
Abstract
Our test results documented that hair and urine mineral analysis results support each other. This is of interest, because hair analysis evaluates past exposure while urine analysis detects immediate exposure.
We evaluated barium, cadmium, manganese, lead and uranium in hair and urine. Our test results indicate that all of the children show evidence of past and immediate exposure to one or more metals.
Hair mineral test results for the 114 children aged 12 and younger showed some type of toxic metal exposure for each one of the children; 88% exceeded the uranium reference range for hair. This indicates past and chronic exposure.
After renal evaluation, 55 children aged 3–12 years who passed certain criteria were selected for urine baseline testing. Urine baseline concentrations are a direct reflection of immediate exposure. Of the 55 children, 47 showed elevated urine concentrations for one or more of the toxins listed above, demonstrating immediate exposure.
DMSA is recommended as an oral antidote for lead and other metals. We selected 55 children aged 3–12 for a DMSA (Dimercapto succinic acid) urine challenge test. Our results showed that 98% of this group showed lead concentrations above the baseline level, demonstrating lead binding and excretion. The DMSA challenge did not affect barium, cadmium, manganese and uranium, suggesting that for these elements, DMSA may not be the chelating agent of choice.
In summary, hair and urine mineral testing demonstrated that chronic and immediate toxic exposure had affected our test group of Punjabi children. The DMSA challenge test was effective in detoxifying lead, but did not affect barium, cadmium, manganese or uranium.
Background and Introduction
Toxic metal exposure is a topic of concern to the Indian health care system, especially the environmental exposure of children.
We were contacted by therapists from the Children's Center of Faridkot in Punjab, India. People in the area had been alerted by media information suggesting toxic metal exposure as a cause of the rise in neurological disorders. Numerous publications pointed out that India serves as the toxic dumping ground of Europe and the United States. A BBC news article from 11 September 2000 stated “More than 100,887 tons of hazardous and potentially hazardous wastes entered illegally into India in 1998–99”. 1 Common products dumped are lead waste, used batteries and cadmium. Uranium and uranium waste is another concern. Due to India's geological formation, uranium is found in the water and soil of certain regions.
Punjab is one of the smallest states of India with an area of 50,362 sq km. It is situated in the northwestern part of India, bordering Pakistan. Punjab's natural ecosystem, rich in animal and plant life, is facing problems. Continuous use of herbicides, pesticides and large volumes of fertilizers affect the ecological quality of soil and water. While no uranium mining is reported in Punjab, coal mines may be a uranium source.
This study was developed to determine if chronic and/or acute metal exposure is affecting the children of Punjab. We selected hair mineral analysis to detect chronic and past metal exposure, and urine mineral analysis to document immediate exposure. After renal evaluation, a test group of children was subjected to a DMSA urine challenge test to prove that oral metal detoxification can be a treatment option.
Methodology and Explanation
Phase 1
Hair mineral analysis (HMA) evaluates long term metal exposure. Considerable research has documented the validity of HMA for the diagnosis of metal overexposure at an early stage.2,3 Degner et al used hair analysis to verify a patient's long term manganese intoxication 4 , while Melaku et al verified that hair and serum zinc values both confirm the zinc status of Ethiopian children. 5 Ilhan et al reported in 1999 that serum and hair analysis suggest that the changed element status (Zn, Mg and Cu) in hair plays an indicator role in the diagnosis of epileptic patients. 6 Bryne and Benedik of the University of Llubljana compared uranium levels of blood, hair and urine of occupationally exposed and non-exposed test persons, and concluded that hair shows promise as an indicator of exposure. 7
We decided to use this non-invasive test as a starting point to locate chronic exposure.
At the request of the Baba Farid Center staff at Faridkot, Punjab, and after all test persons and/or their legal guardians gave their written consent, 149 hair samples were collected at the Center. Sample preparation and testing was performed in Germany, in cooperation with the analytical team of Labor Friedle of Regensburg. All samples were washed with a de-ionized detergent, rinsed three times with de-ionized water and dried before weighing. Samples weighed around 100 mg, with sample weights varying between 94 mg and 116 mg.
For sample digestion, certified metal-free acids were used. Digestion took place in a closed-vessel microwave digestion system. Ultrapure water was used for final sample dilution and testing was performed via inductively coupled plasma with mass spectrometry (ICP-MS) utilizing collision/reaction cell methods coupled with ion-molecule chemistry, a relatively new method for interference reduction. 8 Statistical evaluation of data included a comparison of a 95th percentile of test values for children and adults and compared these to existing 95th percentile reference ranges for children and adults. Certified hair standards and in-house standards were used as part of the laboratory validation of results.
Phase 2
We ‘prepared’ our test group for a one-time Dimercapto succinic acid (DMSA) challenge test.
DMSA is an oral chelating agent that is considered safe for children. 9 Unlike other chelating agents, it does not significantly bind nutrient elements, although a study by Yingjun Liao of China Medical University, Shenyang, suggests that micronutrient provision potentiates the chelating efficacy of DMSA. 10
The Faridkot Center was thus supplied with DMSA and with nutritional supplements including a multimineral-vitamin-amino acid complex in powder form and zinc gluconate in1 5 mg capsules. Clinic staff members were in charge of distributing nutritional supplements to the test group. The patients were on a program of supplements for three months prior to the DMSA urine challenge.
Phase 3
Criteria for inclusion into Phase 3
Parental written consent
Age: 6–12 years
Health: renal function and normal blood chemistry tests. These were performed at Bagi Clinical Laboratory, Faridkot and the Charitable Hospital, Distr. Kapurthalla. The following tests were part of the criteria:
B. urea
Serum creatinine
Serum bilirubin
Serum alkaline phosphatase
SGOT
SGPT
Serum calcium
Serum sodium
Serum potassium
Of the initial 149 test persons, 55 children aged 6 to 12 years passed the criteria for inclusion and were admitted into Phases 3–4.
To avoid contamination, all urine collection cups and tubes had been provided by the Center by Micro Trace Minerals Laboratories, Germany. At the laboratory, samples were digested with certified metal-free acids involving closed-vessel microwave digestion. For sample dilution ultrapure water was used. Testing was performed via ICP-MS as outlined under Phase 1. Certified urine standards and in-house standards were used to validate results.
Urine test values were compared with reference ranges provided by the German Environmental Protection Agency (UBA). 11 Statistical data evaluation included a comparison of test values to existing reference ranges for children and adults.
Results
Hair mineral analysis (HMA)
The clinical staff at the Baba Farid Centre selected all test persons after properly informing patients and parents. Legal consents were received.
During Phase 1 of the research, hair mineral analysis was performed to evaluate the long term metal exposure of 149 test persons, 114 of whom were younger than 12 years of age. As no Environmental Protection Agency (EPA) provided reference ranges for hair, Micro Trace Minerals Laboratories had developed reference ranges for adults and children, following standard procedures as recommended by American and German/European laboratory regulations as early as 1984. Reference updates were initiated on a two-yearly basis.
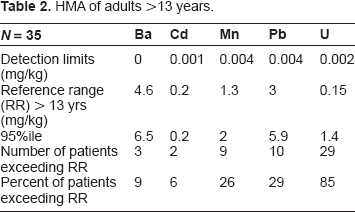
From the test results (N = 149), we established a 95th percentile for people 13 years of age and older (N = 35; the “adult” group) and compared these to available 95th percentile reference ranges. The 95th percentile patient value for cadmium (Cd) was within limit; for the metals barium (Ba), manganese (Mn), lead (Pb) and uranium (U), the 95th percentile patient values exceeded the reference ranges.
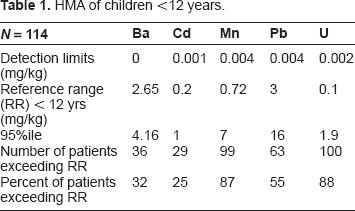
The 95th percentile values for children age 12 years and younger (N = 114) exceeded reference ranges for all metals (see Tables 1 and 2).
HMA of children <12 years.
HMA of adults >13 years.
Barium
Further comparison showed that in the adult group, 9% exceeded the adult reference range; in the children's group, 32% exceeded the reference range for children.
The 95th percentile test value for the children's group was 4.16 mg/kg compared to a 95th percentile reference range of 2.65 mg/kg.
Barium is a heavy metal that enters the air during mining and refining processes, and during the production of barium compounds. It can also enter the air during coal and oil combustion. Exposure to barium occurs mostly in the workplace or from drinking contaminated water. Ingesting drinking water containing levels of barium above the EPA drinking water guidelines for relatively short periods of time can cause gastrointestinal disturbances and muscle weakness. Ingesting high levels for a long time can damage the kidneys.12,13
Cadmium
Quarter (25%) of the children and 6% of the adults in our study exceeded the reference range. The 95th percentile test value for the children group was 1 mg/kg compared to a 95th percentile reference range of 0.2 mg/kg.
Eating food or drinking water with very high cadmium levels severely irritates the stomach, leading to vomiting and diarrhea. Cadmium overexposure may damage the kidneys, and contribute to anemia, liver disease and nerve damage. However, the Agency for Toxic Substances and Disease Registry (ASTDR) admits that it has no solid information that indicate what levels of cadmium cause these diseases.12,14
Manganese
In our sample, 87% of the children <12 years of age and 26% of the adults exceeded the appropriate reference range. The 95th percentile for the children's group was 7 mg/kg compared to a 95th percentile upper reference range of 0.72 mg/kg.
Manganese is an essential trace element, and ingesting small amounts from food or water is needed to stay healthy. Exposure to excess levels of manganese may occur from breathing air in areas where manganese is used in manufacturing. Excessive exposure can cause damage to the brain.12,15
Lead
Around half (55%) of the children <12 years of age and 29% of the adults exceeded the appropriate reference range. The 95th percentile test value for the group of 114 children was 16 mg/kg compared to a 95th percentile reference range of 3 mg/kg.
Exposure to lead can happen from breathing workplace air or dust, eating contaminated foods or drinking contaminated water, which may come from lead pipes in homes. Children can be exposed by eating lead-based paint chips or playing in contaminated soil. Lead is also a stable element of the uranium decay chain. Lead can damage the nervous system, kidneys and the reproductive system. The Centers for Disease Control and Prevention (CDC) recommends that children are tested as early as at ages 1 and 2 years of age. EPA limits lead in drinking water to 15 μg per liter (= 0.015 mg/L).14,16
Uranium
In our sample, 88% of the children <12 years of age and 85% of the adult group exceeded the respective reference range. The 95th percentile for children was 1.9 mg/kg compared to a reference range of 0.1 mg/kg, exceeding the recommended levels about 20-fold.
Uranium occurs naturally and is mildly radioactive. While everyone is exposed to low amounts of uranium through food, air, and water, overexposure can cause kidney disease. Uranium is not known to cause cancer, but can decay into other radioactive materials that may.14,17
To summarize, the hair metal test results for the 114 children aged 12 and younger showed some type of toxic metal exposure for each one of the children. This indicates that chronic exposure had affected them all.
Baseline urine test results versus DMSA challenge test results
After renal evaluation, 55 children aged 3–12 years who passed the criteria were selected for urine baseline testing. Of the 55 children, 47 exceeded reference ranges for one or more of the toxins analyzed, demonstrating immediate exposure.
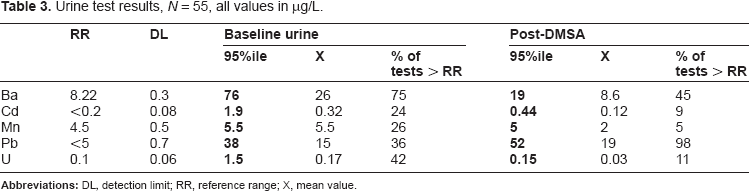
The reference ranges for the metals cadmium, lead and uranium are provided by the German EPA; for barium and manganese, we developed a 95th percentile from a healthy test group as outlined by standard laboratory regulations (see Table 3).
Urine test results, N = 55, all values in μg/L.
DMSA (trade name Chemet) has been initially approved by the US Food and Drug Administration in 1991 for the treatment of lead poisoning in pediatric patients. 18 In Russian literature, DMSA is named Succimer. Germany's poison center, GIZ Nord, lists DMSA as an official antidote for the treatment of lead, mercury and arsenic intoxication. 19 Environmental researchers at the University of Cincinnati documented that DMSA treatment improved muscle functions associated with postural balance and movement in lead-exposed children. 20 The recommended treatment dose is 10–30 mg/kg body weight. For the one-time challenge test, we stayed with the lower dose.
Baseline urine
The 95th percentile of all metals tested exceeded the 95th percentile reference range (Table 3).
DMSA challenge test results
The DMSA challenge only increased the urinary lead excretion above baseline levels (Table 3). The DMSA challenge did not affect barium, cadmium, manganese and uranium, suggesting that DMSA may not be the chelating agent of choice for these elements.
Conclusion
The results of this study demonstrate that our test group from the Faridkot Children's Center have been affected by immediate and chronic metal exposure.
ICP-MS hair mineral analysis confirmed long-term exposure for barium, cadmium, manganese, lead and uranium, with the children's hair values exceeding reference ranges more than the adult group, indicating that chronic metal exposure affects children more than adults (see Tables 1 and 2).
Baseline urine testing confirmed immediate exposure for all elements tested.
The DMSA challenge test resulted in an increase in urinary lead excretion, demonstrating that DMSA can be of therapeutic value to lead-exposed children. The DMSA challenge did not affect barium, cadmium, manganese or uranium, suggesting that oral DMSA is not the appropriate chelating substance for these metals.
The comparison of hair mineral results and baseline urine concentration provided diagnostic information in support of each other. This documents that both tests are confirming and valuable diagnostic tests.
Since hair and urine mineral analysis are noninvasive, these laboratory tests seem particularly suitable for the diagnosis of chronic metal exposure in children.
Discussion
Early diagnosis of metal exposure can prevent the onset of serious metal-related health problems, and should be in the interest of governmental health care agencies and health care providers.
Through our study, we confirmed that chronic and immediate metal exposure affects the children in the Punjab region. Alerted by the media after our work started, the Atomic Energy Regulatory Board tested hair samples taken from patients at the Baba Farid Center for Special Children in Faridkot, Punjab. VD Puranik of the Atomic Energy Regulatory Board stated that their results indicate that concentrations were within recommended limits, which is in clear contrast to our data. To substantiate this statement, we suggest a follow-up study and a comparison of methodology and reference ranges. Most likely, different methods and reference ranges account for the discrepancy in data interpretation.
Based on our results, we suggest early screening for metal exposure of children, as has been suggested by the CDC in 2000. 21 While the Advisory Committee on Childhood Lead Poisoning Prevention focused on routine blood testing for children, 21 our study indicates that non invasive testing through hair and urine analysis may be equally or more appropriate. Our data demonstrates that hair would be suitable in diagnosing chronic exposure. Urine metal testing is useful in detecting immediate exposure. Our data also supports the study by Bryne and Benedik that indicates that hair and urine are useful diagnostic tools in the evaluation of uranium exposure. 7
DMSA challenge tests are another diagnostic option. A challenge test demonstrates that metal binding and excretion take place, allowing physicians to monitor detoxification treatments. While our study confirmed that oral DMSA is a useful chelating substance for the treatment of lead intoxication, 22 we could not substantiate information listing DMSA as an antidote for uranium exposure. 23
To locate the Punjabi children's source of exposure, we suggest water and soil testing to identify geographic locations which may be considered high risk environmental areas. In fact, the Indian Atomic Energy Regulatory Board initiated water testing in the Punjab area, particularly evaluating uranium concentrations. Official statements concluded that no problem was found.
A comparison with the EPAs’ maximum contaminant levels may be appropriate. Such comparisons may place the Indian analytical data in a different light. For example, the German Bundesumweltamt (UBA) has set a MCL for uranium in drinking water of 10 μg/L; the EPA lists a MCL of 30 μg/L. An analysis of drinking water by the departments of physics and chemistry at Guru Nanak Dev University in Amritsar, Punjab, listed uranium concentrations in water samples varying from 1.65 ± 0.06 to 74.98 ± 0.38 μg/L. The authors concluded that these values when ‘compared with safe limit values are safe for drinking water’. 24
We also find it important to compare reference ranges for biomonitoring of hair, blood and urine. The discrepancy in reference ranges as utilized by various organisations can cause confusion among patients and physicians. Environmental health problems are easily ignored or overlooked. We suggest cooperation between laboratories and the appropriate governmental agencies, and we find it important to initiate follow-up studies that evaluate early metal exposure in children who live in industrial or otherwise environmentally endangered regions.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgements
This study was funded and supported by individuals. It is our hope that this study provides valuable information that hopefully results in follow-up studies, which are much needed.
It should be acknowledged that during the past three years, the laboratory team scored near 100% in all governmental “round robins” scheduled for laboratory licensing requirements. All those involved worked with extreme care and without compensation.
We thank Dr. Preet Chou and the staff at the Faridkot Children's Center for their involvement and help.