studies incorporate this, it will be interesting to see if the dropout rate decreases, especially early in therapy.
Febuxostat is well tolerated in patients, as evidenced by the high compliance rates observed in each trial. Compared to allopurinol, febuxostat does not present any tolerability issues for patients, as the studies showed similar incidences of adverse events. Future studies should be aimed at exploring cardiovascular-related events and whether they are related to febuxostat, as well as the effect on the dropout rate and incidence of gout flares with longer prophylaxis administration.
Through these 4 trials (FACT, APEX, EXCEL, and FOCUS), febuxostat has demonstrated efficacy and tolerability in patients with gout. Compared to the current standard of care (allopurinol), febuxostat is more effective at lowering sUA in a greater number of patients and to a greater extent. If future studies can prove a significant difference in clinical endpoints between febuxostat and allopurinol, then febuxostat would clearly be superior to allopurinol in clinical practice. However, if future studies provide a link between cardiovascular events and febuxostat, more caution should be taken in prescribing febuxostat to patients with these risk factors. Until these studies are done, febuxostat provides an alternative pharmacological option for patients with hyperuricemia and gout, especially for patients who have not responded to allopurinol therapy.
Special Conditions
Allopurinol Hypersensitivity Syndrome
The allopurinol hypersensitivity syndrome (AHS) is a potentially life-threatening adverse event of allopurinol that occurs in approximately 0.4% of patients. The exact mechanism for AHS is unknown, but there have been three possible mechanisms proposed that may play a role in the reaction: immunologic factors (including both humoral- and cell-mediated immune reactions), genetic predisposition, and drug accumulation. 90
Allopurinol is metabolized via xanthine oxidase to its primary active metabolite, oxypurinol, to exert its pharmacologic effect in the management of gout. It is also metabolized by hypoxanthine-guanine phospho-ribosyltransferase (HGPRT) and orotate phosphori-bosyltransferase (OPRT) to form other nucleotide and nucleoside derivatives. Due to the structural similarities of allopurinol and its metabolites to purines and pyrimidines, these analogues bind and inhibit other enzymes involved in purine and pyrimidine metabolism, including purine nucleoside phosphorylase (PNP) and orotidine-5‘-monophosphate decarboxylase (OMPDC). Allopurinol and its metabolites have been reported to inhibit T-cell function, most likely due to the inhibition of PNP. Impaired T-cell function, through a cell-mediated immune reaction, may result in AHS. 91
Allopurinol accumlation is also considered a risk factor. Oxypurinol, allopurinol's major metabolite, has a long half-life and is primarily excreted by the kidney. In renal impairment, the half-life of oxypurinol is extended, therefore, less frequent dosing of allopurinol is required. If the dosing interval is not adjusted, oxypurinol can accumulate to potentially toxic concentrations leading to either a toxic mechanism in genetically predisposed patients or an immunologic reaction that causes tissue injury. Tissue injury then leads to the release of antigens, which causes a secondary immune reaction. 90
Febuxostat is a non-purine based xanthine oxidase inhibitor. Studies have shown that febuxostat does not affect other enzymes in purine and pyrimidine metabolism, including guanine deaminase, HGPRT, PNP, OMPDC, or OPRT, most likely due to its non-purine based structure. 91 Therefore, febuxostat is considered a selective inhibitor of xanthine oxidase. Unlike allopurinol, febuxostat is primarily metabolized through hepatic enzymes to acyl-glucuronide and (to a much lesser extent) oxidative metabolites. Less than 5% of unchanged drug is excreted renally. Therefore, drug accumulation in patients with renal impairment is not of concern with febuxostat. Febuxostat is an excellent pharmacologic choice for managing patients with gout, not only because it is very effective in decreasing uric acid production, but also because it does not cause this serious hypersensitivity reaction seen in patients taking allopurinol.
Patients on purine based therapies
Azathioprine is a thiopurine immunosuppressant used in organ transplant patients and autoimmune inflammatory diseases. Azathioprine is a prodrug that is rapidly converted via glutathione S-transferase to 6-mercaptopurine. 6-mercaptopurine is metabolized via three pathways: thiospurine S-methyltransferase (TPMT), xanthine oxidase, and hypoxanthine phosphoribosyl transferase (HPRT). Metabolism via TPMT leads to the active metabolite 6-methylmercaptopurine, and metabolism via HPRT leads to the other active metabolite 6-thioguaninenucleotide. In a case report, a woman taking azathioprine presented with chronic autoimmune pancreatitis with no active azathioprine metabolites (compliance was confirmed). The researchers concluded that, due to high xanthine oxidase activity, 6-mercaptopurine was not available to the other metabolic enzymes to form the active metabolites. They gave the patient allopurinol to inhibit xanthine oxidase, and a few days later found active metabolites of azathioprine. Eventually, the metabolite levels increased far above therapeutic range, and the patient developed leukopenia (which resulted in discontinuation of the drugs). This confirmed the researchers’ findings and emphasizes the importance of xanthine oxidase in thiopurine metabolism. 92
Studies have shown that pretreatment with allopurinol resulted in a five-fold increase of 6-mercaptopurine bioavailability, and there have been reports of myelotoxicity due to the combination. 93 The dose of azathioprine and 6-mercaptopurine should be decreased to one-third of normal with concomitant allopurinol use. Because febuxostat inhibits xanthine oxidase, serum concentrations of 6-mercaptopurine and its active metabolites may increase, leading to potential hematologic toxicity. There is no data available concerning the interaction between these drugs and febuxostat; however, concurrent use of the medications is not recommended and considered contraindicated.
Cardiac failure
Increased systolic blood pressure over time can lead to left ventricular hypertrophy and congestive heart failure. The increased size and workload of the heart increases myocardial oxygen consumption, which can ultimately lead to ischemia in the failing heart. Hyperuricemia has been shown to be an independent predictor of mortality in patients with heart failure. A retrospective cohort study showed that patients treated with higher doses of allopurinol (300 mg/day) had similar cardiovascular-related mortality compared to patients without hyperuricemia. Patients treated with lower doses of allopurinol (100 mg/day) had higher cardiovascular-related mortality, suggesting that patients with poorly treated gout, and thus hyperuricemia, have greater cardiovascular-related mortality. 94
Increased uric acid production results from increased activity of xanthine oxidase. Under normal conditions, xanthine oxidase generates reactive oxygen species (ROS), which are regulated and broken down by other enzymes. However, in hyperuricemia, the activity of the enzyme may be greater than the activity of the regulatory enzymes, resulting in increased ROS. ROS impair nitric oxide production; therefore, vasodilation in response to increased blood volume or heart rate is impaired, leading to increased blood pressure. This chronic endothelial dysfunction results in heart failure. 95
Febuxostat has been evaluated in mice with transverse aortic constriction, and it has shown to significantly decrease systolic overload-induced left ventricular hypertrophy, dysfunction, and fibrosis. 96 Through xanthine oxidase inhibition, febuxostat decreases ROS production and allows nitric oxide production to occur normally. With normal regulatory mechanisms to control blood pressure intact, the heart undergoes less stress. Studies in humans have shown increased peripheral vascular capacity and blood flow (to the myocardium and the rest of the body) when given allopurinol. 97
Not only does febuxostat decrease uric acid production, it also may decrease cardiovascular mortality by reducing oxidative stress. During ischemia, the oxidative half reaction is inhibited because oxygen is not available to receive electrons. This leads to an accumulation of reactive oxygen species that sit in the enzyme until reperfusion with oxygen. Upon reperfusion, the enzymes that normally break down ROS cannot keep up with the release of ROS from the enzyme. The increase in ROS leads to tissue damage and ultimately heart failure. Through xanthine oxidase inhibition by febuxostat, less reactive oxygen species are produced; therefore, less tissue damage. 98
Febuxostat may provide cardio-protection in patients with heart failure by decreasing uric acid production (thus decreasing endothelial dysfunction) and decreasing tissue injury caused by oxidative stress. Febuxostat has proven to have greater urate-lowering potential than allopurinol; therefore, it may decrease cardiovascular mortality to a greater extent than allopurinol.
Renal insufficiencies
Renal failure can be caused by several mechanisms, including vasoconstriction in the kidney, oxidative stress, tubular and micro-vascular injury, and interstitial inflammation. There have been several studies done suggesting that hyperuricemia may contribute to renal failure and possibly cause it. It has been shown to be an independent predictor of the development of microalbuminuria and renal dysfunction. There have been some studies showing decreased progression of renal failure and improved renal function in patients with hyperuricemia when treated with allopurinol.
One study performed in patients with normal renal function measured the effect of allopurinol treatment on glomerular filtration rate and other parameters. The researchers found that allopurinol significantly improved all of these parameters compared to control, indicating not only that hyperuricemia affects glomerular filtration rate, but also that allopurinol treatment may delay the progression of renal failure. 99 In another study among patients with chronic kidney disease, treatment with allopurinol resulted in a lower serum creatinine level compared to the control group, as well as less patients reaching endpoints for kidney function deterioration with allopurinol. The researchers concluded that allopurinol treatment preserved kidney function compared to patients not taking allopurinol. 100
A complication of ureterolithiasis may be renal failure. Uric acid is primarily reabsorbed in the proximal tubule via the URAT1 transporter (90% of filtered uric acid is reabsorbed). In patients with hyperuricemia, the amount of uric acid in the renal tubules may overload the reabsorption ability of URAT1 and result in urolithiasis. This is especially noticed among patients in the Japanese population due to a mutation in the transporter that impairs its function. 35 These patients are said to have renal hypouricemia because uric acid is not reabsorbed from the kidney. Renal hypouricemia results in greater incidence of urolithiasis. Febuxostat, by inhibiting xanthine oxidase, can decrease uric acid production, thus decreasing the incidence of urolithiasis.
Hyperuricemia, through a variety of mechanisms, may cause vasoconstriction in the kidney. As explained earlier, increased xanthine oxidase activity (evidenced by hyperuricemia) generates increased ROS, which impair NO production. This leads to endothelial dysfunction and increased blood pressure within the renal vasculature. Uric acid can also cause vasoconstriction by decreasing prostaglandin production and increasing angiotensin II production via the renin-angiotensin system. 8 Oxidative stress, which can also lead to renal failure, can be attributed to hyperuricemia via increased ROS generation as described above. By decreasing uric acid and ROS production via xanthine oxidase inhibition, febuxostat can delay the progression of renal failure.
Diabetic patients
Many studies have shown a correlation between hyperuricemia and features of metabolic syndrome, including type II diabetes mellitus. Some evidence suggests serum uric acid as an independent predictor of diabetes development. Insulin requires nitric oxide to stimulate glucose uptake. When nitric oxide response to insulin is impaired, insulin resistance is thought to develop. An increase in serum uric acid decreases nitric oxide. Therefore, hyperuricemia may be linked to insulin resistance and type II diabetes. 8
A meta-analysis was performed involving 11 cohort studies. 101 The researchers found that an increase in serum uric acid of 1 mg/dL resulted in a relative risk of developing type II diabetes mellitus of 1.17. The study concluded that serum uric acid levels are positively correlated with the development of diabetes regardless of other disease states; therefore, uric acid should be considered an independent predictor of diabetes development.
Studies have shown that allopurinol prevented and even reversed features of metabolic syndrome. 102 By using febuxostat to inhibit xanthine oxidase, serum uric acid will decrease and nitric oxide will respond to insulin in order to increase glucose uptake into cells. In a study done in rats fed with fructose (shown to increase uric acid), allopurinol was given to examine the development of insulin resistance. Allopurinol was shown to improve insulin sensitivity compared to controls. The researchers speculate that hyperuricemia may play a role in causing features of metabolic syndrome, including diabetes, and treatment with xanthine oxidase inhibitors, like febuxostat, may decrease insulin resistance and the progression of type II diabetes.
Hypertension
Hypertension can be linked to endothelial dysfunction, in which the response to mechanisms aimed at regulating blood pressure is impaired. Endothelial dysfunction has been linked to elevated levels of uric acid. Hyperuricemia inhibits nitric oxide production via ROS generation. Due to impaired nitric oxide production, vasodilation does not occur properly; therefore, hypertension develops over time.
In rats, there was an inverse correlation between uric acid levels and serum nitrates. The study also showed a dose-dependent inhibition in nitric oxide production with increasing uric acid. Mice treated with allopurinol showed a completely reversed inhibition of nitric oxide production after 7 days of treatment. The study demonstrated that the decrease in nitric oxide due to hyperuricemia is reversed with allopurinol treatment in rats. 95
In another study among patients with newly diagnosed stage 1 hypertension, allopurinol was given to determine the effects on casual and ambulatory blood pressure. 103 While patients were receiving allopurinol, reductions in both casual and ambulatory blood pressure occurred to a greater degree when compared to control. In fact, the extent of blood pressure lowering was similar in these patients when compared to most anti-hypertensive drugs. Two-thirds of the patients achieved normal blood pressure levels with allopurinol. This study provides a potentially new therapeutic approach to treating hypertension, and studies with febuxostat should be conducted in the future.
Concluding Remarks
Based on evaluation of summarized clinical trials and special conditions, it is apparent that febuxostat is effective at lowering uric acid levels. Although a decrease is noted both with patients taking febuxostat and with patients taking allopurinol, the review of special conditions certainly speaks positively regarding the availability and development of febuxostat. Importantly, clinical trials did not show significant differences in the clinical outcomes, only in serum uric acid levels. In general, the goals of the trial were to compare the decrease in uric acid levels between the two treatment groups, a goal which was met in each case. However, by use of this comparative design, the study was not able to compare clinical outcomes based on patients’ previous or current accompanying conditions. Similarly, the study (even in the extended version) was not long enough to conclusively compare tophi size or the manifestations of clinical symptoms. The comparison is further complicated by the fact that neither febuxostat or allopurinol result in immediate relief of symptoms, and in the case of febuxostat, seem to generate an increase in gouty attacks as uric acid is mobilized during early treatment. For this reason, clinicians were encouraged to treat flare ups and discomfort via conventional NSAID methods, possibly altering the significance of the results with both drugs. Many current opinions based on these trials, support the use of febuxostat and refer to it as superior to allopurinol. Again, these opinions are based solely on the dose (lower for febuxostat than allopurinol) and the comparable decrease in serum uric acid. Although febuxostat clearly achieves this decrease at a much lower dose than allopurinol, the difference in end points between the two drugs is not substantial. Also worth noting, is that trials did not include a careful titration of allopurinol to achieve maximal therapeutic efficacy, as suggested by the manufacturer. Without achieving maximal effectiveness with allopurinol, the efficacy of the two drugs cannot be directly compared.
In conclusion, febuxostat is definitely an effective alternative to allopurinol therapy. However, based on insignificant differences in clinical outcomes between the two drugs, the need for an alternative therapy in healthy patients (those with no other co-existing disease states or identified sensitivity to allopurinol) is limited. Selective treatment with febuxostat should be indicated in patients that have exhibited sensitivities to allopurinol or in patients’ disorders in purine metabolism. Importantly, patients suffering renal impairment will likely benefit remarkably from this alternative therapy more notably than those without renal impairment. How far have we come from allopurinol? Considering the comparable effectiveness and safety exhibited thus far for febuxostat, it appears that despite minimal differences in clinical outcome (often also limited with allopurinol) and cost, therapeutic advances in gout treatment have advanced considerably in recent research; this much needed advancement coming decades following development of our previous “most effective” treatment for gout and hyperuricemia. Although perhaps limited to a subgroup of patients exhibiting hyperuricemia, the advancement promises decreased pain and increased mobility for a number of patients that could not be treated effectively prior to the development of febuxostat.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgements
We would like to thank Dr. Dave Kisor for his careful reading and editing of the manuscript.