
Abstract
The overactive bladder (OAB) is a debilitating condition in which patients suffer from urinary urgency, frequency and nocturia with or without urge urinary incontinence. The mainstay of pharmacotherapy for OAB is muscarinic receptor antagonists, which have been shown to be effective treatments for the symptoms of OAB. The mechanism underlying the efficacy of antimuscarinic agents against the symptoms of OAB is not completely understood. This review explores the role of bladder mucosal muscarinic receptors in the signaling pathways that are activated in response to bladder filling. The cholinergic system is seen to be involved in bladder afferent signaling at many levels and as such muscarinic receptor antagonists may affect bladder signaling via numerous pathways including release of mediators from the bladder urothelium and activation of suburothelial myofibroblasts and afferent nerves. Therefore the mucosal cholinergic system may represent another target for the antimuscarinic agents used to treat OAB.
The urinary bladder is a largely unappreciated organ. In normal adults, the urinary bladder performs the vital functions of storing the body's liquid waste and then voiding that waste at a time of our choosing. During the storage phase, the bladder accommodates approximately 500 mL of urine with the bladder wall stretching without any great increase in pressure and without detrusor muscle contractions being initiated. At full capacity, the afferent nerves lying within the bladder wall signal fullness to the central nervous system and at a convenient time voiding is initiated. During voiding, the pelvic floor muscles relax, and the detrusor muscle contracts until the pressure inside the bladder exceeds urethral pressure, at which point voiding occurs. For the majority of individuals, this occurs, about seven or eight times each day, without any real thought. However for the approximately 17% of men and women over the age of 40 years who suffer from an overactive bladder (OAB) this normal activity of the bladder is disrupted.1,2 Surprisingly, the disruption of bladder function associated with OAB is more prevalent than other chronic conditions such as heart disease, asthma and arthritis. 2
Overview of the Overactive Bladder
The overactive bladder (OAB) is a debilitating chronic disorder. In 2002, the International Continence Society defined this condition, in which patients typically experience symptoms of urgency (a sudden compelling desire to void that cannot be deferred), usually with frequency (voiding more than eight times in 24 hours) and nocturia (being woken at night with the desire to void), with or without urge incontinence (the involuntary leakage of urine associated with urge). 3 OAB is a chronic disease with a major negative influence on quality of life, especially associated with the limitations it places on physical and emotional health, vitality and social functioning. 4 The symptoms of OAB affect all aspects of life including: social (limiting outings due to frequent need to urinate), psychological (loss of self esteem associated with incontinence), physical (limitations of physical activities due to fear of incontinence) and occupational (decreased productivity). 3 OAB can also be associated with economic costs including the personal costs of managing incontinence, the treatment costs associated with managing symptoms and providing care for incontinent nursing home residents and costs associated with decreased work productivity. In the US, the economic costs associated with OAB in the year 2000 were estimated to be between $12.02 and $17.5 billion. 4 This makes the economic impact of OAB comparable to the economic impact of influenza, arthritis and osteoarthritis. 4
As can be seen from the 2002 definition the cornerstone symptom of OAB is urgency.1,5,6 Urgency is usually associated with frequency of urination, nocturia and urge urinary incontinence although only about one third of patients with OAB will experience incontinence.2,7 In incontinent patients, urodynamic testing demonstrates detrusor overactivity, where urine leakage arises from involuntary detrusor contraction. 8 The aetiology of these involuntary detrusor contractions remains unknown.
There are numerous treatment options available for patients with OAB including biofeedback, electrical stimulation, bladder training and pharmacotherapy, either alone or in combination. However, the primary treatment for the OAB is pharmacotherapy with muscarinic receptor antagonists.9–11
Bladder Physiology and the Role of Muscarinic Receptors
The traditional dogma behind the treatment of OAB with muscarinic receptor antagonists was based on our understanding of the nerves controlling contraction of the bladder detrusor muscle. During filling, the bladder detrusor muscle is relaxed, expanding at low pressure. During voiding the parasympathetic nerves release acetylcholine onto muscarinic receptors located on the detrusor muscle, causing it to contract. 12 Muscarinic antagonists were thought to inhibit the activation of these detrusor muscarinic receptors and hence inhibit contraction.
There are five subtypes of muscarinic receptors (M1–M5) that have been cloned and pharmacologically characterised. 13 Muscarinic receptors are G-protein coupled receptors. Muscarinic M1, M3 and M5 receptors are coupled to activation of phospholipase C and IP3 production leading to release of calcium from intracellular stores. 14 In contrast, M2 and M4 receptors are coupled to inhibition of adenylyl cyclase leading to a decrease in cAMP and to inhibition of calcium-activated potassium channels. 14 In the urinary bladder, binding and immunoprecipitation studies15–18 on human detrusor muscle have demonstrated that the majority of muscarinic receptors are M2 receptor (~70%) with small populations of M3 (~20%) and M1 (~10%) receptors. 18 Functional studies carried out in M3 knockout mice 19 and human detrusor strips20,21 have demonstrated that the small population of M3 receptors are primarily responsible detrusor contraction. Nevertheless, there is some evidence from studies in M2 knockout mice that the large population of M2 receptors have some functional importance.14,22 M2 receptors enhance the contraction mediated by M3 receptors and inhibit relaxation via a decrease in cAMP.23,24
The wall of the bladder also contains a mucosal layer. The bladder mucosa is made up of the urothelial cell layer, that lines the lumen of the bladder, and the lamina propria containing blood vessels, nerves and suburothelial myofibroblasts. The bladder urothelium is a folded transitional epithelium that expands and unfolds as the bladder volume increases. The urothelium is made up of large surface umbrella cells, intermediate cells and basal cells attached to the basement membrane. Historically, the urothelial cell layer was considered to be an inert layer, simply responsible for containing the urine within the bladder lumen. However, recent evidence has indicated that the bladder urothelium has neuronal and sensor properties 25 and plays a role in the regulation of the activity of the underlying nerve and muscle and as such is involved in the initiation of the micturition reflex.
During bladder filling, stretch of the bladder wall triggers the release of mediators (such as ATP) from the urothelium that signal bladder fullness via the underlying afferent nerves. 26 Signals from these afferent nerves are processed in the brain and, at an appropriate time, efferent parasympathetic nerves are activated. The control and integration of these afferent and efferent signals has been recently reviewed. 27
Within the bladder wall, muscarinic receptors have not only been identified on the bladder detrusor muscle but have also been localized to the urothelium and suburothelial myofibroblasts.18,28–32 Radioligand binding studies in both pig 32 and human bladder 18 have demonstrated M2 (~70%) and M3 (~30%) muscarinic receptors in the bladder mucosa. Mucosal muscarinic mRNA for M1, M2, M3 and M5 receptors have also been demonstrated using RT-PCR studies.18,29,31
Immunohistochemical studies have localised muscarinic receptor immunoreactivity to the bladder urothelium.29–31 Studies in the human 31 and mouse urothelium33 have demonstrated a differential distribution of muscarinic receptor subtypes within the various cell layers of the urothelium (see Fig. 1). While M2, M3, M4 and M5 receptors were found in all layers of the urothelium, the M2 receptors were concentrated in the apical umbrella cell layer and M1 receptors were found exclusively in the basal cell layer.31,33
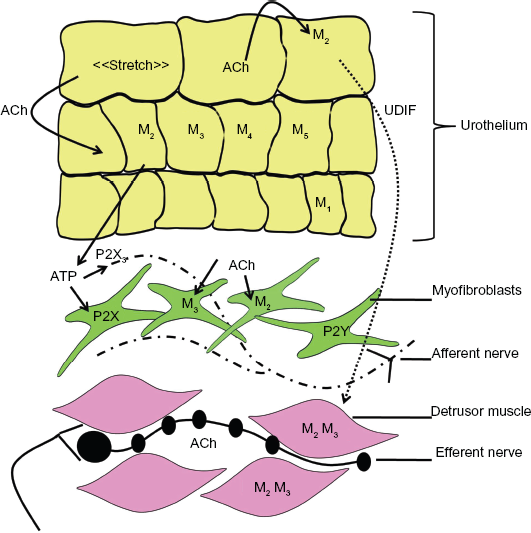
Possible mechanism for cholinergic signaling in bladder activity. During filling stretch of the bladder wall induces release of acetylcholine (and ATP) from urothelial cells. This acetylcholine may then activate urothelial muscarinic receptors which stimulates further release of ATP. Both acetylcholine and ATP may activate the suburothelial myofibroblasts via muscarinic or purinergic receptors which may in turn alter the activity of the associated afferent nerves. ATP can also activate afferent nerves directly via P2X3 receptors. This afferent nerve activity can then signal bladder fullness to the central nervous system which in turn activates the parasympathetic efferent nerves to release acetylcholine onto muscarinic receptors located on the detrusor smooth muscle leading to bladder contraction and voiding.
Muscarinic M2 and M3 receptors have also been localised to the suburothelial myofibroblasts.28,30 In patients with OAB, an increase in both M2 and M3 immunoreactivity on the suburothelial myofibroblasts was observed. 30 Interestingly the increased immunoreactivity correlated with the patients urgency scores 30 indicating a possible role for the muscarinic receptors located on the suburothelial myofibroblasts in the pathophysiology of urgency.
Antimuscarinic Agents show clinical Efficacy against the Symptom of Urgency
Muscarinic antagonists have been repeatedly shown to be effective against the symptoms of OAB (for a systematic review see reference 34 ). However, in contrast to the conventional belief regarding their mechanism of action, recent reports have suggested that at therapeutic doses muscarinic antagonists do not inhibit detrusor contractility.11,35 Despite this, these agents do function to increase bladder capacity and decrease urgency during bladder filling. 35 During filling there is no activity of the efferent parasympathetic nerves,36,37 hence, while muscarinic antagonists are effective treatments for OAB their actions cannot be attributed to inhibition of detrusor muscarinic receptors.
Since OAB was redefined in 2002 a number of studies have evaluated the effectiveness of anti-muscarinic agents against the symptoms associated with bladder filling, such as micturition frequency and urgency. Results from a number of these studies are summarised in Table 1. Studies included in this table were all 12 week, placebo controlled clinical trials that evaluated the effectiveness of some of the newer antimuscarinic agents (fesoterodine, solifenacin, tolterodine and trospium). The clinical outcomes included were micturition frequency, urge urinary incontinence and urgency episodes. These were determined from a three day bladder diary.
Efficacy of antimuscarinic agents used to treat OAB against micturition frequency, urge urinary incontinence (UUI) and urgency episodes.
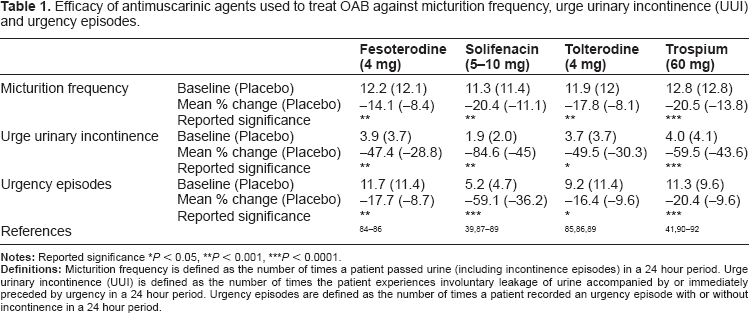
It can be seen from the review by Chapple 34 and the data summarised in Table 1 that treatment with all of the muscarinic antagonists included (fesoterodine, solifenacin, tolterodine and trospium) is associated with some reduction in micturition frequency with a mean reduction in micturition frequency greater than 14% reported for all of these agents (Table 1). These antagonists (fesoterodine, solifenacin, tolterodine and trospium) have also been shown to effectively reduce urge urinary incontinence (Table 1) with an almost 50% reduction in the number of urge urinary incontinence episodes at the conclusion of the 12 week clinical trials.
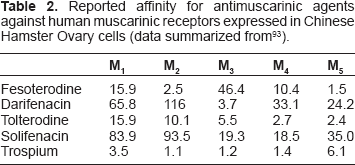
In addition to efficacy against micturition frequency and urge urinary incontinence, these antagonists have also been seen to reduce the number of urgency episodes per 24 hours (Table 1). Fesoterodine, tolterodine and trospium inhibit urgency episodes by approximately 17% while solifenacin reduces urgency episodes by 59%. The reasons underlying the improved efficacy of solifenacin against urgency are unknown. While it would be tempting to postulate that it may be related to the high degree of M3 receptor selectivity associated with solifenacin (Table 2), other agents with similar M3 selectivity (e.g. darifenacin, Table 2) are not associated with similar reductions in urgency episodes (darifenacin reduces the number of urgency episodes by 22%). 38
Reported affinity for antimuscarinic agents against human muscarinic receptors expressed in Chinese Hamster Ovary cells (data summarized from 93 ).
In addition to quantifying an effect on the number of urgency episodes, some studies have also evaluated the efficacy of antimuscarinic agents on the severity of urgency. Urgency severity has been evaluated according to PPIUS scale 39 in which each urgency episode is characterised with a score from 0 to 4; with 0 indicating no urgency, 1 mild urgency, 2 moderate urgency, 3 severe urgency and 4 urge incontinence. 39 Using scales such as this, muscarinic antagonists such as solifenacin, 39 darifenacin, 40 oxybutynin 40 and trospium 41 have been shown to reduce the severity of urgency episodes. Therefore, indicating that muscarinic antagonists not only reduce micturition frequency and urge urinary incontinence episodes but also the number and severity of urgency episodes.
These beneficial effects, on the symptoms of urgency, raise questions about how urgency is sensed. Urgency (a sudden compelling desire to void that cannot be deferred) is a pathological sensation 42 that is distinct from the gradual buildup of sensation that usually accompanies normal bladder filling. 6 However, insight into the processes underlying urgency can be gained from our understanding of the normal bladder sensations during filling.
Muscarinic Involvement in Afferent Processes in the Bladder Mucosa
It is believed that filling sensations from the bladder are mediated by afferent nerves located in the lamina propria of the mucosa. These afferent nerves (Aδ and C fibres) are closely associated with both the urothelium and the underlying layer of suburothelial myofibroblasts.43,44 These nerve fibres are activated by stretch and chemical stimuli45,46 with the myelinated Aδ fibres thought to be associated with normal micturition processes while the unmyelinated C fibres are thought to be responsible for sensations arising from painful stimuli.45–47
During filling, stretch of the bladder wall is associated with release of mediators from the urothelium.26,48–52 Some of these mediators, such as ATP 26 are thought to stimulate the underlying afferent nerves while others, such as nitric oxide (NO)53,54 are thought to be inhibitory.55,56 These mediators (ATP, NO) are therefore involved in the transduction of stretch of the bladder wall during filling, into activation of sensory afferent fibres.55,56 We have recently reported that the concentration of ATP in voided urodynamic fluid correlated significantly with voided volume in normal and overactive bladders 49 suggesting that stretch of the bladder wall during filling leads to an incremental release of ATP from the urothelium. ATP can then activate the underlying afferent nerves, with increased afferent nerve firing associated with bladder filling. 57 Afferent nerve activation occurs via ligand-gated P2X3 receptors.45,51,58 In knockout mice, loss of P2X3 receptors leads to decreased voiding frequency and increased bladder capacity. 58
In addition to activating the afferent nerves, ATP released from the urothelium can also activate purinergic receptors located on suburothelial myofibroblasts. These purinergic receptors may be either ligand-gated P2X receptors 59 or G-protein coupled, P2Y receptors. 60 Suburothelial myofibroblasts are closely associated with the afferent nerves of the lamina propria61,62 and may function to modulate and amplify the afferent nerve responses following stretch of the bladder wall.43,63
Stretch of the bladder wall has also been associated with release of acetylcholine.37,52,64 Acetylcholine release is not sensitive to the nerve toxin tetrodotoxin and is dependent on the presence of the urothelium, suggesting that the urothelium is a source of non-neuronal acetylcholine. 37 The urothelium has been shown to contain the cellular machinery required for the synthesis of acetylcholine, including choline acetyltransferase 52 and carnitine acetyltransferase.56,57,65,66 Acetylcholine is therefore another stimulatory agent released from the bladder urothelium.
Recent studies have demonstrated that antimuscarinic agents such as oxybutynin have an inhibitory effect on afferent nerve firing.56,57,66 Systemic administration of oxybutynin and darifenacin significantly decreased the firing rate of both Aδ and C fibres during bladder filling.57,66 Similarly, long-term administration of oxybutynin led to an increase in the micturition interval and increased bladder capacity together with decreased c-Fos expression in the spinal cord, which is associated with decreased activity of afferent nerves. 67 In contrast, intravesical administration of muscarinic agonists, carbachol and oxotremorine, leads to increased excitability of bladder afferents, as seen by a decrease in the inter-contraction interval.54,68,69 Although, instillation of low concentrations of oxotremorine was also associated with an inhibitory effect on bladder afferents mediated by NO. 54
Stimulation of the bladder mucosa by the muscarinic agonist carbachol also leads to the release of an as yet unidentified “urothelial derived inhibitory factor” (UDIF).32,70,71 Release of UDIF is mediated via activation of muscarinic M2 receptors. 72 UDIF released following activation of muscarinic receptors functions to directly inhibit detrusor muscle contractions. This effect can be observed in an organ bath and hence is independent of any stimulatory or inhibitory effects of muscarinic agonists on bladder afferent nerve fibres.
The mechanism underlying the effect of antimuscarinic agents on afferent nerve function remains uncertain, however it is likely to involve mucosal muscarinic receptors.18,28–32 A possible mechanism is summarised in Figure 1. Acetylcholine released from the urothelium in response to stretch52,64 could act in an autocrine or paracrine manner to stimulate urothelial muscarinic receptors and trigger the release of ATP. 50 The ATP released may then facilitate the generation of afferent nerve activity either directly, via P2X3 receptors, or indirectly via activation of purinergic receptors on located the suburothelial myofibroblasts. In addition, acetylcholine could also activate the muscarinic receptors located on the suburothelial myofibroblasts.28,30
Mucosal Muscarinic Receptors as Therapeutic Targets
Mucosal muscarinic receptors may therefore represent another target for antimuscarinic therapy. Following oral administration, antimuscarinic agents may gain access to mucosal muscarinic receptors via the bloodstream. In addition, any antimuscarinic agent excreted in the urine unchanged, or as an active metabolite, may have direct access to urothelial muscarinic receptors. 73 In vivo studies in rat bladder have suggested that antimuscarinic agents excreted in the urine may have therapeutic potential. In order to examine this, human volunteers were administered antimuscarinic agents (darifenacin, oxybutynin, solifenacin, tolterodine and trospium) at the regularly prescribed dose for 5 days. Samples of urine from these volunteers was then instilled into rat bladders and the effect on carbachol-induced detrusor overactivity monitored.68,69,74
Intravesical administration of urine from volunteers who took trospium prevented the reduction in bladder capacity and inter-contraction interval (detrusor overactivity) induced by carbachol.68,69 Similarly, urine from volunteers who took solifenacin was able to prevent carbachol-induced detrusor overactivity. 74 However, urine from volunteers who took oxybutynin,68,69 tolterodine68,69 or darifenacin 74 was unable to inhibit carbachol-induced detrusor overactivity. In all of these studies68,69,74 the urine was only instilled into the bladder for a short period of time in order to minimise any absorption across the mucosal wall and hence to remove any direct effects on the detrusor muscle itself.
Trospium and solifenacin are unusual in that pharmacokinetic studies have shown that a relatively high percentage of the administered dose is excreted in the urine unchanged (Table 3). It can therefore be concluded that the ability of some of the antimuscarinic agents to prevent carbachol-induced detrusor overactivity is determined by the actions of the unchanged drug and/or active metabolite excreted in urine. 73 Interestingly, in clinical trials these two agents (trospium and solifenacin) have been associated with the highest percentage reduction of the number of urgency episodes in a 24 hour period (20.4% and 59.1% respectively, see Table 1). However, urinary excretion of parent compound or active metabolite is not the only requirement for clinical efficacy. Darifenacin also reduces the number of urgency episodes by a similar percentage 38 although urine from volunteers taking darifenacin was unable to prevent carbachol-induced detrusor overactivity 74 and this agent is not excreted via the urine (Table 3).
Urinary excretion of antimuscarinic agents.

Current use of muscarinic receptor antagonists is limited by side effects such as dry mouth and constipation, that are associated with the binding of these agents to muscarinic receptors located in the salivary glands 75 and gastrointestinal tract.76,77 These side effects result in many patients discontinuing therapy 3 and may in part explain why long term clinical improvement is only seen in 35% of patients. 78 These side effects occur due to a lack of organ selectivity of antimuscarinic agents. 79 In the future, improvements in the bladder selectivity of muscarinic receptor antagonists may be achieved by developing muscarinic receptor antagonists that are targeted to the bladder mucosa via excretion in the urine or via intravesical administration. Some clinical efficacy has previously been obtained from intravesical instillation of oxybutynin in patients with OAB.80–82 In rats, intravesical administration of oxybutynin was associated with greater bladder selectivity 83 and as discussed above reduces stretch activated afferent nerve firing56,57,66 which may be associated with urinary urgency.
Conclusions
Over the last 15 years, antimuscarinic agents have been shown to be effective treatments for the symptoms of OAB including micturition frequency, urge urinary incontinence and urgency episodes. Previously this therapy was thought to target the muscarinic receptors located on the detrusor muscle, however, recent research indicates that this is not the case. The mechanism underlying the clinical efficacy of antimuscarinic agents against the symptoms of OAB is not completely understood. This efficacy is likely to involve interplay between the muscarinic receptors located in the bladder mucosa and mediators released from the bladder urothelium, including ATP and acetylcholine Figure 1. ATP and acetylcholine released from the urothelium may act on the suburothelial myofibroblasts and associated afferent nerves to mediate the sensations of bladder filling. Thus, the cholinergic system is integral to bladder afferent signaling and as such muscarinic receptor antagonists may affect bladder signaling via numerous pathways.
Disclosure
This manuscript has been read and approved by the author. This paper is unique and not under consideration by any other publication and has not been published elsewhere. The author reports no conflict of interest. The author confirms that they have permission to reproduce any copyrighted material.