
Abstract
Today the world is facing a high prevalence of dyslipidemia among type II diabetes, and in matter of fact clinical practices against hyperglycemic and hyperlipidemia were quiet intrusive. Our aim was to determine the therapeutic compliance against the clinical practices of dyslipidemia with type II diabetes in a multiracial society. A three year retrospective cohort study was planned to achieve the above mentioned objectives of the study. Study was carried out in out-patient department of General Hospital Penang over a period of ten months (Jan–Oct 2008). Study data collection duration was from Jan 2005–Dec 2007. All the concerned approvals were obtained from Clinical Research Committee (CRC). Data was analyzed by using SPSS 15®. A total of all only 501 diabetes type 2 patients with dyslipidemia were included in this study. The demographic data showed that 55.9% (n = 280) were female patients and 44.1% (n = 221) were male patients. According to racial distribution, Chinese constituted 41.7% of the study population, Malay 34.3% and Indians 24%. The mean age was 62.2 ± 9.2 years. About 56.1% of patients were more and equal than 60 years old range, while 43.9% were in the less or equal range of 59 years. Lifestyle and social habits data demonstrated 86.2% non-smokers, 74.1% with uncontrolled diet and 78.4% on bad exercise. Patients on combination therapy of metformin with other antidiabetic agent were 79%, while 21% were on monotherapy. The test analysis revealed that there was a significant difference between Malay and Chinese in FPG levels, in which the Malay had higher mean FPG than Chinese (mean difference Malay/Chinese 0.75991, P = 0.007). This study showed that both metformin and lovastatin were effective in reducing elevated glucose and lipid values. However, for glucose levels, the values were still above the normal limit used by the hospital. Among the multiracial study population, Chinese had the most controlled HDL levels and Malay had the highest uncontrolled FPG levels. Recommendations were associated with more frequent follow- up and therapeutic monitoring for the patient's condition by the health practitioners to determine the appropriate compliance with therapy and to control diabetes and dyslipidemia as per needed with therapeutic goals.
Introduction
The need for strict glycemic control in order to avoid or postpone the development of late complications in patients with type 2 diabetes mellitus (DM2) has been well established. 1 Although the initial management of DM2 involves lifestyle changes and oral hypoglycemic drugs, a significant number of patients will need insulin in order to reach satisfactory glycemic control. 2 Furthermore, DM2 does not mean glycemic alterations alone since this disease is associated with cardiovascular risk factors such as dyslipidemia, systemic arterial hypertension, and obesity. 3 This association is clinically relevant since over 50% of deaths among DM2 patients are due to cardiovascular disease. 4
Treatment of DM2 must include pharmacological agents able to improve not only glycemic levels, but also blood pressure (BP), lipid levels, and body weight, since in approximately 90% of type 2 diabetics hyperglycemia is associated with other cardiovascular factors that constitute the metabolic syndrome.
Several studies5,6 have demonstrated that, in order to prevent the development and progression of chronic complications of diabetes, a comprehensive approach to all elements of the metabolic syndrome is required. The main feature of the metabolic syndrome, which can be clinically assessed by measurement of the waist circumference (WC) whenever more sophisticated laboratory methods are not available, 7 is insulin resistance.
After metformin proved to be effective in reducing insulin resistance, 8 several studies were undertaken to assess its effects on total cholesterol (TC), triglycerides (TG), and HDL-cholesterol (HDL-C) levels, and also on BP and body mass index (BMI). However, there is no consensus about its beneficial effects on these parameters. 9 Most studies have analyzed independent samples, comparing patients on insulin with patients on combined insulin-metformin therapy10–12 with no conclusive results.
Lipid abnormalities will lead to the development of atherosclerosis, the central pathological mechanism that causes the macrovascular complications in type 2 DM. 13 As lovastatin may be of particular importance in patients with complex dyslipidemias, such as those with Type 2 diabetes mellitus and metabolic syndrome.14,15 Clinical reviews highligtened the important revelence of lovastatin among type 2 Diabetes with Dyslipidemia.16–18 According to the United Kingdom Prospective Study UKPDS 35 the management of hyperglycemia was only associated with reduction in micro vascular complications and only 16% reduction in the macro vascular complications. Macro vascular events were improved by controlling lipid and blood pressure abnormalities. 14 In Malaysia, the prevalence of dyslipidemia among diabetes type 2 subjects is 63%–76%. 15
This study was aimed to characterize the evidence of use of metformin (monotherapy and combined antiglycemic) against lovastatin (monotherapy and combined gemfibrozil), in term of monitoring parameters of Diabetes type II and Dyslipidemia. We assumed that both principal therapies (metformin and lovastatin) are significantly improving the core symptoms when used as monotherapy as compared to combination with other either hypoglycemic agent or hypolipidemic drug.
Methods
A three years retrospective cohort study was planned to achieve the above mentioned objectives of the study. Study was carried out in out-patient department of General Hospital Penang over a period of ten months (Jan–Oct 2008). During the data collection period, the study was deemed to cover three years of cohort analyses which include 2005, 2006, 2007. Study population was targeted on the basis of type II diabetes with dyslipidemia. Once the targeted sample was identified we then redistributed them in two separate cohorts one with metformin (mono or combined therapy) other with lovastatin (mono or combined therapy). Then each cohort were separately analyzed against the respective monitoring parameters to identify the compliance and therapeutic effectiveness during a period of 3 years.
We took the continuous form of data in each monitoring parameter and compared and contrasted against the mean and standard deviations against the normal range of hospital setting. All of the monitoring parameters were divided into two datasets, one includes the baseline reading on the initiation of the therapy and other was the last recorded value with the same therapy. If the therapy was changed from mono to combine therapy then the last lab values would be considered as the baseline value of combined-drug therapy and vice-versa. Patients’ demographic data, medication profile, and laboratory tests for glucose and lipids were the prime monitoring parameters in this study. The study is certified with the approval of Clinical Research Committee (CRC) as all the ethical requirements were fulfilled during the study period.
Hb1AC with FBS
Due to the limited availability of subjects’ HbA1c results, in this study sub-optimal glycaemic control was defined as a mean of at least three fasting blood glucose (FBG) levels of more than 7 mmol/L. Prior studies have shown that FBG of more than 7 mmol/L is associated with increased micro- and macro-vascular complications.16–19
Dietary reference for uncontrolled diet
The quantity of carbohydrate intake and the number of meals consumed each day were recorded by physician or self-reporting assessment. Patients’ data reflects how often they ate during their waking hours. Patients were asked to reduce carbohydrate intake during meals when they had consumed sweetened foods and drinks and whether their eating habits in the last week resembled their usual behavior.
Adherence to therapy
Medication adherence was characterized with reference to reported medication dosage, frequency and timing with the physician's prescription. Medical adherence was defined as adherence to 90% or more of the daily prescribed medication and calculated as the number of doses actually taken divided by the number prescribed. 20 All the patients selected retrospectively in this study were in compliance with the above.
Physical activity
Assessment of physical activity included leisure, non-leisure and total daily physical activities minutes of activity such as walking or cycling. Activity levels were categorized as ‘least active’ (bad exercise 0–10 min), ‘moderately active’ (10–25 min) and ‘most active’ (>25 min). Self-reported system was used to assess the parameter.
Statistical analysis
Data obtained were analyzed by using the Statistical Package of Social Sciences (SPSS) version 15®, Chi-square, paired and independent t-tests as well as univariate analysis of variance (ANOVA) have been used to compare results. The level of significance was 0.05 with the confidence interval of 95%. All the results and findings were then illustrated in discussion section in term of comparison. We intend to determine the argumentive issues in this study to be of benefit in clinical practice.
Results
A total of all 501 diabetes type 2 patients with dyslipidemia were included in this study. The demographic data showed that 55.9% (n = 280) were female patients and 44.1% (n = 221) were male patients. According to racial distribution, Chinese constituted 41.7% of the study population, Malay 34.3% and Indians 24%. The mean age was 62.2 ± 9.2 years. About 56.1% of patients were more and equal than 60 years old range, while 43.9% were in the less or equal range of 59 years. Lifestyle and social habits data demonstrated 86.2% non-smokers, 74.1% with uncontrolled diet and 78.4% on bad exercise. Patients on combination therapy of metformin with other antidiabetic agent were 79%, while 21% were on monotherapy. Lovastatin was received as monotherapy in 83% of study population, while only 17% were on combination with gemfibrozil. Means of FPG and lipid profile were reduced from the initial (2005) to the latest level (2007) significantly (Table 1).
Difference in means for variables from initial to latest levels.
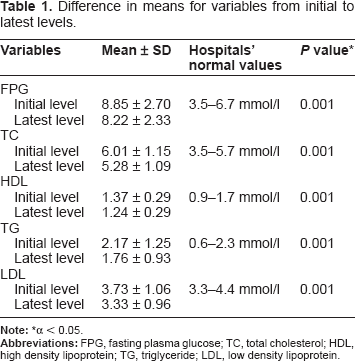
α < 0.05.
Control values were between 3.5–6.7 mmol/l, while uncontrolled values were >6.7 mmol/l. We found that majority (396, 79%) of the patients were receiving combination therapy for hyperglycemic condition and among them 83.3% (304) patients have uncontrolled FPG levels which is significantly higher as compared to 58.1% (61) patients on monotherapy with Metformin. While 32.4% of patients on monotherapy had controlled FPG levels significantly (Table 2). We found that monotherapy with Metformin is more likely to control FPG level as compared to combination therapy (OR: 2.4). In contrast to hyperglycemic control results, hyperlipidemia control measures showed that majority of patients were on monotherapy with lovastatin (416, 83%) with controlled lipidemia among 291 (86.6%) which is significantly higher than 40 (52.95) patients with combination therapy of Gemfibrozil (Table 3). The odd control ratio showed that patients with lovastatin monotherapy were more likely to control lipidemic condition as with lovastatin with Gemfibrozil.
Regarding analysis of monitoring parameters against gender, we found that females exhibited higher mean FPG value than males with no significance but they had significantly higher mean TC (0.005) and HDL (0.001) than males. Moreover, females had higher LDL and lower TG levels than males with no significance (Table 4).
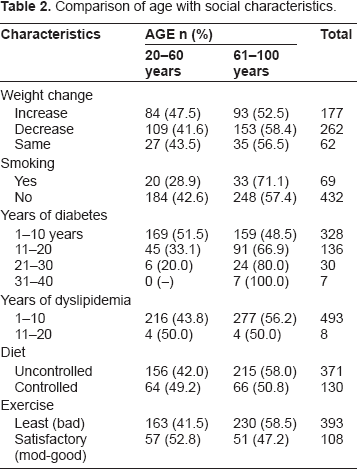
Comparison of age with social characteristics.
Therapeutic monitoring of metformin regime by using FPG parameter.
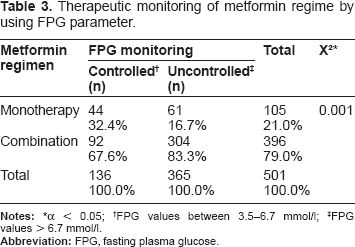
α < 0.05;
FPG values between 3.5–6.7 mmol/l;
FPG values > 6.7 mmol/l.
Therapeutic monitoring of lipidemia regimen by lipidemic parameter.
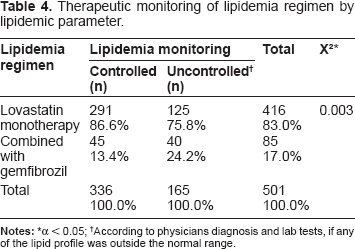
α < 0.05;
According to physicians diagnosis and lab tests, if any of the lipid profile was outside the normal range.
The test analysis revealed that there was a significant difference between Malay and Chinese in FPG levels, in which the Malay had higher mean FPG than Chinese (mean difference Malay/Chinese 0.75991, P = 0.007). Likewise, Malay had higher TC values than Chinese and Indians with no significance (mean difference Malay/Chinese and Malay/Indians 0.04284, P = NS and 0.02908, P = NS respectively). Furthermore, Chinese exhibited higher levels of HDL than Malay and Indians significantly (mean difference Malay/Chinese and Indian/Chinese -0.13521, P = 0.001 and -0.12691, P = 0.001 respectively). There was no significant difference found among the races regarding TG and LDL levels. However, Chinese had the highest TG values (mean difference Malay/Chinese and Chinese/Indians -0.07504, P = NS, 0.11808, P = NS respectively), while the Malay were with the highest LDL levels (mean difference Malay/Chinese and Malay/Indians 0.21952, P = NS and 0.02241, P = NS respectively).
Discussion
In Malaysia, the prevalence of dyslipidemia among type 2 diabetic patients is 63%–76%. 21 We found that metformin monotherapy were more likely to reduce the mean FPG level with compared to combined with other antidiabetic agent, significant results were presented in baseline (Table 1). Nevertheless, FPG values were still above the normal range of the hospital, indicating inadequate glycemic control and the values were above the recommended goals (10.3 and 7.85 mmol/l respectively). So difficulty in achieving adequate control might be due to several factors such as poor adherence of patients to therapy, uncontrolled diet, lack of exercise and poor follow-up. 22
On the other hand, the means of TC, HDL, TG and LDL were significantly reduced from the baseline to the latest levels which were within the hospital normal range (Table 1). These results agree with the findings of Oikawa et al 23 in which the lipid profiles showed reduction from the baseline to values within the normal range of each variable (TC = 5.64 ± 0.81, LDL = 3.38 ± 0.76, HDL = 1.39 ± 0.35 and TG = 2.04 ± 1.46). Such results might give an indication to the effectiveness of the hypolipidemic therapy (lovastatin monotherapy or in combination with gemfibrozil) in controlling diabetes dyslipidemia. Combination therapy of metformin with other antidiabetic agent (mainly sulfonylurea) was found in higher percentage than monotherapy in this study. A cross comparison between age and social activities was done, result revealed high proportional difference between two age groups against weight change, diet, exercise, smoking etc (refer to Table 2).
Uncontrolled FPG levels were significantly found more (83.3%) among patients on combination therapy (Table 3). This statistical significance might indicate that metformin can give better therapeutic effect when it is used as monotherapy than in combination with other antidiabetic drugs. In Chien et al 24 clinical trial, metformin combination with glyburide produced more reduction in FPG than monotherapy. This could be attributed to differences between the cohorts of the two studies regarding compliance to medication and patients’ follow- up.
Our study showed that the highest rank of patients with controlled lipidemia was significantly found among those on lovastatin monotherapy (Table 4). In a study conducted by Bell, 10 lovastatin therapeutic dose (20–40 mg/day) reduced significantly TC, HDL, TG and LDL levels from baseline to the controlled levels. These results could be attributed to the small sample size of the study. In the present study, the evaluation of lipid levels was done according to the latest value available in patients’ medical record. Unfortunately, not all patients had annual lipid profile follow- up compared to other studies. As well, there were no satisfying medical recordings regarding patient compliance to therapy and diet. This study finds that 76.2% of the patients with uncontrolled FBS had uncontrolled hypertension as well.
The complications associated with diabetes are appalling. It is estimated that about 15,000 to 39,000 people lose their sight because of diabetes and about 14.6% of NIDDM aged 40 years and above, developed diabetic retinopathy after 5 years duration of diabetic condition. It is also estimated that 10% of diabetes develop kidney disease and 50% develop evidence of nerve damage after over 25 years of having diabetes. People with diabetes are 2 to 4 times more likely to have heart disease and 5 times likely to suffer a stroke. The risk of leg amputation is 27.7 times greater and the occurrence of impotence due to diabetes neuropathy, among men is one third of male diabetics. It should be stressed that early detection in asymptomatic individuals provides an opportunity in attempting to prevent or delay the complication of diabetes through dieting and pharmacological measures to achieve euglycaemia. 25
Hence, it is important that prompt and effective treatment is made available to diabetics. There are 4 major components in the management of diabetes mellitus namely, diet, exercise, medication and education. Nonpharmacologic treatment (diet and exercise) must be attempted for at least 3 months before drug treatment is introduced in ambulant uncomplicated and especially obese diabetics. In addition, monitoring for diabetic control and management of complications should be emphasized. 25
According to gender, females showed higher mean FPG values but with no significance (Table 5). In a previous study conducted by Kobayashi et al 26 similar result was obtained in which females none significantly had higher FPG levels (14 ± 4.4 mmol/l) than males (13.8 ± 4.2 mmol/l). A significant difference was found in the present study between both genders regarding TC and HDL levels. Females exhibited higher values of the two former lipid parameters than males. As well LDL levels were higher in females, but without significance. Except for TG, higher values were found in males with no significance (Table 4). Similarly, Kobayashi et al 26 found that females had higher HDL levels (1.43 ± 0.5 mmol/l) than males (1.19 ± 0.3 mmol/l) significantly and no significant difference was obtained between both genders in LDL values. However, TG levels were significantly higher in males (2.22 ± 1.02 mmol/l) than females (1.59 ± 1.04 mmol/l) and TC levels were more elevated in males (5.68 ± 1.2 mmol/l) than females (5.35 ± 1.2 mmol/l). These variations between both genders in lipid profiles are most probably due to different circulating levels of sex hormones, particularly estrogens and androgens in females compared to males. It has been reported that females had higher production rates of than males. Apo A-I is the main apoprotein for HDL, which its levels and production rates together with Lp A-I increase with estrogen administration. 27
Differences between gender regarding FPG, TC, HDL, TG and LDL latest levels.
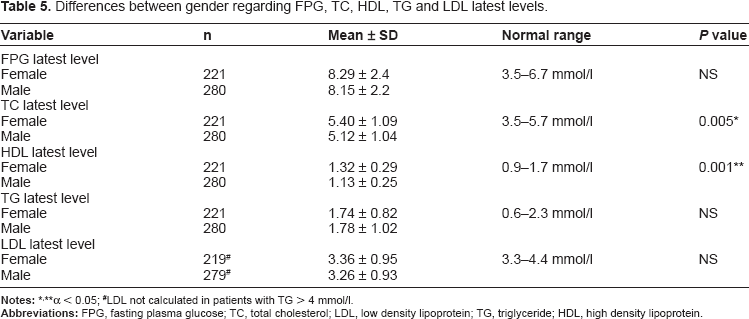
α < 0.05;
LDL not calculated in patients with TG > 4 mmol/l.
Different researches have shown that lower regimen adherence can be expected when a health condition is chronic, when the course of symptoms varies or when symptoms are not apparent, when a regimen is more complex, and when a treatment regimen requires lifestyle changes 28 Studies with diabetic patients indicate better adherence to medications than to prescribed lifestyle changes 29 and better adherence to simpler regimens than to more complex ones.30,31
We concluded from our study that ethnic difference regarding diabetes control was found to be significant between Malay and Chinese in which the Malay had higher mean FPG. In a study performed by Ng et al 31 Malay were significantly associated with the poorer glycemic control as they had the highest HbA1c levels in comparison with Chinese and Indians. However, in our study FPG monitoring was used to assess glycemic control and not HbA1c. Moreover, a significant variation was found between Chinese/Malay and Chinese/Indians in HDL levels. Chinese were with the highest HDL at the latest levels. This might be due to differences in insulin sensitivity.32,33 There were no significant differences found among the three races regarding TC, TG and LDL latest levels. In a study done by Ismail et al 32 Malays showed the highest TC and LDL levels (mean 6.19 mmol/l and 4.16 mmol/l respectively). In addition, Chinese had the highest HDL values than other races (mean 1.24 mmol/l).
In both studies controlled HDL levels were found more within Chinese race significantly. This might give an indication to a good lipidemia control among Chinese as HDL is considered a cardio protective lipoprotein and according to ADA and Malaysian-MOH guidelines, rising HDL level is the second strategy in the treatment of diabetes dyslipidemia.34–36
Limitations of the study
As a retrospective data was unavailable to identify the BMI influence on individual subject. The subjects were enrolled according to the completeness of medical profile, so this can cause a possible bias in term of selecting the subjects with incomplete medical follow-up/record. Study can not suggest any risk ratios as the data was collected retrospectively so limitations lies on data analysis.
Patient noncompliance is attributed to personal qualities of the patients, such as forgetfulness, lack of will power or discipline, or low level of education. The concept of noncompliance not only assumes a negative attitude toward patients, but also places patients in a passive, unequal role in relationship to their care providers. This study did not involve a prospective interview-type structured methodology, so identifying compliance issues in a cohort of retrospective data is a problem.
Conclusion
In conclusion, this study showed that both metformin and lovastatin were effective in reducing elevated glucose and lipid values. However, for glucose levels, the values were still above the normal limit used by the hospital. Furthermore, the study showed that the majority of patients with controlled FPG levels were receiving metformin monotherapy, unlike those who were on a combination regimen. Lovastatin was effective in reducing elevated lipid levels to values which are within the normal range. There was no difference between males and females in response to therapy, except for TC and HDL levels in which females exhibited higher levels for both lipid profiles than males. Among the multiracial study population, Chinese had the most controlled HDL levels and Malay had the highest uncontrolled FPG levels.
Recommendation(s)
This study recommends more frequent follow- up and therapeutic monitoring for the patient's condition by the health practitioners to determine the appropriate compliance with therapy and to control diabetes and dyslipidemia as per needed with therapeutic goals. More details about patients’ demographic data, social and lifestyle habits are needed to be recorded in the medical records.
List of Acronyms
Type 2 diabetes mellitus (DM2); Blood pressure (BP); Total cholesterol (TC); triglycerides (TG); HDL-cholesterol (HDL-C) levels; also on BP and body mass index (BMI); United Kingdom Prospective Study UKPDS; Fasting blood glucose (FBG); Statistical Package of Social Sciences (SPSS); American Diabetic Association (ADA); Ministry of Health Malaysia, (MOH).
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.