
Abstract
Peripheral T-cell lymphomas (PTCL) represent about 12%–15% of non-Hodgkin lymphomas and are characterized for being a molecularly heterogenous group of diseases. The optimal treatment for PTCLs remains to be defined as they are usually refractory to existing therapies and carry a poor prognosis. Pralatrexate (PDX), a rationally designed antifolate drug, was granted FDA approval as a single agent for the treatment of relapsed/refractory PTCL in 2009. Because of its favorable toxicity profile and activity, Pralatrexate has become a major compound for patients with refractory PTCL.
Introduction
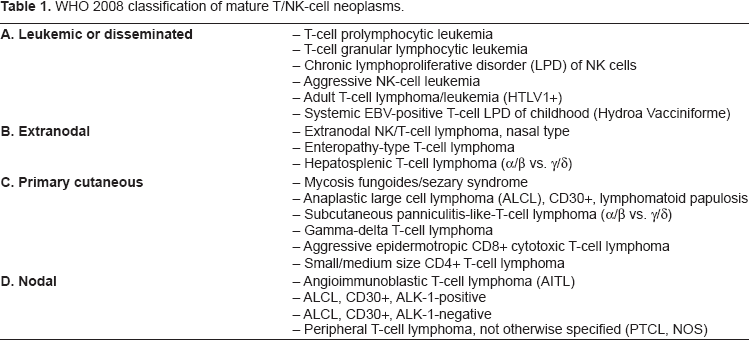
About 65,980 people living in the United States were diagnosed with non-Hodgkin's lymphoma during 2009. Non-Hodgkin's lymphoma (NHL) is the seventh most common cancer in males and females in the United States. 1 T-cell lymphoma is one entity of NHL (10%–15% of NHL) which represents a heterogeneous group of diseases that is notably more difficult to treat than B-cell lymphoma.2,3 PTCL is defined by their post-thymic origin (or mature Tcell), in contrast to the precursor T-cell neoplasm, lymphoblastic lymphoma. PTCL represent approximately 7% of NHL and it is listed as a “rare disease” by the Office of Rare Diseases (ORD) of the National Institutes of Health (NIH).4,5 The Revised European American Lymphoma (REAL) classification provided basis for the World Health Organization classification of PTCL (mature natural killer (NK)/T-cell lymphoma). In 2008, the WHO modified the classification of PTCL, dividing them into predominantly leukemic, extranodal, nodal, and primary cutaneous types. (Table 1).6,7 The most common subtypes in North America are PTCL unspecified (4% of NHL), anaplastic large cell lymphoma (ALCL) and angioimmunoblastic T-cell lymphoma (AITL). 4
WHO 2008 classification of mature T/NK-cell neoplasms.
Prognosis
PTCL is a heterogeneous disease characterized by widespread dissemination, aggressive behavior, and very poor outcome. 8 The disease carries a 5-year survival rate between 25% and 45%.2,9–13 This poor prognosis is due to lower response rates, higher relapse rates, and lower overall survival (OS). For example, in the Groupe d'Etudes des Lymphomes de l'Adulte (GELA) retrospective study, the 5-year overall survival (OS) rates were 53% for B-cell lymphomas (BCL) and 41% (P = 0.0004) for PTCL and event-free survival (EFS) rates were 42% for BCL and 33% (P < 0.0001) for PTCL. Comparison of the different histological subtypes of lymphoma showed that the 5-year OS rate for T-ALCL (64%) was superior to those of other PTCL (35%) as well as diffuse large B-cell (53%) NHL. When multivariate analysis was applied using the International Prognostic Index (IPI) (age higher than 60 years, lactate dehydrogenase (LDH) level higher than normal, ECOG performance status ≥2, advanced Ann Arbor clinical stage (III or IV), number of involved extranodal disease sites >1) as one factor, non-anaplastic PTCL remained an independent parameter (P = 0.0004). The 5-year overall survival rate was decreased to 36% and 23% for PTCL patients with two or at least three adverse risk factors, respectively. 2 In other multivariate analysis they defined the Prognostic Index for PTCL (PIT) (age higher than 60 years, impaired performance status ECOG ≥ 2, elevated LDH and bone marrow involvement) as adversely prognosis. For those with no adverse factors the 5-year survival rate was 62%; for those with one factor it was 53%; for those with 2 risk factors it was 33%; for those with three or four risk factors it was 18%. 13 However, in most series, most patients with PTCL have a higher proportion of adverse risk factors such as in GELA study; 77% of patients with PTCL had at least two adverse risk factors.2,13 Therefore the treatment decision making depends on the ability to identify a favorable group of patients as well as those with the poorest outcomes.
Initial treatment
There is no consensus as to the appropriate standard therapy for PTCL. Historically, PTCLs have been treated with strategies closely paralleling the treatment of diffuse large B-cell lymphoma (DLBCL), using CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisolone) or CHOP-like chemotherapy regimens. However, published studies show that this approach does not have the same efficacy as seen for aggressive B-cell lymphoma. The published data pertaining to the use of CHOP to treat PTCL is largely retrospective. These studies suggest that approximately 30% of patients with PTCL are cured after first line treatment. However when the analysis is limited to the patients with multiple risk factors (IPI), the estimated OS drops to approximately 15 to 20%.3,13–15 Since most patients present with widely disseminated disease and multiple adverse factors at diagnosis we can conclude that standard CHOP regimen may be adequate only for the minority of patients with favorable features, as indicated by IPI or PIT scores. One exception is anaplastic lymphoma kinase (ALK)-positive ALCL, as this type of PTCL has a much more favorable prognosis with standard CHOP-type chemotherapy than other types of PTCL. 8
The inadequacy of CHOP beckons a far better approach. Several groups have looked at intensifying chemotherapy regimens over standard doses of CHOP without apparent improvement in progression free survival rate (PFS) and OS. These include the primary use of platinum-based regimen such as ESHAP or very intensive regimens, such as Hyper-CVAD, VIP-ABVD and VP16 plus high dose cytarabine.16–21 In addition, Kim, J.G. et al conducted phase II study of Alemtuzumab (humanized monoclonal antibody binds to the CD52) plus CHOP in PTCL. This study achieved 80% overall response rate with 65% complete response (CR) and an estimated event-free survival of 43.3%. However it was closed after 20 of the planned 43 patients had been enrolled due to high incidence of the adverse infectious and hematological events. 22 The other pilot study of CHOP plus etoposide and gemcitabine also achieved high overall response rate (76.9%) and 57.7% CR. The median survival had not yet been reached and this study also had 53.8% of grade 4 neutropenia with 15.4% having febrile neutropenia. 23 Furthermore, in the International Peripheral T-Cell and Natural Killer/T-Cell Lymphoma Lymphoma Study:Pathology Findings and Clinical Outcomes, no significant difference in outcome was found between patients who received anthracycline-and non-anthracycline containing regimens except in patients with ALK-positive ALCL. 24 The choice of the initial chemotherapeutic regimen for PTCL remains a clinical challenge. Randomized clinical trials are needed to improve the outcome of these diseases.
There are several series that attempted to establish the role of frontline autologous stem cell transplantation (ASCT) as a consolidation for aggressive PTCL patients (exclude ALCL ALK+) in whom response to initial induction chemotherapy with enough number of patients and acceptable median observation time have been reported. The Nordic Lymphoma Group performed a prospective study of CHOEP (CHOP + etoposide) given every 2 weeks for 6 cycles then followed by high dose therapy (HDT)-ASCT in responding patients (excluding those ALK-1 positive ALCL). In this study, 54% of patients had high-to-intermediate or high risk disease. Seventy-three percent of patients responded to initial chemotherapy (50% CR, 35% PR) and proceeded to HDT-ASCT. At a median follow up of 24 months, 67% of patients were alive at 3 years with 4% transplant related mortality rate. 25 Corradini P, et al reported the long term-term follow up of two phase II studies in which two treatment patients were given multi-agent high-dose sequential therapy or MACOP-B (MTX, doxorubicin, cyclophosphamide, vincristine, prednisolone and bleomycin) followed by HDT-ASCT. Seventy-four percent of patients is chemosensitive (56% CR, 16% PR) and proceeded to HDT-ASCT. OS and PFS at 12 years are 34% and 30%, respectively. 26 Furthermore, in the recent two Spanish studies of 41 PTCL patients who received ASCT as a consolidation, the outcome was very good, with 86% disease free at 4 years of median follow up. From this series, the chemosensitive non-transplanted group had 2.5-fold more relapses and 2-fold less 4-year even-free survival than chemosensitive transplanted group.27,28 Another recent study was done by Reimer, P. et al also showed a good OS rate at 3 years (50%) with 47% CR and 26% PR from the induction chemotherapy. However in this study, around 30% of the patients planning to receive the transplant failed to do so mainly due to progression or toxicity. 29 There are few more studies that also showed the good OS and PFS in ASCT as a consolidation therapy.30–32
Indeed, the results of these studies showed that ASCT is relatively safe as the transplant related mortality is below 5% and the results seem to improve the outcome of high-risk features in PTCL patients both in OS and PFS but the caution should be taken, as the follow-up is still too short and only a randomized trial could confirm whether ASCT is better than other less intensive therapies.
Thus, today the patients (intermediate and high risk) who attain a good response from induction therapy may proceed to consolidation with HDT and ASCT except for ALCL with ALK-1 positive [considered to be category 2B evidence By the National Comprehensive Cancer Center Network (NCCN) Guidelines]. 33
Relapsed and refractory disease
Most of clinical series have reported poor median survivals (less than 2 years) and 5-year survival rates less than 30% especially in patients with high and intermediate-risk disease.3,14,34 Nearly one-half of patients were refractory to their initial chemotherapy in one series. 35 As mentioned above, anthracyclines do not impact survival in PTCL and CHOP-like chemotherapy regimens or the combinations may not be the optimal backbone in these poor-risk patients. P-glycoprotein expression which is known to involve to anthracycline resistance may in part of chemoresistance in PTCL patients. In normal T and NK cells, the expression of P-glycoprotein is elevated, which may explain the lack of effectiveness of anthracycline-base regimens in T- and NK- cell malignancies. 36 Thus it might be useful if we can find the chemotherapy agents that bypass the P-glycoprotein mechanism of drug resistance. Gemcitabine is a novel nucleoside analogue with a low-toxicity profile and activity in several solid tumors and it has recently demonstrated activity in hematologic malignancies. The previous study in 2001 showed a very good response rate (60%) with the use of gemcitabine as a single agent to relapsed/refractory T-cell NHL. 37 Furthermore, there are three phase II studies in relapsed/refractory cutaneous peripheral T-cell lymphoma and naïve cutaneous PTCL reported high response rate with gemcitabine monotherapy.38–40 In addition, there are few studies of gemcitabine chemotherapy combinations in relapsed/refractory PTCL in the past few years. Most of them include gemcitabine plus cisplatin and the other one is gemcitabine plus vinorelbine, all of them have overall response rate 40%–70% but they are too small of number of enrolled patients (n = 5–16).41–43 SWOG currently conducts phase II clinical trial (S0350) of cisplatin plus etoposide plus gemcitabine plus solumedrol (PEGS) in PTCL. Other regimens based on Ara-C or Platinum frequently used in salvage chemotherapy regimens have not reflected superior results to CHOP based regimens. Therefore intense treatment are being tested in order to improve these results.
HDT and ASCT should be considered in relapsed or refractory PTCL especially in patients with documented chemosensitive disease. There are several published studies of ASCT as a salvage therapy in PTCL and most of them demonstrated the similar results compared with aggressive B-cell lymphoma.44–48 Another large study with longer follow-up has been recently reported by the Spanish GEL-TAMO group. 123 patients with relapsed or refractory PTCL were transplanted as salvage therapy, 71% of patients had CR with a median follow-up of 61 months and the OS and PFS at 5 years were 45% and 33%, respectively.46,49 Several recent reports have suggested that allogeneic stem cell transplantation may be an effective therapy but they are the small series with a high rate of treatment mortality and cumulative evidences of a graft versus PTCL in patients receiving full myeloablative allogeneic transplant.50–55 In one of the phase II studies, 17 patients who had refractory or relapsed PTCL were treated with salvage chemotherapy followed by reduced intensity conditioning and allogenic stem cell transplantation. The estimated 3-year overall and progression free survival rates were 81 and 64% respectively, with donor lymphocyte infusion inducing a response in two patients who relapsed post-transplant, suggesting a graft-versus-lymphoma effect. The transplant-related-mortality was only 6% in this study. 56 Hematopoietic stem cell transplantation resulted in a feasible and an effective method to rescue patients with relapsed/refractory PTCL; also considered as consolidation treatment after first line induction chemotherapy, at least for those with chemosensitive disease as mentioned above.
The choice of chemotherapy regimen for relapsed/refractory PTCL remains a clinical challenge. New treatment approaches are urgently needed to improve PFS and OS rates in PTCL. In the past several years a number of new agents have undergone evaluation and positive results from clinical trials for PTCL are emerging. Pralatrexate (PDX), a novel agent, has shown impressive overall response rates in relapsed and refractory PTCL. 57 In the following section, we will describe the clinical development and role of Pralatrexate in PTCL therapy.
Pralatrexate and peripheral T-cell Lymphoma
In September 2009, the FDA approved PDX or Folotyn for the treatment of relapsed or refractory peripheral T-cell lymphoma. The FDA recommends a seven-week treatment cycle: 30 mg/m2 of PDX administered by intravenous (IV) push over three to five minutes through the side port of a free-flowing IV line of 0.9% Sodium Chloride injection once per week for six consecutive weeks followed by no treatment during the seventh week. Therapy should continue until the lymphoma progresses or an unacceptable toxicity occurs. In addition patients should receive vitamin B12 and folic acid supplementation. 58
Pralatrexate
Pralatrexate (PDX, 10-propargyl 10-deazaaminopterin) is a novel targeted antifolate (small molecule dihydrofolate reductase, DHFR inhibitor), developed by Allos Therapeutics Inc. under license from Memorial Sloan-Kettering Cancer Center, Southern Research Institute and Stanford Research Institute International. It is a 10-deazaaminopterin derivative which is structurally similar to methotrexate (MTX; one of antifolate) with only a propargyl group substitution at carbon 10. However, PDX possesses a greater anti-tumor effect and has a higher affinity for the reduced folate carrier type 1 (RFC-1).59–63 The cellular uptake of antifolate agents is mediated by RFC-1, while the antifolates are retained intracellularly via polyglutamylation catalyzed by folylpoly-gamma-glutamate synthetase (FPGS). 64 RFC-1 is a fetal oncoprotein, the principal transporter through which folates and antifolates enter the cell, and it is preferentially overexpressed in fetal and malignant tissues. RFC-1 is also known to be up regulated by a variety of oncogenes such as H-ras, c-myc.59,60,65,66 The high level expression is related to the demands for natural folates required by cell proliferation and in order to meet the demands for purine and pyrimidine nucleotides during DNA synthesis. Previous pharmacokinetic studies have shown that PDX is much more efficient for RFC mediated internalization than MTX. Biochemically, the influx Vmax/Km (Vmax/Km = a measure of the rate of capture of substrate by free enzyme into a productive complex destined to form a products and complete a turnover at some later time) mediated by RFC shows PDX is far more efficiently transported, incorporated at a rate nearly 14 times greater than MTX and 3 times greater than edatrexate (EDX).60–62,67–69 Furthermore, PDX is also a more effective substrate for FPGS (Vmax/Km data for FPGS mediated glutamylation reaction suggest that PDX is 10-fold greater than MTX and 2-fold greater than EDX).60–62,67–69 These biochemical features of PDX suggest that PDX should have a more potent antineoplastic activity compared with MTX and EDX and it should overcome mechanisms of MTX resistance caused by RFC-1 downregulation and/or FPGS leads to MTX resistance.
In vitro studies
A preclinical model of lymphoma confirmed the superiority of PDX over MTX in human lymphoma cell lines RL (transformed follicular), HT (DLBCL), Hs602 (B-cell lymphoma), Hs445 (Hodgkin lymphoma), Raji (Burkitt's lymphoma) and SKI-DLBCL-1 (de novo DLBCL). The cytotoxicity assays demonstrated the IC50 of PDX (IC50 = 3 to 5 nM) consistently 1-log below that seen with MTX (IC50 = 30 to 50 nM) against all cell lines, including a very chemotherapy-refractory transformed lymphoma carrying the 14:18 translocation. 63 There are no data in T-cell lymphoma cell lines.
In vivo studies
PDX was also consistently found to be superior to MTX in an in vivo model. NOC/SCID mice xenografted with HT, RL, and SKI-DLBCL-1 tumor cells were treated intraperitoneally with a saline control, PDX (60 mg/kg) or MTX (40 mg/kg) twice weekly for three or four doses. Complete lymphoma regression was observed in 89, 56, and 30% of PDX-treated HT, RL and SKI-DLBCL-1 xenografted mice, respectively, whereas complete regressions were not observed following treatment with MTX. Furthermore, quantitative reverse transcription polymerase chain reaction (qRT-PCR) for characterization of the markers of antifolate activity including RFC-1, FPGS, and folylpolyglutamate hydrolase (FPGH) revealed an obvious correlation between the level of RFC-1 expression and the incidence of complete remission in xenografted model (RFC-1 expression level in HT, RL, SKI-DLBCL-1 were 0.96, 0.41 and 0.3, respectively), suggesting that the level of RFC-1 gene expression may be a predictor of response to PDX. There was no significant difference seen in the expression of FPGS or FPGH. 63
Clinical development
Sixteen patients with relapsed/refractory lymphoma including Hodgkin's disease (n = 5), aggressive B-cell lymphoma (n = 8), mantle cell lymphoma (n = 2) and one patient with peripheral T-cell lymphoma were treated with PDX single agent at a dose of 135 mg/m2 intravenously given every other week extrapolated from phase I data in the aforementioned lung cancer study. The trial also allowed supplementation with folic acid and vitamin B12 for patients who developed stomatitis. All patients developed mucositis-related adverse events. The only patient who had a complete remission (CR) after one dose of PDX, was a middle-aged man with history of very chemorefractory PTCL-nos. Additionally, a higher incidence of stomatitis was associated with marked elevations in pretreatment homocysteine and methylmalonic acid levels, which were reduced by folic acid and vitamin B12 supplementation. After normalization of homocysteine and methylmalonic acid level, the patients did not develop progression to advanced grade stomatitis. 70 Due to the high incidence of stomatitis, the phase I portion of the trial was subsequently modified to a dose-escalation study, beginning at 30 mg/m2 weekly for 3 weeks in a 4-week cycle, progressing to 30 mg/m2 weekly for 6 weeks in a 7-week cycle, and increasing by 15 mg/m2 on the 7-week schedule.
All patients received folic acid and vitamin B12 supplementation. The maximum-tolerated dose (MTD) was 30 mg/m2 weekly for 6 weeks in a 7-week cycle, and the incidence of stomatitis was 17%, a marked reduction compared to the every other week schedule. 71 This trial was then expanded to phase II study in B-cell and T-cell lymphoma at a dose of 30 mg/m2 weekly for 6 weeks in a 7-week cycle. Of 48 evaluable patients, the overall response rate was 31%, including 17% who experienced CR. When analyzed by lineage, the overall response rates were 10% and 54% in patients with B- and T-cell lymphomas, respectively. All patients who achieved CR had a diagnosis of T-cell lymphoma and 4 of the first 5 patients achieved CR within the first cycle of treatment. The duration of response ranged from 3 to 26 months. From this trial, it was deduced that pralatrexate has significant single-agent activity in patients with relapsed/refractory T-cell lymphoma. In addition, quite remarkably, normalization of elevated homocysteine and methylmalonic acid levels by pretreatment with vitamins completely abrogated the previously noted dose-limiting toxicity of stomatitis. Hematologic toxicity was minimal with 50% reduction in cytopenias once the weekly reduced schedule was adopted. 71
A phase II, non-randomized, open-label, multicenter clinical trial, Pralatrexate in Relapsed or Refractory Peripheral T-Cell Lymphoma (PROPEL) was conducted under the FDA Special Protocol Assessment Program. This trial has led to the approval of this agent for the treatment of relapsed and refractory PTCL in 2009. 115 patients were enrolled, 109 patients were evaluable for efficacy. All patients received 30 mg/m2 weekly of PDX for 6 weeks in a 7-week cycle with vitamin supplementation. Patients had failed a median of 3 prior regimens, 16% of patients had previous autologous stem cell transplantation, and 25% of patients had never responded to any prior therapy. The overall response rates were 27% and 39% by central review and by investigators, respectively. This discrepancy can be explained by the underestimated evaluation of patients with skin lesion. It cannot be adequately captured by photography alone. 11 patients had CR, 18 patients had PR and 24 patients had SD. Furthermore, 69% of responders were after just 1 cycle. The most adverse events were mucosal inflammation (grade 3 = 17%, grade 4 = 4%) and thrombocytopenia (grade 3 = 14%, grade 4 = 19%). 72
Pralatrexate in combination with gemcitabine for the treatment of lymphoma
The combination of pralatrexate (2 nM) and gemcitabine (20 nM) was assessed in the human NHL cell lines SKI-DLBCL-1, HI, DOHH2 and RL, all of which were exposed to one drug for 24 h followed by the same drug or the other drug for a further 24 h, or to the combination for 24 h. Synergistic cytotoxicities were observed in all cell lines, and the strongest synergistic effect was noted when pralatrexate was administered prior to gemcitabine. The same combinations of pralatrexate and gemcitabine were tested in mice xenografted with SKI-DLBCL-1 cells. The mice received four intraperitoneal doses twice weekly of saline control, pralatrexate (60 mg/kg), gemcitabine (60 mg/kg) or the combination of pralatrexate and gemcitabine (administered concomitantly at doses of 30 mg/kg). Rapid disease progression was observed in controls, leading to euthanasia of the animals at 22 days following the initiation of treatment. Following monotherapy, tumor volumes initially decreased, but then increased to 739.0 and 317.7% of the initial tumor volume by day 44 for pralatrexate and gemcitabine, respectively. In contrast, tumor reductions of 63.1% of the initial tumor volume were observed by day 44 in mice receiving the combination; three complete regressions, one partial regression and one case of disease progression were observed (out of five animals).73,74 An important study, published in 2006, found that the sequence of PDX followed by gemcitabine was five times more effective at inducing apoptosis when compared with the simultaneous exposure of PDX plus gemcitabine. In addition this regimen schedule had superior cytotoxicity than the combination of MTX and cytarabine, even using one-quarter of the maximum tolerated dose of the PDX and gemcitabine combination. 75
At the 51st ASH Annual Meeting And Exposition, December 2009, Steven M. Horwitz presented Phase I results of PDX and gemcitabine in patients with relapsed or refractory lymphoproliferative malignancies. This trial was a multi-center phase 1/2a study (PDX-009; NCT00481871), and the primary objective of the phase I portion was to determine the MTD. Thirty-four patients were enrolled including B-cell lymphoma (n = 13), T/NK cell lymphoma (n = 11), Hodgkin's lymphoma (n = 7), and other lymphomas (n = 3). Patients were randomized into three groups. Group A (n = 7) received PDX on day 1 and gemcitabine on day 2, once weekly for 3/4 weeks. Group B (n = 10) also received PDX and gemcitabine on sequential days, but were only treated every 2 weeks (q2w). Group C (n = 17) received PDX followed 1 hour later by gemcitabine on the same day q2w. All patients received vitamin supplementation (B12 and folate). Those patients in group A treated with once-weekly sequential-day dosing with PDX 10–15 mg/m2 and gemcitabine 300–400 mg/m2 had dose-limiting toxicities (DLTs) of thrombocytopenia and/or neutropenia, thus accrual to this schedule was halted and subsequent cohorts received the q2w schedule. They found the MTD with the q2w dosing schedule was PDX/gemcitabine 10/400 mg/m2 when given on sequential days (group B) and 15/600 mg/m2 when given on the same day (group C). 7 patients (21%) achieved PR and responses were seen in patients treated on the same day as well as the sequential day schedules. From this phase I clinical trial, they concluded that the treatment with PDX and gemcitabine is feasible with acceptable toxicity, when administered on a q2w schedule. In addition, the MTD of each drug is 50% greater when given on the same day as compared to treating on the sequential day. 76 However, phase II expansions at the MTD will explore both sequential-day dosing and same-day dosing in a q2w schedule.
Pralatrexate toxicities
The common toxicities of PDX include mucositis, stomatitis, bone marrow suppression, nausea, and fatigue. From the PROPEL study, the most adverse events were mucosal inflammation (grade 3 = 17%, grade 4 = 4%) and thrombocytopenia (grade 3 = 14%, grade 4 = 19%). 72
The FDA recommends that patients should receive folic acid 1–1.25 mg by mouth daily and vitamin B12 1 mg by intramuscular. injection every 8–10 weeks. Folic acid therapy should start in the 10 days preceding the first dose of PDX and continue for 30 days after the last dose. Vitamin B12 therapy should start no more than 10 weeks before the first dose of PDX. 58 Supplementation of MTX therapy with folic acid also has been demonstrated to be beneficial in reducing MTX-induced side effects. 77 When PDX treatment was supplemented with Vitamin B12 and folic acid in patient with NSCLC, no dose limiting toxicities were observed at doses of 150–230 mg/m2 and the MTD was able to be then increased to 270 mg/m2. 78
Other Emerging Agents
Recently there have been eight groups of novel agents for the treatment of relapsed/refractory PTCL other than PDX that are currently being investigated.
Nucleoside analogues/antimetabolites; neralabine, clofarabine, pentostatin, gemcitabine, forodesine and PDX.79–85
Histone deacetylase inhibitors; desipeptide and suberyoylanilide hydroxamic acid (SAHA), para-binostat and belinostat.86–88
Mammalian target of rapamycin (mTOR) inhibitors; temsirolimus and everolimus (for which only preliminary information is available).
Proapoptotic agents; oblimersen, obatoclax, AT-101 and ABT-263.91,92
Monoclonal antibodies; alemtuzumab, SGN-30, zanolimumab and siplizumab.95–97
Immunotoxins/immunoconjugates; delileukin diftitox, SGN-35 and daclizumab.98,99
NCCN guideline 2010, suggested that PDX, alemtuzumab, bortezomib, denileukin diftitox, gemcitabine should all be considered as second-line treatments for relapsed/refractory PTCL (non-candidate for HDT with stem cell rescue) but there are limited data for alemtuzumab and bortezomib.
Conclusion and Future Direction
Patients diagnosed with PTCL are faced with an aggressive disease, poor prognosis and very few treatment options. Only recently international efforts are putting into motion both biological studies and targeted new treatment for PTCL. PDX was rationally developed as an antifolate to target the high affinity RFC-1 and it is a more effective substrate for FPGS than other agents in the same class. PDX has demonstrated impressive activity in vitro and in vivo in several tumor types, including lymphomas. In T-cell lymphoma, PDX has shown significant anti-tumor activity, particularly in patients with PTCL, therefore gaining FDA approval as single agent therapy in relapsed or refractory cases. However, it displays minimal activity in patients with Hodgkin's lymphoma or other forms of B-cell lymphoma, the basis for which is not well understood. Contrary to other antifolates, PDX is well tolerated when it is administered along with vitamin supplementation. Future efforts are being aimed at finding additional surrogate markers of response such as distribution of RFC-1 on the surface of B- and T-cell malignancies and other markers of antifolate activity. Furthermore, combinations of PDX with other chemotherapeutic agents or targeted agents are being tested in clinical trials to improve the potency and efficacy of treatment in both hematologic and solid malignancies.
The development of optimal therapeutic modalities for PTCL remains a clinical challenge given the disease's rarity and biological heterogeneity. A multicenter collaboration is needed to ensure adequate patient enrollment to clinical trials aimed at improving strategies of treatment in the near future.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.