
Abstract
Inflammatory Bowel Disease (IBD) treatments are rapidly evolving. Current knowledge of the immunopathology responsible for IBD grows on a daily basis. These scientific discoveries are quickly being translated into clinical advances for improved treatment of IBD patients. The breakthrough in biologic therapy occurred with the introduction of infliximab for the treatment of Crohn's disease. Since then, research applying biologic therapies for IBD has expanded dramatically. Even though significant therapeutic gains have occurred with the expanded use of biologic therapies directed against tumor necrosis factor (TNF)-α, some patients still remain underserved by this type of treatment. Clinicians need to be familiar with alternative biological therapeutics to so that patients will have an opportunity to benefit from this effective class of medications. This review will highlight the advances made in integrin inhibitor therapy, and discuss the application of this therapy to an IBD treatment paradigm.
Introduction
Inflammatory bowel disease (IBD), comprised of both Crohn's disease (CD) and ulcerative colitis (UC), stems from an inappropriate response of the mucosal immune system to intestinal flora and other luminal antigens found in the intestinal ecosystem. 1 The uncharacteristic dysregulated response (dysbiosis) most likely results from the three-way intersection of genetic, environmental, and immunologic factors. 2 This “perfect storm” results in chronic waxing and waning inflammation that usually lasts a lifetime. Uncontrolled inflammation can result in serious complications, such as mega-colon, perforation, abscess, fistula formation, or fibro-stenotic disease.
Mild to moderate cases of IBD are typically managed with aminosalicylic acid compounds, immunomodulators such as azathioprine, 6-mercaptopurine or methotrexate, or corticosteroids. 3 Regrettably, a significant number of patients affected by CD and UC either fail to respond to standard treatments, or lose response after a variable period of time. Medical refractoriness often results in debilitating complications, impaired quality of life, and need for surgery. In addition to the disease related complications encountered by IBD patients, many therapeutic options, including immunosuppressants and corticosteroids, can induce significant side-effects that may counterbalance long-term benefits. 4
Recent advances in our understanding of the inflammatory processes responsible for IBD have spurred the discovery of biologic agents targeted against specific pathways. Targeted therapy holds great promise for improving the management of IBD. Tumor necrosis factor alpha (TNFα), an inflammatory cytokine, is found at elevated levels in many autoimmune disorders, including IBD. 5 Antibodies against TNFα have demonstrated efficacy against moderate-to severe CD. The success of infliximab set the stage for the development of two additional TNFα inhibitors, adalimumab and certolizumab. Even with the roll out of multiple anti-TNF antibody therapies, approximately 30% of CD patients who find themselves refractory to standard treatment also do not respond to induction therapy with TNF-α inhibitors. Even more unsettling is the fact that of those who initially respond, 50% or more cease to respond within a year.6–8 Finally, the use of anti-TNF agents is hampered by both immunogenicity and a risk of significant complications, including opportunistic infections, hematologic and skin malignancies, neurologic disorders, hepatic dysfunction and congestive heart failure.6–8
Clearly, additional therapies based on other pivotal pathways in the inflammatory cascade are necessary to effectively treat patients with IBD. This review will expound upon the class of medications specifically targeting the trafficking of activated lymphocytes by inhibiting the action of integrins. The integrins consist of a class of molecules important in the activation and recruitment of tissue specific T-lymphocytes, which contribute heavily to the continuation of an established inflammatory process. The success of this class of molecules provides an exciting opportunity to fill the gap left after patients fail standard therapy and anti-TNF agents. Therapies targeting integrins may ultimately result in steroid-free remission for those patients experiencing refractory disease despite the administration of commonly used therapies.
IBD Background
IBD immunopathology
Components of the mucosal ecosystem which play an active role in IBD include resident microbes contained within the intestinal lumen, mucosal epithelial cells, innate immune cells (macrophages and granulocytes, which recognize general pathogen motifs through pattern-recognition receptors), and adaptive immune cells (T-lymphoctyes) (Fig. 1). Disruptions of the mucosal ecosystem homeostasis likely arise from a perturbation of the complex interaction of genetic factors,1,9–12 abnormal stimuli from the host's indigenous flora,1,13 and dysregulated innate and adaptive immune responses against the same.1,9,11,12
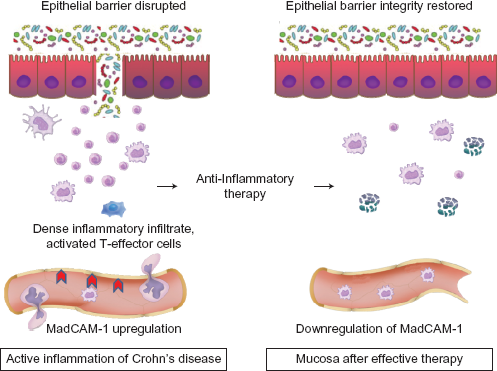
Immunobiology of inflammatory bowel disease. 33
The raising of an adaptive immune response involves the recruitment, activation, and subsequent differentiation of naïve (T0) lymphocytes into helper or effector T cells (Th1, Th2, and Th17) and regulatory T cells (Treg). The differentiation process is controlled by professional antigen-presenting cells (dendritic cells and a sub-type of tissue macrophages). In IBD, the differentiation process is skewed toward an inflammatory function which is relatively unopposed by a regulatory component. CD is associated with over-abundance of overactive Th1 and Th17 effector cells, while UC is more highly associated with overactive Th2 effector cells.
Lymphocyte trafficking and adhesion molecules
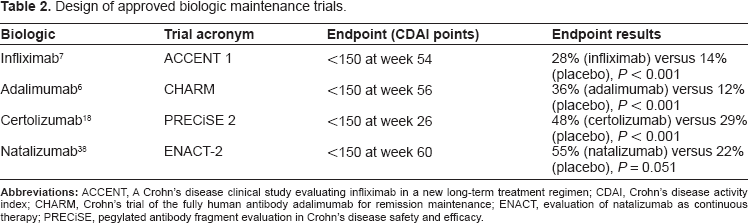
Depending on class of cell, different components of the immune system follow different life-cycles. Based on tissue independent chemotactic factors, neutrophils rapidly migrate to inflamed tissues, perform their function, and undergo apoptosis. Circulating monocytes infiltrate inflamed tissues in a similar fashion, with a portion establishing themselves as resident macrophages. Naïve lymphocytes, on the other hand, continuously circulate through the body, looking for their cognate antigen presented in the context of the appropriate major histocompatability complex (MHC). Once the cognate antigen is detected, appropriate co-stimulatory signals cause differentiation of the activated lymphocyte into an effector cell. One component of the activation process involves the expression of a variety of cell surface receptors, including cytokine and chemokine receptors as well as adhesion molecules. The combination of cell surface proteins provide a tissue-specific homing mechanism for the return of the activated lymphocyte to its tissue of origin, 14 much as a spawning salmon returns to the stream of its birth. Normally, inflammatory processes abate as pathogenic antigens become eliminated. However, chronic inflammatory processes such as IBD persist due to the continuous replenishment of lymphocytes into the mucosal tissue. Lymphocyte trafficking occurs due to the effects of an elaborate system of immune cell surface adhesion molecules and their tissue-based receptors. 4 In the case of IBD, the leukocyte adhesion molecules α4/β7 and very late antigen-4 (VLA-4), a heterodimer of α4/β1 (CD49d/CD29), interact strongly with endothelial ligands, especially vascular cell adhesion molecule-1 (VCAM-1) and mucosal addressin cell adhesion molecule-1 (MAdCAM-1). The interaction between these molecules is central to the process of recruitment and trafficking of leukocytes into the intestinal mucosa. The binding of α4 integrin (dimerized with either β1 or β7) with its ligand provides a mechanism for firm adhesion, which is the process responsible for leukocyte resistance to shear forces generated by flowing blood. 15 Diapedesis across the vascular endothelium ensues (Fig. 2). This initial development is quickly followed by leukocyte migration into inflamed tissues. Pro-inflammatory cytokines (particularly TNF-α) upregulate expression of endothelial ligands, providing yet another enhancement to leukocyte recruitment and sustaining inflammation. 10
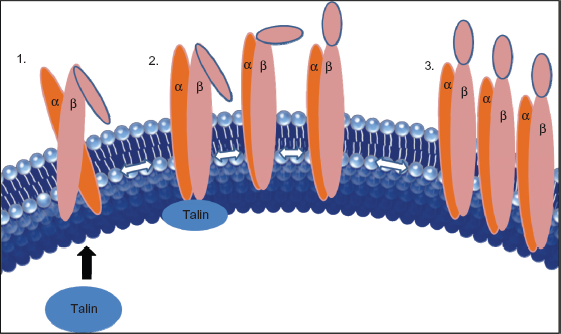
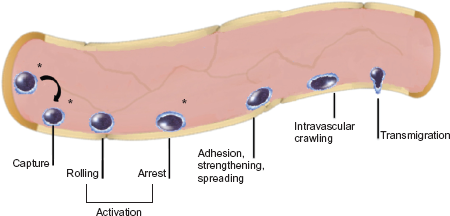
Agonist stimulated integrin activation. 1. Cell surface receptors bind agonist (eg, selectins and mucins), leading to signal transduction events culminating in recruitment of Talin to form the integrin activation complex. 2. Integrin affinity triggering. Talin binding enhances the molecular configuration of integrin monomers to increase the binding affinity for their ligand. 3. Lateral mobility of activated integrins leads to formation of clusters and increased binding energy.
Cytokine mediators
Activated Th1 cells found in CD produce interferon γ (IFN-γ), interleukin 12 (IL-12), and interleukin 23 (IL-23), which in turn stimulate macrophages to produce large amounts of TNFα, interleukin 1(IL-1), and interleukin 6 (IL-6). These subsequent inflammatory cytokines promote additional leukocyte recruitment from the mucosal vasculature, which produce even more inflammatory cytokines. The result of this destructive cycle ultimately amplifies the inflammatory response. 1
The central role of TNFα in the inflammatory cycle of inflammation has proven to be an attractive target for IBD therapy. Other cytokines which present attractive targets for therapeutic agents include IFN γ, IL-12, and IL-23, as they play an important role earlier in the inflammatory cascade. The fact that variants in the IL-23 receptor gene have been associated with both UC and CD highlight the importance of IL-23 in IBD. 11
T-cell dysfunction
In addition to aberrant cytokine production, other T-cell defects likely contribute to IBD. Under normal conditions, a balance between effector and regulatory T-cells (Treg) allows immune surveillance without inappropriate inflammation. During periods of appropriate inflammation, depletion of antigen leads to T-cell apoptosis and promotion of a healing milieu. In IBD, T-cells demonstrate resistance to apoptosis and exhibit alterations in cell-cycle function. Furthermore, alterations in IL-10 and transforming growth factor (TGF)-β production and/or function fail to shift the balance away from inflammation and toward regulatory T-cell formation. 1
Biologic Therapy Targets Immune Mechanisms of IBD
Biologic agents (typically describing directed antibody based therapeutic agents) offer a unique method of targeting specific protein molecules in the body for either therapeutic or diagnostic aims. The specificity of monoclonal antibodies allows for very precise manipulations of various components of cellular growth, differentiation and expansion. The ability to disrupt these biologic processes has led to a tremendous expansion of research into how these agents can be used clinically to successfully intervene in a variety of disease processes. The first class of biologic therapy in Crohn's disease successfully targeted TNFα, which resulted in significant clinical success, given TNFα's multi-faceted role in inflammation. However, biologic therapy against this cytokine is not specific to the intestinal tract, which has resulted in some of the non-GI side effects noted with anti-TNF therapy. Ongoing basic and clinical research is now focusing on more specific targets of IBD, in hopes that non-selective side effects can be minimized or eliminated, while clinical efficacy improves. The following section will review both the benefits and short-comings of non-selective biological therapies, then focus on potential benefits from GI-selective biologic therapies.
Anti-TNFα agents
Therapeutic strategies targeting TNFα have proven effective in treating a number of autoimmune inflammatory diseases, including rheumatoid arthritis, psoriasis and psoriatic arthritis, and ankylosing spondylitis. As discussed above, this cytokine also appears to have a major role in the pathogenesis of IBD. 12 The United States Food and Drug Administration (FDA) has currently approved three anti-TNFα agents for the treatment of Crohn's disease.
Mechanism of action
TNFα is a pluripotent cytokine present in the body in both soluble and membrane-bound forms, and a number of different mechanisms of action have been proposed to account for the activity of anti-TNFα agents in IBD, including neutralization of soluble and membrane-bound TNFα, induction of antibody-dependent cell-mediated cytotoxicity, complement-mediated cytotoxicity and apoptosis, and inhibition of bacterial LPS-induced cytokine production. 12 Although infliximab and adalimumab both demonstrated evidence of antibody mediated effects, certolizumab was no better than placebo at inducing antibody-dependent cell-mediated cytotoxicity, complement-mediated cytotoxicity, and apoptosis, which suggests these mechanisms are not as important as originally hypothesized in CD. 12
Clinical efficacy in IBD
Most clinical trials of biologics have used clinical response as the primary endpoint measuring efficacy, but great variation exists in defining this indicator of benefit (Table 1). Remission is universally defined by a Crohn's Disease Activity Index (CDAI) score <150, which can individually be manifest by improvement of disease manifestations without complete cessation of clinical symptoms. In clinical practice, the ultimate treatment goal for treating CD patients should consist of inducing and then maintaining a corticosteroid-free remission. 16
Design of approved biologic induction trials.
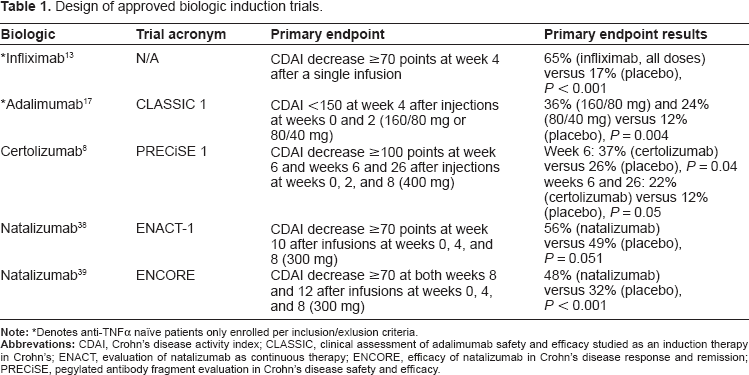
Denotes anti-TNFα naïve patients only enrolled per inclusion/exlusion criteria.
Clinical trials examining the induction efficacy (with or without a maintenance phase) of anti-TNFα therapy (infliximab-ACCENT 1; A Crohn's Disease Clinical Study Evaluating Infliximab in a New Long Term Treatment Regimen, adalimumab-CLASSIC 1; Clinical Assessment of Adalimumab Safety and Efficacy Studied as an Induction Therapy in Crohn's, and certolizumab-PRECiSE 1; Pegylated Antibody Fragment Evaluation in Crohn's Disease Safety and Efficacy) all demonstrated statistically significant superiority of the active treatment over placebo for their respective pre-specified primary end-points.8,13,17 Additionally, at indicated and/or optimal doses, all 3 agents demonstrated statistically superior remission rates at the week 4 time point compared with placebo (Fig. 3A).
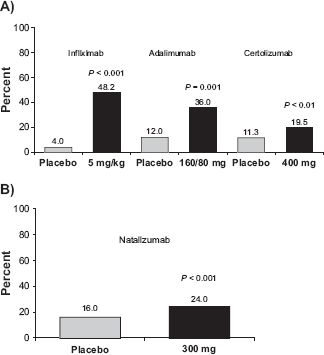
Week 4 remission rates with approved biologic therapies;
Infliximab, adalimumab, and certolizumab are all capable of maintaining remission in patients who respond to initial induction therapy (Table 2).6,7,18 Registration trial designs for each approved agent utilized different time points for measuring remission: certolizumab was measured at 26 weeks, compared with 54 and 56 weeks for infliximab and adalimumab respectively (Fig. 4A). To compare the results of the ACCENT 1, CHARM (Crohn's Trial of the Fully Human Antibody Adalimumab for Remission Maintenance), and PRECiSE 2 trials at similar time points (weeks 26 through 30), a recent review calculated an overall remission rate by multiplying the percentage of patients responding to induction therapy (at weeks 2 to 6) by the remission rates at weeks 26 to 30. 19 The results showed striking similarity in overall remission rates for the three TNFα inhibitors. Both infliximab and adalimumab demonstrated an overall remission rate of 23% (at weeks 30 and 26, respectively) and the overall rate with certolizumab was 31% at week 26.
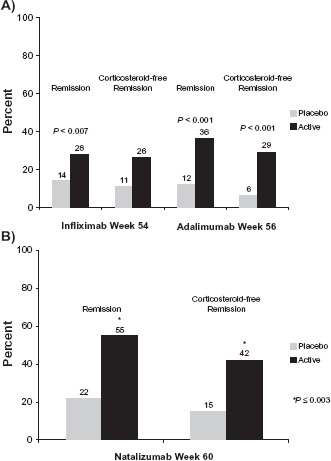
Long-term remission for approved biologic therapies;
Design of approved biologic maintenance trials.
Safety and efficacy concerns for anti-TNF therapy
The frequently heralded benefits of anti-TNFα treatment do not come without attendant risks. Antibody therapy against TNFα has been associated with serious infections, hematologic and skin malignancies, neurological symptoms, worsening heart failure, and liver function abnormalities. Furthermore, the development of native antibodies targeting the therapeutic antibodies can result in a loss of control of the underlying disease process, infusion reactions, injection site irritation, or immune complex related complications. Less than complete response rates have prompted efforts to optimize clinical efficacy, such as use of combination therapy or implementing escalating dosage levels.
Optimization techniques for maintaining remission and preventing therapy related immune reactions
Considerable controversy exists regarding the optimal treatment regimen when using biologic therapies, especially when considering the administration of concomitant immunomodulators. The practice of combining TNFα inhibitor therapy with immunosuppressants came about after analyzing the results of initial trials with infliximab. These trials suggested that the development of native antibodies against infliximab was reduced when given in combination with immunomodulators such as azathioprine, resulting in enhanced efficacy rates.20,21 More recently approved TNF inhibitors do not appear to be as immunogenic, and may be more reliably used without concomitant immunosuppressants.6,18 Recent reports even suggest that immunosuppressants can be safely withdrawn for CD patients receiving scheduled infliximab, especially when those patients are in a state of deep remission characterized by a CRP <5 mg/L and a normal platelet count.22,23 However, discussion regarding the need for immunomodulator therapy in combination with anti-TNF therapy has assumed center stage again after results of the Study of Biologic and Immunomodulator Naïve Patients in Crohn's Disease (SONIC) were recently published. 24 The primary endpoint, steroid-free clinical remission, was achieved by 30.6% of patients receiving azathioprine alone, 44.4% of patients on infliximab monotherapy (P = 0.009), compared to 56.8% of patients on combination therapy (P < 0.001). Patients with active inflammation, as indicated by elevated baseline levels of C-reactive protein and/or baseline colonoscopic evidence of ulcers, appeared to have the strongest benefit from combined therapy. A total of 44% of patients on combination therapy (P < 0.001) and 30% of patients on infliximab monotherapy (P = 0.0223) achieved mucosal healing compared to 17% of patients receiving azathioprine monotherapy. Safety profiles were comparable amongst all three treatment groups. The six month benefits persisted out to the final analysis at one year.
Consequences of anti-therapeutic antibody development Loss of response
The development of native antibodies to infliximab occurs more frequently in patients receiving episodic treatment than those receiving regularly scheduled maintenance therapy.21,25 Anti-infliximab antibodies have been associated with decreased clinical efficacy. 20
Hypersensitivity, infusion, and injection reactions
In clinical trials with infliximab, subjects receiving active therapy with infliximab were almost twice as likely to experience some form of infusion reaction within two hours of drug administration, compared to subjects receiving placebo. Much less frequently, a delayed serum sickness-like reaction can occur. This type of reaction occurs more often in patients restarting infliximab after 2 or more years out from a treatment hiatus. 26 Given the role of the skin as an organ of tolerance, it is not unexpected that hypersensitity reactions to adalimumab were rare. Approximately 1% of patients experienced allergic reactions, while an even lower rate of reactions were reported with certolizumab.27,28
Complications of TNFα inhibitors Infection
Given the fact that TNFα plays a pivotal role in the development of an innate immune response to pathogens, it stands to reason that treatment with anti-TNF antibodies carries an increased rate of infection when used in patients with chronic inflammatory conditions.9,29 While the use of corticosteroids, AZA/6MP or infliximab carries an increased risk of serious infections in patients with IBD (OR = 2.9) compared to no treatment; patients receiving a combination of prednisone plus another of these drugs had an odds ratio of 14.5. 30 Clinicians need to be aware of the specific risk of opportunisitic infections by fungal organisms, which has prompted the FDA to add an additional black box warning to the label of every inhibitor of TNFα.
Malignancy
The role of TNFα in tumor growth is unclear. Evidence from animal studies of anti-TNFα therapy in the azoxymethane/dextran sulfate sodium model suggests that anti-TNFα antibodies can reduce colonic tumor formation in the presence of chronic inflammation.31,32 However, clinical data suggest this form of therapy conveys an increased risk of malignancy. In a meta-analysis of adverse events associated with therapy in rheumatoid arthritis patients treated with infliximab and adalimumab demonstrated that the risk for malignancy with active treatment was three times higher than that of placebo treated patients. 29 In contrast, a similar meta-analysis of placebo controlled trials for CD did not find an excess of malignancies in treated patients. 33 Further data from large population databases containing TNFα exposed patients will be required to detect whether relatively infrequent malignant events actually occur at higher rates with therapy. One especially fearsome malignancy is that of hepatosplenic T-cell lymphoma (HSTL). HSTL is a rare non-Hodgkin's T-cell lymphoma that comprises only 5% of T-cell lymphomas. This malignancy most often occurs in immunocompromised patients, such as those infected with human immunodeficiency virus (HIV), but recent reports documenting HSTL in patients receiving anti-TNF therapy and concomitant immunomodulators for IBD have alarmed gastroenterologists. 34
Rationale for therapy beyond TNFα antibodies
While TNFα-antibody treatment provides a number of patients with benefit, approximately 30%–40% of patients with CD do not respond to induction therapy with anti-TNFα agents. Of those who initially respond, 50% or more lose their response within a year, clearly suggesting a need for additional approaches to the treatment of patients with IBD.6–8
Role for anti-integrin therapies
Continuous replacement of effector lymphocytes occurs by the recruitment and migration of circulating lymphocytes into inflamed mucosal tissue in IBD patients. This replenishment process is crucial to the sustained inflammation characteristic of chronic IBD. The process of enticing lymphocytes into an area of inflammation is contingent on interactions between lymphocyte cell surface proteins and their endothelial receptors. This complex process allows lymphocytes to come out of “solution” and begin the process of transendothelial migration into inflamed tissues. Because the interaction between integrins (specialized cell surface proteins expressed by T cells after activation by antigen presenting cells) and their receptors plays a key role in the inflammatory process in IBD, interfering with this interaction promises to be an attractive target for treatment. Functional integrins exist as a dimer composed of an α and a β subunit.
Integrin molecules participate in at least two events of the leukocyte adhesion cascade, involving arrest from rolling and initiation of the post-binding phase, when the tenuous leukocyte adhesion is stabilized. 15 Prior to interacting in this process, the integrin must first become activated. (Fig. 5) Integrin activation is a complex process controlled by an inside-out signal transduction event triggered by selectins, chemoattractants and TCR-bound Ag. 35 Agonist receptors lie scattered across the cell surface of a leukocyte, ready to interact with specific ligands such as mucins and selectins. The ligand/receptor interaction stimulates G-protein signaling events, which lead to diacylglycerol formation and intracellular calcium liberation. 36 As additional mediators gather, recruitment of Talin to the intracytoplasmic portion of the β-integrin subunit ensues, resulting in a conformational change of the integrin sub-units. 36 The conformational change opens the molecular structure of the integrin sub-units to allow ligand binding sites to become available. Following integrin activation, target ligand affinity is further enhanced by a simultaneous migration of the activated dimers through the cell membrane to form clusters. 35 This high affinity state allows the lymphocyte to transition from the rolling state to the arrest state. Once arrest has been achieved, the lymphocyte proceeds to transmigrate to the inflamed tissue by either paracellular or transcellular routes. 15 To date, antibodies targeted to α4, α4β7, and β7 integrins have undergone clinical trials for IBD.
Key events of leukocyte adhesion under control of α4, α4β7 integrins.*
Natalizumab
Structure and mechanism of action
Natalizumab is a humanized monoclonal antibody which possesses specificity for human α4 integrin. The antibody's complementary-determining regions (CDRs) bind to the α4-subunit of both α4β1 and α4β7 integrin heterodimers. The natalizumab-α4 integrin complex blocks the interaction of the cell surface proteins with their endothelial targets, including VCAM-1 and MAdCAM-1. 37
Clinical efficacy in CD
Two trials have examined the induction efficacy of a 300 mg monthly infusion of natalizumab (Table 1).38,39 Although a large proportion of subjects receiving natalizumab responded to therapy in the ENACT-1 (Evaluation of Natalizumab as Continuous Therapy) trial, a correspondingly high placebo rate likely caused the study to fail to demonstrate statistical significance over placebo for the primary endpoint. One suggestion for the exuberant placebo response relates to the study design. In order to accumulate sufficient subjects for long-term follow-up and to assist recruiting, a 4:1 drug to placebo randomization scheme was followed. It is well known that the method of calculating Crohn's disease activity index response and remission rates contain some subjective responses. The category of well-being may be influenced by a subject's perception of receiving therapy, or simply by being more intensely monitored by study personnel. However, subgroup analyses did demonstrate a greater separation of treatment response compared to placebo when considering subjects with an elevated baseline CRP levels (>2.87 mg/dL). In light of this finding, a second induction trial (ENCORE; Efficacy of Natalizumab in Crohn's Disease Response and Remission) only enrolled patients with elevated baseline CRP levels (>2.87 mg/dL). In addition, subjects were randomized in a 1:1 ratio to either active therapy or placebo. In the final analysis, the ENCORE study clearly demonstrated an induction benefit gained from natalizumab according to the primary endpoint of a clinical response at both weeks 8 and 12, rather than at a single time point. 39 In addition, the secondary endpoint consisting of remission at both weeks 8 and 12, was also significantly higher in the natalizumab group.
Responders from the ENACT-1 trial (patients achieving a clinical response at weeks 10 and 12), who chose to continue in the ENACT-2 maintenance trial, were randomized to receive either continued therapy with natalizumab or placebo every 4 weeks. 38 The remission rate at week 60 in the natalizumab group was 55% compared with 22% in the placebo group (P < 0.05) (Fig. 4B). Of those subjects who were still in remission at month 12, a total of 87 patients enrolled into ENABLE (Evaluation of the Natalizumab Antibody for Long-term Efficacy) study. At the end of an additional 12 months, 75 out of the 87 subjects (86%) entering ENABLE maintained remission (in submission).
Corticosteroid sparing effects
Forty-two percent of the natalizumab responders in ENACT-1 were receiving oral corticosteroids or budesonide at entry. Among responders re-randomized to placebo, 28% had eliminated corticosteroids at week 36, compared with 58% of responders who had been re-randomized to natalizumab (P < 0.001). At week 36, 45% of natalizumab-treated patients who took corticosteroids at entry had discontinued them and were in remission, compared with 22% of patients in the placebo group (P = 0.01). This benefit was maintained throughout the trial and, at week 60, 42% of natalizumab-treated patients entering on baseline corticosteroids had discontinued them and were in remission, compared with 15% of patients in the placebo group (P = 0.001). 38 Eighty of the subjects from ENACT-2 were in corticosteroid-free remission at entry into ENABLE, with 65 of the 80 (85%) finishing an additional year steroid free (in submission).
Concomitant immunosuppresants
Approximately 1/3 (300/905) of subjects entering ENACT-1 took concomitant medications. 38 Although not a primary or secondary objective, in a post-hoc analysis, subjects with combination therapy responded better to natalizumab than those on mono-therapy (62% vs 54%). However, this finding was not borne out in the ENCORE study, as patients receiving monotherapy with natalizumab responded better than those receiving concomitant immunodmodulators. 40 This information is useful, as current prescribing restrictions per the TOUCH program limit the administration of natalizumab as a monotherapy, precluding the use of concomitant immunomodulators. 40
Efficacy in the setting of TNFα antibody exposure
Both induction trials with natalizumab (ENACT-1, ENCORE) contained a large number of patients who had previously undergone treatment with a TNFα inhibitor. In fact, many were considered TNFα failures. Of the 48% of patients in the ENCORE trial who had prior exposure to a TNFα inhibitor, most (71%) were considered to have failed this therapy. 41 In a post-hoc analysis of the efficacy of natalizumab in ENCORE subjects who were also TNFα failures, 38% of patients had a sustained response to natalizumab through weeks 8 and 12, compared with only 15% of patients treated with placebo (P < 0.001). Approximately 50% of the natalizumab-treated patients who had failed prior treatment with anti-TNFα therapy responded to treatment at either time point (52% at week 8 and 49% at week 12), which compared favorably with the placebo group (22% at week 8 and 29% at week 12) (P ≤ 0.006). Remission was sustained through weeks 8 and 12 in 17% of patients treated with natalizumab compared with only 5% of patients in the placebo group (P = 0.012). 41
In ENACT-2, 58% of patients treated with natalizumab and who also had a history of TNF inhibitor exposure achieved a sustained response at every time point through month 9 compared with 10% treated with placebo (P < 0.001). Similarly, sustained remission was observed in 39% of patients treated with natalizumab versus 8% of those treated with placebo (P = 0.002). Statistically significant treatment differences in the maintenance of sustained clinical response and remission between natalizumab and placebo were observed until the end of the study at month 15 (in submission). In ENACT-2 subjects who had failed TNF inhibitor therapy, sustained response at every time point through month 9 was observed in 53% of natalizumab recipients compared to 13% of placebo recipients (P = 0.001). These differences remained statistically significant through the end of the study at month 15. Remission was achieved by 29% of natalizumab-treated patients and 8% of placebo-treated patients (in submission). Corticosteroid withdrawal in patients previously exposed to a TNFα inhibitor was possible in 46% of natalizumab-treated patients compared with 18% of placebo-treated patients (P = 0.044) (in submission). This information, demonstrating benefit after TNF-α antibody failure/non-responders, is helpful to clinicians and potential patients to recognize how natalizumab performs within the prescribing requirements per the TOUCH program. This limited prescribing program requires that patients treated with natalizumab must have failed standard therapies, including anti-TNF regimens.
Clinical limitations and safety
Common side effects
In all controlled clinical trials of natalizumab, the most common adverse reactions (with an incidence ≥10%) were headache and fatigue. 37 The most frequently reported adverse reactions resulting in discontinuation of natalizumab in CD trials involved the exacerbation of CD (4%) and acute hypersensitivity reactions (2%). 37
Immunogenicity
Immunogenicity has occurred at consistently low rates in controlled studies of natalizumab. Fewer than 10% of patients developed anti-natalizumab antibodies in the ENACT-1 and ENCORE trials, with persistent antibody formation (defined as 2 positive antibody tests occurring at least 6 weeks apart or a single positive test at the last measurement) occurring in only 6% of patients in the ENACT-2 maintenance trial. 38 The occurrence of persistent antibodies against natalizumab was associated with a loss of clinical efficacy in the ENACT-2 trial; however, 75% of patients with transient antibody formation continued to maintain a response through week 60. 38
Hypersensitivity
Anti-natalizumab antibody formation appears to affect the rate of acute infusion reactions, as 45% of ENACT-1 subjects who experienced acute infusion reactions tested positive for anti-natalizumab antibodies (24 of the 53 patients), compared with 53 of the 597 patients (9%) who tested negative for such antibodies (P < 0.001). Of the five patients who had serious hypersensitivity reactions, three tested positive for anti-natalizumab antibodies. In ENACT-2, anti-natalizumab antibody positive subjects had higher rates of acute infusion or hypersensitivity reactions compared to anti-natalizumab antibody negative subjects. 38 A post-marketing report of 40 patients with relapsing-remitting multiple sclerosis published a 10% incidence (4 out of 40 subjects) of type III allergic reaction in patients treated with chronic natalizumab. 42 Clinical symptoms of type III reaction included fever, headache, arthralgias, edema, and peripheral lymphadenopathy which progressed over several days after infusion. Two patients developed documented antibody response against natalizumab. 42 Co-administration with corticosteroids improved symptoms with subsequent infusions, but some patients required discontinuation.
Acute infusion reactions typically manifest with one or more of the following symptoms: flushing, shortness of breath or chest tightness, dizziness, headache, changes in blood pressure, diaphoresis, fever, or nausea/vomiting. 43 Intervention for an acute infusion reaction consists of stopping or slowing the infusion rate, substituting intravenous fluids for resuscitation to maintain blood pressure, frequent monitoring of vital signs, and administration of an antihistamine and/ or acetaminophen. Severe decompensation of vital signs or airway compromise should be treated with prompt subcutaneous administration of 1 mL epinephrine 1:1,000. Infusion reactions occurring within the first 24 hours are considered acute reactions, with most occurring within 2 hours of drug administration. 43 Delayed infusion reactions may occur from one to fourteen days after drug infusion. 43 Delayed type infusions may be mild, moderate or severe, and may require one or more of the following: anti-histamines, acetaminophen or even corticosteroids for severe or refractory cases.
Malignancies
From registration trials of natalizumab for the treatment of CD, seven malignancies were reported in 1182 patients: breast cancer (n = 2), colon cancer (n = 1), bladder cancer (n = 1), lung adenocarcinoma (n = 2), and malignant melanoma (n = 1). One subject, who received only placebo, developed uterine cancer. The composite rate of malignancies in natalizumab-treated CD patients was 1.6 events/100 patient years, compared with 0.60 events/100 patient years in the placebo group. 44 A recent report on melanomas in patients treated outside of clinical trials described the development of melanomas in close temporal relationship with the onset of therapy with natalizumab. 45 Both patients had previously known nevi which underwent a change soon after initiating therapy with natalizumab.
Infections
Of 1182 subjects participating in CD clinical trials, 40% experienced at least one infection compared to 36% of placebo-treated patients. Relatively few infections resulted in permanent discontinuation. Discontinuation rates were similar between natalizumab (0.6%) and placebo-treated (1%) patients. Serious infections also occurred at comparable rates (natalizumab = 2.5%, placebo = 2.6%). 44 Five serious opportunistic infections occurred in CD subjects receiving one or more natalizumab infusions (n = 1598), equating to an incidence of 0.3% (95% confidence interval [CI] = 0.10–0.73) and a rate of 0.0029 (95% CI = 0.001–0.007) per person-year. 44 Opportunistic infections involved organisms such as Cytomegalovirus, Aspergillus, Pneumocystis carinii, M. avium and JC polyomavirus. 44 Reactivation of the JC polyomavirus (JCV) which lies dormant in approximately 85% of healthy individuals, can lead to a rare demyelinating disorder of the central nervous system named progressive multifocal leukoencephalopathy (PML). 46 One theory linking drug exposure to PML suggests that natalizumab interferes with CNS immune surveillance by JC polyomavirus specific effector T cells. In fact, the ratio of CD4:CD8 T cells in the cerebrospinal fluid (CSF) of patients treated with natalizumab dropped to levels seen in patients with human immunodeficiency virus (HIV), which was not reflected in the peripheral blood T cell pool. 47 An imbalance of the immune cell components in the CNS may not be the only explanation. Primary infection with JCV does not generally cause a clinically significant infection. However, natalizumabmediated effects on B lymphocyte differentiation may influence JCV-infected bone marrow cells to produce rearrangements during JCV reactivation, releaseing a more potent variant capable of inducing the clinical syndrome recognized as PML. 48 The number of cases of PML has steadily increased as more patients initiate therapy with natalizumab. Exposures to natalizumab longer than one year impart a greater risk of infection. Based on more than 30 confirmed cases of PML in patients exposed to natalizumab, the Food and Drug Administration (FDA) confirmed that a 1 in 1000 risk of developing PML calculated from clinical trials data appears to be accurate, but warned that the risk might increase when treatment continues beyond 24 months. 49 A lack of pathognomonic symptoms of early PML precludes easy detection of the onset of PML, but symptoms of visual changes, mental status changes, or motor dysfunction should prompt a thorough evaluation. Laboratory evaluation for virus shedding in the urine or blood has not been helpful in predicting PML infection. 48 CNS evaluation with magnetic resonance imaging (MRI) is most helpful in suggesting a diagnosis of PML, which frequently demonstrates hyperintense, multifocal white matter lesions on T2 imaging. 48 Confirmation should be accomplished via polymerase chain reaction testing (PCR) for elements of the JC virus. Current strategies for dealing with PML include immediate cessation of natalizumab, rapid elimination of the drug through multiple plasma exhanges, and treatment of immune reconstitution inflammatory syndrome (IRIS), if present. The administration of mefloquine hydrochloride has been suggested as a mechanism for impairing JCV replication. 50
Hepatotoxicity
Although no evidence of liver injury surfaced in clinical trials, clinically significant liver injury has occurred in patients receiving natalizumab in the post-marketing period. Re-injury has been noted upon repeat exposure to natalizumab, strengthening the link between natalizumab and the injury. 37
Pregnancy
The demographics of Crohn's disease coincide with the prime childbearing years for women, leading to a need for information on the interactions of disease specific medications and a developing fetus. Although natalizumab is currently classified as category C by the FDA, a global registry has been formed to follow the outcomes of pregnancies exposed to natalizumab. A recent snapshot from the registry determined that out of 125 known outcomes from 179 total pregnancies enrolled, there were 99 live births with eight malformations. 51 The number of spontaneous abortions in the prospectively enrolled pregnancies (11%) conformed to the expected rate in the US population. None of the malformations were judged related to natalizumab exposure.
Vedolizumab
Structure and mechanism of action
Vedolizumab (MLN0002) is a humanized monoclonal antibody, which differs from natalizumab in that it specifically recognizes the heterodimer α4β7 integrin without interacting with the individual component monomers. 52 The most important receptor for this integrin, MAdCAM-1, is expressly up-regulated on the vascular endothelium of inflamed intestinal tissue. 52 The ability of vedolizumab to specifically interfere with trafficking to inflamed intestinal mucosa makes this molecule extremely attractive for the treatment of IBD.
Clinical efficacy in Crohn's disease
Several early phase studies have demonstrated a potential benefit for vedolizumab for treating Crohn's disease. In a small pilot study, vedolizumab was significantly more effective than placebo at inducing clinical remission (P = 0.03) and endoscopic remission (P = 0.007) at week 6. 52 The therapy was well- tolerated, but human anti-human antibodies developed by the week 8 time point in 44% of subjects receiving active treatment. Subjects who were positive for antibodies at a titer of > 1:125 had lower saturation of α4β7 binding sites and responded similarly to the placebo group.
In a larger phase II trial studying patients with moderate to severe CD, vedolizumab was again well tolerated and resulted in a substantial benefit. 53 One hundred eighty-five subjects with moderate to severe Crohn's disease were enrolled and randomized to receive two infusions of either MLN0002 2.0 mg/kg, 0.5 mg/kg, or placebo. The primary endpoint, determined on day 57 by a ≥70 point drop from the baseline CDAI score, was achieved by 53%, 49% and 41% of subjects respectively in a somewhat dose dependent fashion (P = 0.14 and P = 0.36 for the highest and lowest dose, respectively). Although the trial failed to meet the primary endpoint, the highest dose did achieve statistical significance for the more difficult to achieve endpoint of clinical remission on days 15, 29 and 57 (P = 0.009, 0.47 and 0.49, respectively). Vedolizumab is currently being evaluated in large phase III clinical trial for patients with moderate to severe Crohn's disease and ulcerative colitis.
Clinical limitations and safety
Common Side Effects
The most common adverse event occurring, at > 10% for both active therapy and placebo, was headache. 53 Other common adverse events included nausea, fatigue, nasopharyngitis, and abdominal pain.
Serious adverse events
A similar number of adverse events and serious adverse events were seen in both groups. Sixteen subjects (13%) treated with MLN0002 experienced at least one serious adverse event (SAE), compared to 10 (17%) subjects receiving placebo. Exacerbation of Crohn's disease was the most common SAE. 53 Other serious events occurring in more than one patient include small bowel obstruction and kidney stones. Escalating doses did not correlate with increasing side effects. One serious infection occurred in an actively treated subject, while two occurred in subjects receiving placebo. Lastly, no cases of PML, colon cancers, lymphomas or deaths were seen in any subject.
Immunogenicity
Antibody formation to MNL0002 was noted in 21 (34%) of subjects receiving the lowest dose active therapy, while 8 (12%) of subjects receiving 2.0 mg/kg MLN0002 developed anti-therapeutic antibody titers. 53 Higher titers of human-anti-human antibodies (HAHA) tended to correlate with reduced clinical efficacy and possibly one clinically significant infusion classified as an SAE.
Conclusion
Current guidelines recommend a step-wise approach to the treatment of IBD, involving the addition of more powerful therapies as severity and refractoriness to therapy increases. Therefore, biologic therapies are typically used after corticosteroids and immunosuppressants have failed to achieve or maintain prolonged remission. 19 Anti-TNFα agents represent a major therapeutic advance for patients with moderate-to-severe CD. Patients who enter remission after induction therapy with any of the anti-TNF-α agents should continue on that therapy as long as a steroid free remission is maintained. While TNFα inhibitors continue to be an effective therapeutic strategy for patients who are refractory to corticosteroids and immunosuppressants, a growing number of patients have either failed to initially respond to this class of biologics, or lose response over time due to immunogenicity or other factors. Approximately 30% of patients with CD who are refractory to standard treatment do not respond and, of those who initially respond, 50% or more cease to respond within a year. A smaller percentage of CD patients have some contraindication to TNFα inhibitors, and cannot initiate therapy with this class of medication. This clearly indicates a need for novel approaches to the treatment of patients with IBD.
IBD is driven by lymphocytes that traffic from the circulation into the gut tissue. Such trafficking is mediated by a series of adhesive interactions between the invading lymphocyte and endothelial cells. Consequently, anti-adhesion molecule strategies represent an attractive concept for the development of novel therapeutics in the management of IBD. Natalizumab, a humanized monoclonal antibody against human α4 integrin, is approved for the treatment of patients with moderately-to-severely active CD. This agent represents an efficacious therapeutic option for patients who do not respond to, or have failed, a TNFα inhibitor. Development of additional biologic therapies, focusing on integrin targets or other cell recruitment mechanisms offer a great opportunity to target the anti-inflammatory therapy directly at the underlying mechanisms responsible for IBD. More effective and well tolerated therapies offer the chance of enhancing efficacy to capture an even greater percentage of patients symptomatic from these diseases, and create the potential to alter the natural course of the disease.
Natalizumab is currently the only clinically available anti-integrin therapy for Crohn's disease. Although this agent has proven efficacy for the treatment of anti-TNF refractory Crohn's disease, utilization rates will likely remain low over time, unless methods for stratifying the risk for PML or detecting re-emerging JCV before onset of clinical symptoms are developed. If potential patients could be reassured regarding lower to no risk of PML, natalizumab would become a much more palatable choice. If vedolizumab clinical trials demonstrate nearly equal efficacy rates in the setting of a durable therapy, and no new safety concerns materialize, this form of gut selective anti-integrin therapy will likely supplant the use of natalizumab for Crohn's disease.
Disclosures
This paper is unique and not under consideration by any other publication and has not been published elsewhere. The author reports that he has served as an investigator and consultant for Elan, speaker for Abbott and and investigator for Centocor in the past year. The author confirms that he has permission to reproduce any copyrighted material.