
Abstract
Smoking remains a major public health challenge. Nicotine is the main psychoactive drug responsible for the addictive nature of tobacco, explaining why many smokers fail to quit without assistance. Pharmacotherapy for smoking cessation is deemed effective for a broad range of populations and should be routinely offered to smokers interested in making a quit attempt. Varenicline, a partial agonist at the α4β2 nicotinic receptor increases chances of quitting three-fold compared to placebo in smokers without comorbidities, and in smokers with cardiovascular disease or chronic obstructive pulmonary disease. Persons with mental illness have high rates of smoking, and the potential impact of varenicline on mental status and the underlying pathophysiology of mental illness, has become a salient concern. Varenicline is an appropriate aid for smoking cessation in patients with medical and/or psychiatric comorbidity. This conclusion is supported by current evidence on the safety and tolerability of the drug.
Introduction
One hundred million people were killed by the tobacco epidemic in the 20th century alone. The World Health Organization (WHO) estimated a possible death toll of one billion humans in the 21st century, and reversing this entirely preventable epidemic is a top public health priority. 1 Despite a declining prevalence of smoking rates in some countries, the global numbers of smokers are still on the increase, and tobacco remains the leading preventable cause of death and disease worldwide. Over one-fifth of the U.S. population are daily consumers of cigarettes and 18% of mortality is attributed to tobacco-related causes. 2 Over two-thirds of smokers are interested in quitting, and about 50% will make at least one cessation attempt every year. Without treatment, however, only 4%–7% will achieve lasting abstinence from tobacco. 3
In 1988 the U.S. Surgeon General concluded that nicotine in tobacco is the primary element leading to tobacco addiction. 4 When smoked, tobacco is one of the most highly addictive of all chemical substances commonly abused. 5 Nicotine is a full agonist at the nicotinic acetylcholine receptors, mediating the dependence producing properties. 6 The 2008 report from the Surgeon General has suggested that tobacco dependence treatments are effective across a broad range of populations and recommended that pharmacotherapy be offered to all adult non-pregnant cigarette smokers, willing to make a quit attempt. 7
Three approved classes of medication are widely available as first line options for treatment of tobacco dependence. These include nicotine replacement therapy (NRT), bupropion and varenicline. Bupropion is an antidepressant that enhances synaptic dopaminergic and noradrenergic tone. It also appears to act as a weak antagonist at nicotinic acetylcholine receptors. 8 Among different subtypes of nicotinic acetylcholine receptors, the α4β2 receptor, where nicotine is a full agonist, has been shown to compose the critical link in the neurotransmitter chain that maintains tobacco addiction. 10 Following this discovery, the design and development of a partial agonist at this particular receptor was pursued. Subsequent proof of concept studies showed that a partial agonist would relieve craving and withdrawal by mimicking agonist effects of nicotine, as well as possess antagonistic properties by blocking nicotine from binding the receptor. 11
Initial efforts focused on an alkaloid extract from the golden rain tree Cytisus laburnum, i.e. the compound cytisine. This compound is a partial agonist at the α4β2 nicotinic receptor, and leaves from this tree were used in the World War II as a substitute for tobacco consumption. 11 In some Eastern European countries cytisine has been commercially available for decades, despite a general lack of empirical evidence in support of its efficacy. 11 The most likely explanation is cytisine's limited bioavailability and inadequate penetration of the brain following oral ingestion. 12 Further research and development produced novel partial agonists and ultimately led to the synthesis and marketing of varenicline.
Smokers with a range of medical illnesses have high relative and absolute risk of recurrent disease and premature death that is attributable to smoking. These patients have usually received repeated advice to quit smoking, and those who continue to smoke, may be highly addicted to tobacco and likely to relapse after a quit attempt. 13 Another important group for smoking cessation treatment are patients with mental illness. Persons with mental illness are more likely to smoke, less likely to quit, and consume almost half of all cigarettes smoked in North America. 14 Like other smokers, mentally ill persons who smoke are also at high risk of death and disease due to tobacco-related illnesses.15–20 With the high tobacco consumption rates in the mentally ill the potential impact of varenicline on mental status and the underlying neural basis of mental illness, has become a salient area of interest. Due to the involvement of cholinergic systems in the pathophysiology of both depressive and cognitive symptomatology and disorders, there has been speculation regarding the potential impact of varenicline on mental status, specifically mood symptoms and cognition in those using varenicline. This manuscript reviews the role of varenicline for smoking cessation in patients with medical and/or psychiatric comorbidity and discusses current data on the safety and tolerability of the drug.
Mechanism of Action, Pharmacokinetic Profile and Course of Treatment
Varenicline acts as a partial agonist, with high affinity, at the α4β2 nicotinic acetylcholine receptor. 9 Varenicline's high affinity leads to augmented dopaminergic tonus in the mesolimbic system, but only a 35%–60% maximal downstream increase of dopamine in response to varenicline. 21 This response ameliorates nicotine craving and withdrawal, caused by a nicotine deficit when an individual is quitting smoking, and reduces the rewarding effects of nicotine.
Varenicline is well absorbed and undergoes minimal metabolism after oral ingestion. 22 Almost the entire dose is excreted in the urine, of which 81% is unchanged. It is not affected by food intake and not significantly bound to protein. Drug-drug interactions are minimal due to the extensive renal clearance of the drug, bypassing the cytochrome P450 metabolic pathways in the liver and there are no contraindications. Peak plasma levels are reached 3–4 hours after administration of 1 mg twice daily. Varenicline has a long half life of 17–31 hours and unbound plasma concentrations are approximately 30–50 nM at steady state. The recommended dose is 0.5 mg once a day for three days, followed by 0.5 mg twice a day for the next four days and then 1 mg twice a day for 11 weeks, for a total of 12 weeks of treatment.
Clinical studies
General population
The safety and efficacy of varenicline for smokers volunteering to clinical studies is well-established.23–32 At 1 mg twice-daily varenicline increases carbon-monoxide validated odds ratios for quitting three-fold compared to placebo. 23 The target quit date is generally planned for the eighth day of treatment, also the first day on which the full dose is administered. Smokers are allowed to continue to smoke while taking varenicline during the first week of treatment and as treatment progresses more smokers make quit attempts in weeks subsequent to the first week.25–31 A further 12 weeks of treatment is recommended for patients who succeed in quitting during the initial treatment period, and treatment is individualized based on the characteristics of each specific case. Extended treatment to 24 weeks results in increased likelihood of long-term cessation, 33 particularly in smokers who did not manage complete abstinence from tobacco after their target quit date. 34
The initial studies that examined the efficacy of varenicline were performed in generally healthy smokers.24–33 As is usual in studies of a new drug, adolescents, the elderly, and pregnant or lactating subjects were excluded, as were women that could conceive. In addition, people with a spectrum of medical or psychiatric disease, substance abuse or eating disorders did not participate (Table 1). As noted in Table 1, the range of quit rates in non-Asian populations in these studies was about 44%–49% at the end of a 12-week treatment course, and approximately halved to about 22% after 1 year, which was 40 weeks after the end of treatment.24–27,30 After 12 weeks, the odds of cessation with varenicline versus placebo ranged from 4–8, and after 52 weeks, the odds were still about threefold in favor of varenicline. In Asian populations, quit rates were higher both with varenicline and placebo, and odds ratios somewhat lower.28,29,31 Relative risks in varenicline-treated subjects followed for at least six months are not significantly different from those at the end of treatment indicating that smokers do not relapse faster than placebo-treated subjects despite higher quit rates. 35
Studies of varenicline 1 mg twice daily versus placebo in smokers without significant medical conditions. Exclusion criteria, quit rates with varenicline treatment, odds ratios (ORs) versus placebo and 95% confidence intervals (CIs) are shown. NA = Not available.
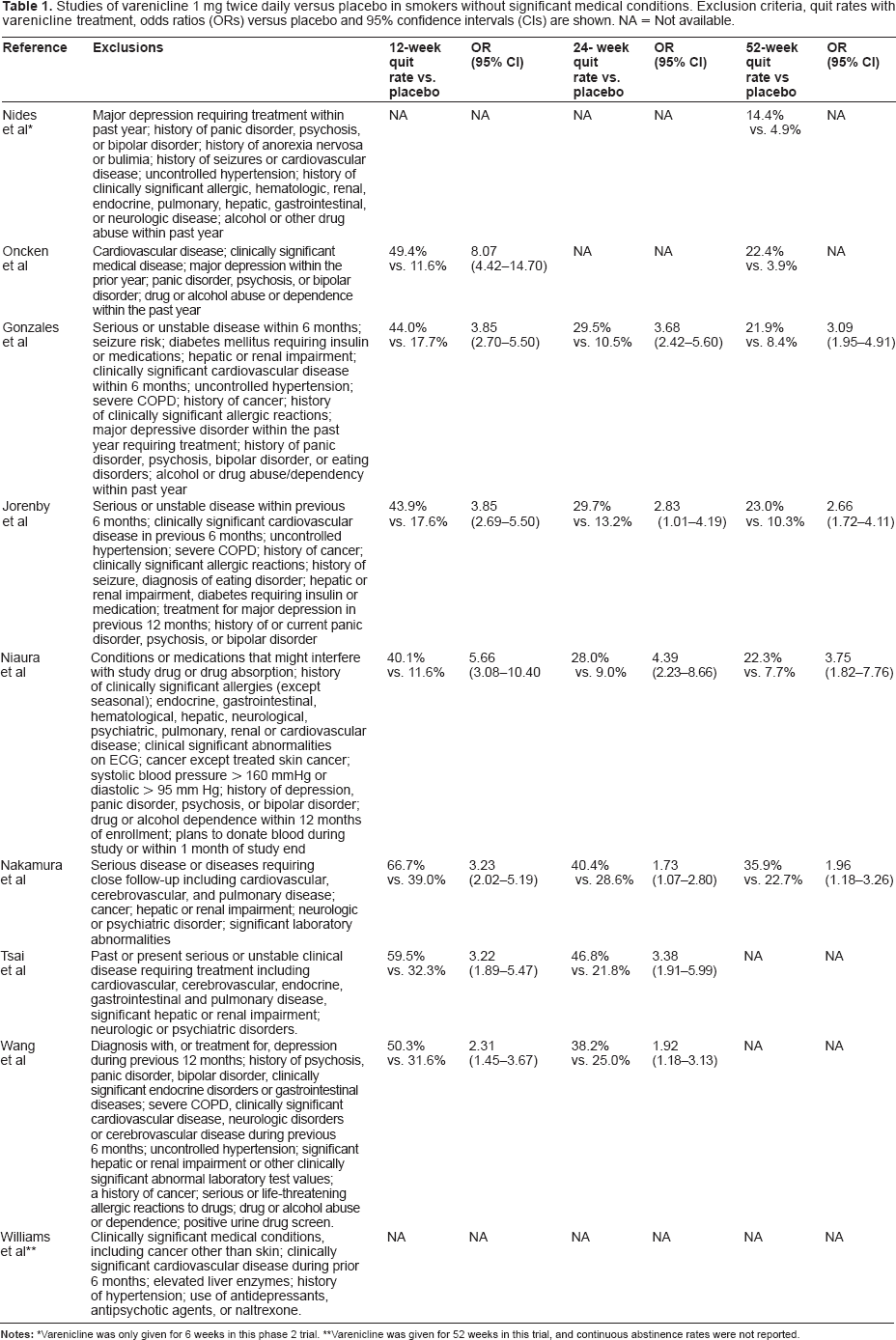
Varenicline was only given for 6 weeks in this phase 2 trial.
Varenicline was given for 52 weeks in this trial, and continuous abstinence rates were not reported.
Several meta-analytic studies have estimated the odds of cessation with varenicline versus placebo across published trials in smokers without comorbidities. In the Cochrane meta-analysis, varenicline increased the odds of successful long-term cessation approximately threefold. 23 Varenicline was found to be more efficacious than bupropion,23,36 and likely, more efficacious than NRT at least in the short term.37,38 While no randomized double-dummy clinical trial of varenicline versus NRT has been published, an open-label head-to-head study of varenicline compared to nicotine patch found increased efficacy of varenicline compared to nicotine patch at the end of treatment, though not after 52 weeks in participants who took at least 1 dose of the study drug. 39 The analysis based on the intention to treat population found an odds ratio of 1.44 (95% confidence interval [CI] 1.02–2.03) after 52 weeks in favour of varenicline.
Medical Comorbidity
Recently, studies have investigated the efficacy of varenicline in populations with conditions strongly associated with smoking, including smokers with cardiovascular and chronic pulmonary disease. These studies provide insight into the effect of varenicline in patient groups that are likely to attain major health benefits from cessation. While smokers suffering of medical diseases or conditions, related to smoking and otherwise, would be expected to respond similarly to medication as smokers who have not yet developed comorbidities, these are the very populations that may be particularly in need of highly efficacious medication.
Cardiovascular disease (CVD)
Cigarette smoking promotes atherosclerosis and is associated with an increased risk of myocardial infarction, sudden death, peripheral vascular disease and stroke. 40 Patients with coronary artery disease who stop smoking dramatically reduce their risk of recurrent events or death to the level of non-smokers within 5–10 years. The smoking-related excess risk is reduced by one-half within 1 year of quitting. About 50% of smokers admitted to a coronary care unit with an acute coronary syndrome stop smoking for extended periods of time but about one-half of this number relapse.
A recent systematic review and meta-analysis looked at trials of smoking cessation in patients with established cardiac disease. 41 Four randomized controlled trials (RCTs) using pharmacotherapies and 11 trials using behavioral treatments were identified. Among pharmacotherapies, one placebo-controlled study of transdermal NRT and one placebo-controlled study of nicotine gum,42,43 and two studies of bupropion were identified.44,45 Despite initial efficacy of NRT, at 6 months differences between subjects treated with NRT or placebo were not statistically significant. This was in contrast to the efficacy of NRT demonstrated in many studies in non-cardiac populations. This difference could be due to the limited number of studies in patients with cardiac disease, and the higher prevalence of depression and greater nicotine dependence in this population. Bupropion was efficacious in stable outpatients with a range of CVDs, 44 but in patients presenting early after an acute unstable coronary event efficacy of bupropion was not shown. 45 Thus, to date very limited data has supported pharmacotherapy for smoking cessation in patients with CVD.
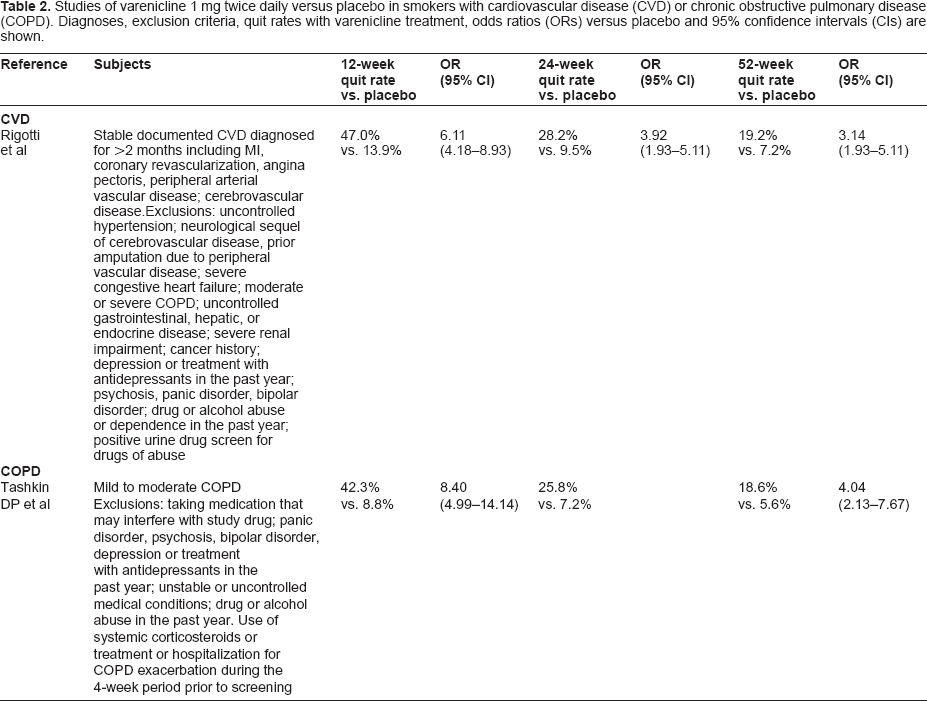
The first trial of varenicline in patients with CVD was a multinational study with 703 participants aged 35–75 years who were randomized to varenicline (1 mg twice-daily) or placebo for 12 weeks (Table 2). 46 Both groups were given behavioral support. At 12 weeks, carbon-monoxide confirmed continuous abstinence was 47.0% for varenicline versus 13.9% for placebo giving an odds ratio of 6.11 (95% CI 4.18–8.93). At 52 weeks, continuous abstinence was 19.8% for varenicline versus 7.4% for placebo resulting in an odds ratio of 3.2 (95% CI 1.97–5.18). The efficacy of varenicline in terms of odds ratios at the end of treatment seems greater than observed in so-called healthy smokers, and the results indicate that very few of these patients achieve abstinence with behavioral support alone (and placebo). As varenicline acts primarily at nicotinic receptors which differ from the α3β4 nicotinic receptors that raise blood pressure and heart rate, it was not expected to affect these hemodynamic parameters. 46 This was confirmed in this trial as the varenicline and placebo groups did not differ in blood pressure or resting pulse change from baseline to the end of treatment. Serious adverse events were observed in 6.5% of varenicline-treated versus 6.0% of placebo-treated subjects. Though it may be expected that cessation would reduce the number of cardiovascular events, this study was not designed to show such a difference, and the period of follow-up was too short for morbidity-related endpoints. With this study, clear evidence supports use of varenicline in stable patients with CVD.
Studies of varenicline 1 mg twice daily versus placebo in smokers with cardiovascular disease (CVD) or chronic obstructive pulmonary disease (COPD). Diagnoses, exclusion criteria, quit rates with varenicline treatment, odds ratios (ORs) versus placebo and 95% confidence intervals (CIs) are shown.
Pulmonary disease
Smoking cessation is the most effective way to reduce the risk of developing chronic obstructive pulmonary disease (COPD). Studies find that smoking cessation leads to a rapid return in the age-related decline in forced expiratory volume to the level seen in individuals who have never smoked. However, few studies have investigated smoking cessation therapies in patients with COPD.
In a systematic review that identified studies published up to 2002, only two studies using pharmacotherapy were identified. 47 In the Lung Health Study the effect of an intensive smoking cessation intervention including an intensive behavioral intervention combined with free nicotine gum was compared to usual care in patients with mild airway obstruction. The program was more effective than usual care after 12 months and throughout the 5-year follow-up period. In smokers with clinically identified COPD, bupropion treatment increased the odds of cessation after 26 weeks compared with placebo, but after 12 months, the difference between the groups was minor and no longer statistically significant. 48
Since 2002, additional studies have appeared and have been reviewed recently. 48 Treatment with bupropion resulted in higher abstinence rates compared with placebo in smokers with COPD or at risk for COPD at 26 weeks (difference versus placebo, 13.1% [95% CI 1.2%–25.1%] but not beyond. 49 The effectiveness of bupropion has not been demonstrated beyond 26 weeks in patients with COPD.47,48 In contrast, sublingual NRT was more effective than placebo after 12 months with a quit rate of 17% versus 10% (odds ratio ~2) in a trial conducted in 370 patients with COPD. 50
A recent study reported the effects of varenicline on quit rates after 1 year of follow-up (Table 2). 51 This was a multinational, double-blind placebo controlled trial where participants with mild to moderate disease, but who did not use systemic corticosteroids and had not been treated or hospitalized for COPD exacerbation during the 4-week period prior to screening, were included. Not surprisingly, these subjects appeared more dependent than smokers included in earlier trials of varenicline,26,27 with a more severe smoking history and a higher Fagerström dependence score. Carbon-monoxide confirmed abstinence from smoking was significantly higher for varenicline versus placebo during the treatment phase (weeks 9–12; 42.3% for varenicline versus 8.8% for placebo; odds ratio 8.40 [95% CI 4.99,14.14]). The efficacy of varenicline was maintained during the follow-up phase (weeks 9–52; 18.6% for varenicline versus 5.6% for placebo; odds ratio 4.04 [95% CI 2.13,7.67]). The expected adverse events occurred in the varenicline group, including nausea, abnormal dreams, insomnia and headache, which are similar to those reported in earlier trials. Serious adverse events were rare and did not occur more often with varenicline (2.8%) than placebo (4.8%). This study clearly established that varenicline is at least as efficacious or more efficacious given the higher odds ratio in smokers with COPD (though serious cases were excluded) as in smokers enrolled in previous trials who had no clinically significant medical conditions, similar to what was seen in the trial in patients with CVD.
Other evidence on the efficacy of varenicline in patients with COPD is scarce. Patients with mild to moderate COPD were eligible for a 1-year study of continuous varenicline treatment, 32 but the percentage of subjects with COPD in the trial was not reported. Trials listed in Table 1 may also have included some patients with mild or moderate COPD, but again, the proportion of these patients has not been reported.
Other comorbidities
Patients with diabetes were excluded from a number of studies if they required insulin or oral medications and probably from the other studies that excluded participants with endocrine or significant medical disease (Table 1),26,27 but comprised about 15% of participants in the CVD trial. 46 Results have not been reported separately for this group. Case reports have appeared of hypoglycaemia in patients with type 1 diabetes treated with varenicline. 52 Whether this is a result of increased insulin sensitivity following smoking cessation remains to be determined. Varenicline does not appear to ameliorate post-cessation weight gain. 53
Patients with cancer other than skin cancer were excluded from the trials (Table 1) and no data is available on varenicline in this patient group. In a group of 19 patients with HIV treated with antiretroviral therapy, 1 subject stopped treatment because of adverse event; in the remaining subjects, treatment was tolerated with no unexpected adverse effects. 54
Considerations in patients with renal or hepatic disease
More than 80% of varenicline is excreted unchanged in the urine. For patients with severe renal impairment (estimated creatinine clearance of <30 ml/minute), a reduction in the dose to 1 mg daily is recommended. The same dose may be used in patients undergoing hemodialysis. In patients with hepatic impairment, dose adjustment is not needed. However, recently a case of acute hepatic injury temporally related to varenicline was reported in a patient awaiting liver transplantation. 55
Other patient groups
To date studies of varenicline are lacking in hospitalized patients, patients who are on a waiting list for a hospital procedure, and smokers who have previously quit with varenicline, but relapsed. Varenicline is a category C in pregnancy. A recent review found no studies examining varenicline use during pregnancy. 56
Psychiatric Comorbidity
Tobacco smoking is the leading preventable cause of death and disease in persons with mental illness. Persons with psychiatric illness are disproportionately affected by the tobacco epidemic, and commonly carry a high risk of tobacco-related disease, also contributing to a significantly decreased life expectancy.15–20,57 Tobacco exacerbates existing health inequalities in this population, in whom tobacco control has traditionally been neglected. Limited empirical evidence is available regarding the efficacy and safety of varenicline for smoking cessation in the mentally ill, but this substantive area has become a progressively salient focus of interest and research.
Since varenicline's launch in >80 countries globally, post-marketing surveillance has reported the emergence of neuropsychiatric symptoms in smokers trying to quit with varenicline. 58 The possible relation to the use of varenicline has become a focus of interest. Neuropsychiatric adverse event warnings, including suicidality warnings, have recently been issued for other agents59–63 indicating that agents with a wide span of mechanisms are becoming of focus of attention in regard to these warnings.
The Impact of Quitting Smoking on Mental Status
There has been increasing concern expressed regarding the potential impact of varenicline on mood and risk of suicide. Substantially confounding the issue is the fact that persons who smoke are at 2–3 fold risk of suicide,63,64 and it is widely acknowledged that abstinence from tobacco may profoundly impact mental status. To date, the differential impact of several confounders on mental status, during cessation and following longitudinal abstinence, has been poorly delineated. The potential for a contributory role of withdrawal and abstinence from a variety of psychoactive compounds in tobacco smoke (mainly nicotine and mono-amine oxidase [MAO] inhibitors), in those deciding to quit smoking, have not consistently been taken into account in interpreting associated adverse events. Our current understanding of the psychophysiological effects of withdrawal from an estimated more than 4000 chemicals in tobacco smoke is incomplete.
The withdrawal syndrome from nicotine as described in the DSM IV-TR includes dysphoric or depressed mood, insomnia, irritability, frustration, anger, anxiety, difficulty concentrating, restlessness, decreased heart rate, and increased appetite or weight gain. 65 In persons with preexisting mental illness withdrawal symptoms may be more severe, 66 and unremedied nicotine deficit states may increase the potential for risk of harm in those with mental illness, who tend to be heavier smokers and are generally more heavily addicted.
Tobacco plants contain several compounds which may inhibit MAO activity, which includes the β-carbolines, harman and norharman. 67 Higher plasma levels of norharman appear to be associated with reduced desire to smoke and relief of negative emotions. 68 During smoking cessation, levels of MAO return to previous functional levels, which may offer a biologically plausible hypothesis, at least in part, for the development of neuropsychiatric symptoms.
A further issue is that of caffeine. Polynuclear aromatic hydrocarbons (PAH) in tobacco smoke induce CYP1 A2, of which caffeine is a substrate. Following sustained abstinence from inhaling tar, the activity of specific cytochrome enzymes also diminishes. Smokers tend to consume more caffeine than non-smokers, and this may in turn offer a viable explanation for symptoms of caffeine intoxication in the days or weeks following abstinence from smoking unless caffeine intake is reduced. There is a significant and linear increase in caffeine levels (.200% of baseline) post cessation, lasting several weeks, for those who quit smoking and continue using caffeine. 69 In the absence of PAH, the bioavailability of caffeine potentially increases as a result of reduced capacity of CYP1A2, leading to potential toxicity. This may contribute to neuropsychiatric symptoms. Caffeine intoxication mimics nicotine detoxification, which may in turn cumulatively impact the anxiogenic and depressogenic effects of the abrupt withdrawal of the MAO-like agents in tobacco smoke. In persons with a preexisting history of depression or suicide, these effects may be more pronounced, and may contribute to neuropsychiatric sequelae observed in some cases.
Any report related to varenicline-associated neuropsychiatric adverse events should be interpreted against the backdrop of the variety of psychophysiological changes occurring during cessation, potentially impacting of on mental status. The expected longitudinal waxing and waning of chronic mental disorders also needs to be factored in. Cessation and varenicline-associated neuropsychiatric adverse events are summarized in the following section, and arbitrarily divided into four categories, listed in rank order of increasing methodological rigor and level of evidence, but not necessarily representing chronological order of the evidence.
Post-marketing surveillance by country-specific regulatory agencies
Once a drug is commercially available, the country-specific regulatory agency (e.g. FDA, Health Canada, UK Medicines, European Medicines Agency, and others) obtain multi-resource safety data reports for purposes of pharmacovigilance. The sources for surveillance, cast a wide net on any reported adverse event, proven to be causally related or not, and include the compound manufacturer, the public, patients, legal professionals, and any entity wishing to report an event. This method of reporting is recognized to potentially be subjective and has limited mechanisms for the validation of the authenticity of any particular report of an adverse event. It is not designed to establish the true frequency, or to determine the causality of any reported adverse event in relation to the drug used. A salient challenge relates to the nomenclature regarding suicidal ideation and suicide attempts. 70
Post-marketing surveillance has related neuropsychiatric events to the use of varenicline in persons with or without preexisting mental illness. These reports include changes in mood, agitation, hostility, depressed mood, suicidal ideation, attempted suicide, and also completed suicide. Some of these cases were reportedly complicated by nicotine withdrawal symptoms, while other symptoms occurred in persons who continued to smoke. The apportioning of the effects of nicotine withdrawal, loss of MAO inhibition, and putative caffeine or other substance effects, versus pharmacotherapy cannot be established using this methodology, and consideration for the complexity of the interactions has been rudimentary.
Following the regulatory and other reports, there has been a wide endorsement of the recommendation that the risks of using varenicline should be weighed against the benefits of its use as well as that of ongoing smoking. The health benefits of quitting smoking are immediate and are substantial, and the benefits of cessation outweigh the risks of pharmacotherapy and ongoing tobacco use. A further recommendation has followed, suggesting that those using varenicline should be observed for neuropsychiatric symptoms, including changes in behavior, hostility, agitation, depressed mood, and suicide-related events. For those persons who do experience symptoms, which are not typical for the particular individual, or if suicidal ideation or suicidal behavior develops, the advice is to discontinue the use of varenicline and to seek the necessary medical attention. Mobilization of social support systems, i.e. spouse, significant other, or caregiver, may provide supplemental information.
Although recommendations followed the regulatory administration's warnings, it should be emphasized that the particular methodological limitations of post-marketing surveillance through adverse event reporting, do not allow for determination of causality in association. Regulatory authorities have neither documented the frequency (as opposed to incidence) of neuropsychiatric adverse events, nor established that varenicline is causally associated to the development of depression or suicide. Postmarketing surveillance methodology may allow for reporting of temporal (not causal) relationships between the use of varenicline, smoking cessation, and the development of adverse events, but does not allow for interpretation on the true frequency of adverse events or of the possible causality of neuropsychiatric adverse events related to varenicline use. Since regulatory approval in the US in 2006, the FDA has alerted the public and the medical profession, and the latest FDA revision of varenicline's prescribing information and medication guide includes a boxed warning. This highlights the risk of serious neuropsychiatric symptoms, the most serious of which is suicide, and is similar to that for bupropion. 71
Post-marketing Surveillance: The Institute for Safe Medical Practices (ISMP) Report
In May 2008, the ISMP issued a report regarding the use of varenicline, citing 988 reports of serious injuries for varenicline, compared to 372 cases related to oxycodone, and 640 related to Interferon, for the 4th quarter of 2007. 58 The majority of events analyzed were reported by the manufacturer to the FDA, and the data was obtained by ISMP from the FDA. Immediate safety concerns were expressed about the use of varenicline among persons operating aircraft, trains, and other vehicles, or in other settings where a lapse in alertness or motor control could lead to massive, serious injury. The report suggested varenicline might not be safe to use in these settings and recommended “patients and doctors exercise caution in the use of varenicline and consider the use of alternative approaches to smoking cessation”.
The ISMP failed to factor in the true frequency of the adverse events in its interpretation and recommendations. This limitation in the report's methodology eroded the validity of its findings and recommendations. It does not give sufficient consideration to the potential for a causal relation of these reported events to nicotine withdrawal (or to the change in MAO and other psychoactive compounds), and fails to suggest risk-benefit approaches in consideration of the use of varenicline versus continuing to smoke tobacco.
Case reports in scientific literature
A recent analysis summarizes the psychiatric adverse drug reactions associated with varenicline in 14 case reports and open-label trials. 72 These cases represent a heterogeneous population ranging between the ages of 24–75 years. A variety of reasons were documented for discontinuation of medication, including paranoia, derealization, visual hallucinations, psychosis, agitation, hypomania, mania, anxiety, vertigo/dizziness, blurred vision, depression, suicidal ideation, and one case of suicide. 73 The majority of the case reports suggested the onset of psychiatric symptoms within days to weeks of initiation of the compound. 72 Case reports of mentally ill persons including single cases of schizophrenia, bipolar illness, and attention deficit/ hyperactivity disorder were reviewed. In these cases there was no exacerbation of psychiatric illness with varenicline treatment.
Open label clinical trials
A case series describing use of varenicline in persons with schizophrenia (n = 19) suggested no reports of adverse psychiatric drug reactions and no psychiatric hospitalizations within 24 weeks of starting varenicline. 74 A retrospective review, in veterans with high rates of psychiatric illness (n = 24), suggested a lower smoking cessation rate in those with mental illness following varenicline use. 75 This review reported no incidents of suicidal ideation, but suggested varenicline should be used with caution in this population, and with close monitoring.
The first prospective study has recently reported quantitative data on the effects of varenicline on cognition and psychopathology in persons with schizophrenia or schizoaffective disorder (n = 12) to measure the impact on cognitive functioning. 76 Varenicline was associated with significant improvements in cognitive test scores, primarily associated with verbal learning and memory, but not in scores on visual-spatial learning or memory, or attention. Although varenicline significantly decreased smoking, it did not produce complete smoking abstinence in most subjects. Further, there was no significant increase in psychopathology and no subject developed depression or suicidal ideation.
Following the suggestions that varenicline may have antidepressant effects, an open-label trial was conducted. 77 Fourteen of 18 patients (78%) completed the study; 4 discontinued due to gastrointestinal effects (n = 3) or worsened mood/irritability (n = 1). The results suggested that patients demonstrated significant improvement in depression as early as week 2. Eight patients (44%) met criteria for categorical response, and 6 (33%) reached remission criteria. Forty four per cent of subjects achieved abstinence and one-half had some reduction in smoking. The reported improvement in persistent depressive symptoms correlated with smoking cessation. There was no evidence of treatment-emergent suicidality.
In a large randomized behavioral intervention trial (n = 1117), mood, prevalence and intensity of treatment side-effects were measured in those taking varenicline, comparing respondents with a history of depression to those without a history of depression. 78 This trial reported that patients with underlying depression were more likely to experience anxiety and depression, which may be associated with varenicline and/or nicotine withdrawal, but which did not affect the smoking cessation outcomes.
A clinical observational study compared the effectiveness of varenicline (n = 208) with NRT (n = 204) and evaluated the safety and effectiveness of varenicline in people with mental illness. 79 Some smokers had been diagnosed with depression (n = 64), bipolar illness (n = 14), psychosis (n = 7), psychosis and depression (n = 24), or an eating disorder (n = 2). Varenicline was found to be equally efficacious in those with or without preexisting mental illness. Varenicline appeared to be more efficacious than NRT and was not associated with exacerbation of preexisting psychiatric illness. This study offers preliminary safety data in mentally ill persons, but the limitations include a small sample size, the heterogeneity of the sample, and lack of randomization.
Recently, an open-label trial reported on the-treatment of subjects (n = 38) with varenicline and bupropion in combination. 80 Subjects with a history of bipolar illness, psychosis, or eating disorder, as well as those with current depression were excluded. The most commonly reported side-effects in this combination trial were nausea (24%) and sleep disturbance (26%). There was no increase in depressive symptomatology or reports of suicidality.
Large-scale pooled retrospective/post-hoc analyses
In a cohort study of 80660 men and women aged 18–95 years NRT (n = 63265), varenicline (n = 10973), or bupropion (n = 6422) were prescribed during follow-up. 81 The primary outcomes measured were fatal and non-fatal self-harm, while secondary outcomes were suicidal thoughts and depression. There was no clear evidence that varenicline was associated with an increased risk of fatal (n = 2) or non-fatal (n = 166) self-harm, although a two-fold increased risk could not be ruled out on the basis of the upper limit of the 95% CI. There was no evidence that varenicline was associated with an increased risk of depression (2244 cases) (hazard ratio 0.88 [CI 0.77–1.00]) or suicidal thoughts (37 cases) (hazard ratio 1.43 [CI 0.53–3.85]).
A systematic quantitative review of the incidence and relative risk of psychiatric disorders in 10 randomized, double-blind, placebo-controlled trials of varenicline was recently published. 82 The authors reported that the incidence of psychiatric disorders other than solely sleep disorders and disturbances was 10.7% in subjects treated with varenicline and 9.7% in those treated with placebo, with an estimated relative risk of 1.02 (95% CI 0.86–1.22). There were no cases of suicidal ideation or behavior in the studies included in this pooled analysis. The review identified one case of suicidal ideation and one suicide in the trial of extended treatment and one case of suicidal ideation in the varenicline to nicotine patch comparative study;33,38 however, these cases occurred after the cessation of varenicline during follow-up phases. There were no significant increases in overall psychiatric disorders, other than sleep disorders and disturbances, in this non-mentally ill sample of smokers involved in the clinical trials. The COPD study, presented after the pooled analysis of 10 trials, reported no suicides or suicidal ideation events in varenicline-treated subjects. 51 These results from RCTs are in line with the findings of a prospective incidence study reporting a 3.6% incidence of depression in varenicline treated patients (n = 2862). 83 Finally, interim safety data from the Intensive Medicine Monitoring Programme in New Zealand also supports a low incidence of suicide in patients taking varenicline. 84 Among 3415 patients dispensed varenicline during the first year of monitoring, there was 1 death from suicide, giving a risk of 3/10000 (95% CI 0.07–16/10000).
Randomized placebo-controlled clinical trials
To date, no double-blind randomized, placebo-controlled clinical trials have been published on the efficacy and safety of varenicline in the population of persons with mental illness.
Tolerability and Safety
In clinical trials the tolerability and safety profiles of varenicline were generally acceptable.24–33,39,45,51 Nausea, the most common adverse event, is usually mild to moderate, and diminishes over time and in response to administration with food or a glass of water taken before the pill. Nausea and vomiting may reduce risk of harm in case of overdose. 85 A meta-analysis of clinical trial safety data found that nausea occurs in about one-third of patients. 35 The next three most common adverse events were insomnia, abnormal dreams and headache. Patients may be advised to take varenicline with dinner rather than at bedtime to minimize insomnia and abnormal dreams. While additional adverse events are reported more commonly in subjects taking varenicline versus placebo, including cardiovascular, psychiatric, gastrointestinal and ophthalmological events, the clinical trials did not indicate an increase in psychiatric adverse events. 82 These events were not sought using symptom-specific scales or measures beyond the routine collection of adverse events and patients with a wide range of psychiatric disorders were excluded from the trials (Tables 1 and 2).
Place in Therapy
Medical comorbidity
Many patients with medical comorbidity will have already tried NRT. In general, transdermal NRT is recommended to be combined with self-administered, short-acting forms of NRT like gum or inhaler to deal with acute cravings despite patch treatment. NRT requires frequent dosing and correct administration may be difficult for some patients to master. Varenicline may be considered a first line drug for patients with comorbidty because of high efficacy, and is particularly useful in patients who are unable to use NRT correctly, or who have tried NRT and failed.
The results of the trials in patients with CVD or COPD suggest that a longer course of therapy may be needed for patients with high dependency. This idea is supported by data from a pooled analysis of two large trials of varenicline. 86 In these studies, the effect of varenicline did not depend on degree of dependence. However, lower dependence smokers, whether categorized by number of cigarettes smoked per day or Fagerström test for Nicotine Dependence score, had higher abstinence rates than their counterparts with high dependence. This suggests that these smokers need more intense or longer treatment regimens. Future studies should determine whether long-term therapy, already shown to have a good safety profile over the course of 6 months or 1 year,32,33 helps more dependent smokers to achieve higher rates of abstinence.
Psychiatric Comorbidity
The range of neuropsychiatric problems associated with quitting smoking may likely be explained by a number of factors, including nicotine detoxification, the loss of MAO inhibition, and caffeine toxicity, especially in those with preexisting psychiatric illness. There does not appear to be a dose-response curve in the emergence of neuropsychiatric symptoms, nor a biologically plausible hypothesis whereby varenicline would directly cause serious neuropsychiatric adverse events. The summary of several lines of evidence also suggests the absence of a signal for increased neuropsychiatric sequelae of varenicline use, other than sleep disturbances. The current label includes a boxed warning declaring that depression including suicidal ideation and behavior could be associated with smoking cessation or with medication use, and that smokers taking varenicline or bupropion should be monitored with this in mind.
To date, studies have not found a disproportionate increase in depression or suicidality causally related to varenicline. Ascertaining causality is difficult as several factors are associated with neuropsychiatric symptoms. The fact that more subjects assigned to varenicline than placebo are abstinent also complicates interpretation of the data. Efforts are underway to address the question of safety in a way that identifies numerators and denominators for the adverse events.83,84 The FDA is requiring manufacturers of smoking cessation drugs to conduct clinical trials to determine how often serious neuropsychiatric symptoms occur in patients using various smoking cessation therapies, including patients with psychiatric disorders. 87
Conclusions
Varenicline should be considered a first line option for pharmacotherapy, along with the other available options, for persons with medical comorbidities. In patients with mental illness, it may be considered as first line or second line, after NRT. The use of varenicline is considered safe and effective in a broad range of populations, including the mentally ill. The current evidence does not support a contra-indication on the grounds of mental illness, or that an increase in neuropsychiatric adverse events is causally related to use of varenicline, with the exception of sleep disturbance. Persons with mental illness, who are interested in quitting smoking, should be offered varenicline in combination with psychosocial interventions, in line with the U.S. Public Health Service Guidelines. 7 Failure to offer varenicline as an option may deprive the mentally ill of an effective treatment to quit smoking.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The peer reviewers of this paper report no conflicts of interest. Up to 2009 Dr Els received unrestricted grant funding and honoraria for education and advisory work from Pfizer and Johnson and Johnson. Dr Tonstad has received honoraria for consulting and lectures for Pfizer and other manufacturers of smoking cessation medication. The authors confirm that they have permission to reproduce any copyrighted material.