
Abstract
In today's healthcare environment prevention plays a pivotal role. With the aging population, herpes zoster (HZ) pain and post-herpetic neuralgia (PHN) are two conditions that will have a significant impact on the healthcare industry. The common held belief that HZ patients are protected from recurrence, after one episode of shingles no longer holds true. In a recent study data has shown recurrence rates of over five percent. The evidence suggests those who experienced pain lasting more than 30 days after the initial onset of shingles were more likely to have a recurrence, especially in the first three to four years after the initial episode. 6 Understanding the variables that influence the patient s perspective of pain can impact healthcare delivery. Increasing the quality of life for the elderly through preventive measures including education, immunization, and implementation of early treatment guidelines can significantly reduce the incidence of PHN.
Patient Perspectives in the Management of Post-Herpetic Neuralgia
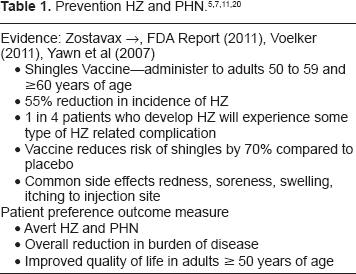
Herpes zoster (HZ) pain and post-herpetic neuralgia (PHN) are two conditions that are predicted to have a significant impact on the aging population unless health care providers give specific attention to prevention and treatment guidelines. PHN can be defined as the persistent pain of HZ that last for more than three months after the resolution of the herpetic rash. 1 Although, the incidence of PHN is common, the precise definition may vary among providers. It is estimated that 10%–20% of all patients with HZ age > 50 and up to 30% of those age ≥ 80 will be affected by PHN. 2 The duration of PHN is highly variable lasting for several months or even years after the rash resolves. 3 According to the Centers for Disease Control and Prevention (CDC), there are approximately one million cases of shingles each year in the United States (US) and about one-third of the US population will get shingles at some point in their lives. 3 Preventing HZ and averting the development of PHN can be accomplished through vaccination programs that focus on administering the shingles vaccine to adults ≥ 50 to 59 years of age as well as those 60 years and older, and implementing early treatment guidelines for patients diagnosed with HZ. 11 Improving the quality of life for older patients through the use of evidenced-based treatment guidelines can reduce pain and suffering, and the economic burden of HZ.
Clinical Studies
Research findings from the Shingles Prevention Study (SPS), a large clinical trial established efficacy of the shingles vaccine for the prevention of shingles in individuals 60 years of age and older. The SPS study compared the shingles vaccine to placebo in an effort to assess the overall incidence of HZ. The study involved 38,000 adults who were 60 years or older and found that the vaccine reduced the overall incidence of HZ in older adults by approximately 51% and reduced the incidence of PHN by 67%. 4
In an effort to identify the incidence and complication rates of HZ prior to the introduction and administration of the shingles vaccine, a population-based study was conducted. This study by Yawn and associates found the incidence of HZ and the rate of HZ associated complications increased with age, and 68% of the cases occurred in individuals 50 years of age and older, PHN occurred in 18% of the patients with HZ and in 33% of those 79 years of age and older. 5 Data from the study revealed that HZ primarily affects immunocompetent adults older than 50, with at least one in four patients experiencing some type of HZ related complication. 5
Yawn and associates have continued to follow the patients from this study group for an average of eight years, examining their medical records to determine whether any of the patients had been treated for a second episode of shingles. The data revealed a recurrence rate greater than 5%, the same rate expected to be seen in an age-matched cohort for first time cases of shingles. 6 The evidence also found that women are more likely than men to have shingles and more likely to experience recurrence. It is worth noting that the team had suspected higher recurrence rates in older patients, however, age did not make individuals more susceptible to recurrence. 6 The most striking determinant for recurrence was the patients pain during the initial episode. Individuals who had experienced pain lasting more than 30 days after the initial onset were more prone to have another bout of the disease, especially in the first three to four years after the initial episode. 6 The study findings suggest that the shingles vaccine, which is known to reduce first-time occurrences of shingles by 50%, can also prevent a second episode of the disease. 6 The information from this study can give practitioners and patients a better understanding of the risk of recurrence and the benefits of immunization and disease prevention.
In March 2011, the US Food and Drug Administration (FDA) approved the use of the shingles vaccine, Zostavax, for the prevention of shingles in individuals 50 to 59 years of age. 7 Approval was based on an international multicenter study conducted by the United States and four other countries in approximately 22,000 people who were 50–59 years of age. 7 According to the FDA news release half of the study group received the vaccine and half received a placebo. The study participants were monitored for the disease for at least one year. The results indicated that compared with placebo, Zostavax reduced the risk of developing shingles by approximately 70%. 7
Concern has been reported in that HZ has not been correctly perceived by many practitioners, who have considered it a mild and readily treatable disease. However, treatment options remain inadequate, especially for PHN. 8 Efforts at prevention of HZ and PHN are important in that 40% to 50% of those with PHN do not respond to any type of treatment. 1
Place in Therapy
In today's healthcare environment prevention plays a pivotal role, it is essential for practitioners to educate their patients and prescribe the shingles vaccine (Zostavax). Approximately one million episodes of HZ occur in the US each year, until recently, the only identifiable risk factor for this condition has been age and immunosuppression. 9 In a retrospective cohort study by Tseng and associates, individuals enrolled in a general practice setting from Kaiser Permanente Southern California health plan were evaluated for the risk of HZ after receiving the shingles vaccine. 9 Findings from the data complemented the results of the SPS findings. Indicating a reduction in risk of HZ in a community setting with its mixed population and routine clinical practices, and the vaccine was associated with reduced risks of ophthalmic HZ and hospitalizations potentially attributed to HZ. 9 These results suggest that these potential benefits extended to individuals of all ages for whom HZ vaccine is recommended, and to individuals with chronic diseases. The vaccine was found to be associated with a 55% reduction in incidence of HZ, which is consistent with the 51% vaccine efficacy reported from the SPS. 9
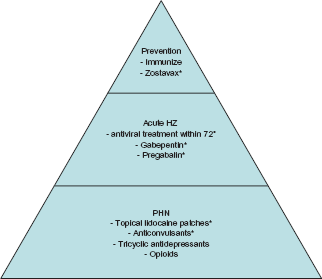
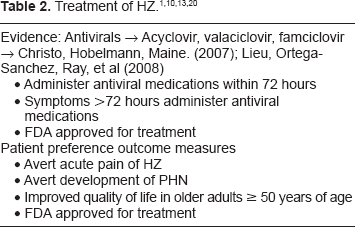
Several studies have provided evidence that administering antiviral agents within 72 hours of the onset of HZ lesions can reduce symptoms of acute pain and may attenuate the burden of PHN.1,10 Additionally, the evidence supports that patients who delay treatment for more than 72 hours can still benefit from antiviral treatment. Current research findings indicate that valaciclovir, famciclovir, and aciclovir have shown equivalent efficacy in enhancing the resolution of HZ related pain and PHN. 10 Administration of any of these three antiviral medications–-valaciclovir 1000 mg orally three times a day for seven days or famciclovir 500 mg orally three times a day for seven days or acyclovir 800 mg five times a day for seven to ten days have shown to be effective in relieving the pain and duration of HZ. Incorporating antiviral therapy as an initial step in treatment for older patients presenting with acute HZ is critical to controlling the burden of symptoms. 10
Research evidence provided by the American Academy of Neurology (AAN), has established a classification of evidence and formulation of recommendations for the treatment of PHN. The treatment categories as outlined by the AAN are divided into four groups with Group I–-indicating medium to high efficacy, good strength of evidence, and low levels of side effects. The options for Group I treatment include gabapentin, topical lidocaine patches, oxycodone or morphine sulfate (controlled release), pregabalin, and tricyclic antidepressants (TCAs). 1 Group II–-category indicates lower efficacy than those listed in group I, or limited strength of evidence, or side effect concerns. In Group III–-there was no evidence indicating efficacy compared to the placebo group and in Group IV–-the reports of benefit were limited to class IV studies. 1
Safety/Efficacy
Immunization
The FDA has approved the use of Zostavax for the prevention of shingles in individuals 50 to 59 years old, as well as those ≥60 years old. 11 The efficacy of the vaccine was determined and then licensed in 2006 for adults age 60 and older. Approval in 2011, for administration of the vaccine to a younger age group, will provide additional opportunity to prevent the often painful and debilitating disease. 11
The vaccine is administered in a single subcutaneous injection, preferably in the upper arm. Zostavax is recommended for the prevention of HZ and its complications in most adults even those who are frail or taking multiple medications for chronic illnesses. The only individuals who should not take the vaccine are those who are on immunosuppressant agents, such as high-dose prednisone or cancer chemotherapy, and those with immunodeficiencies due to AIDS, leukemia, lymphoma, or certain types of tumors affecting the bone marrow or lymphatic system. Patients who are allergic to neomycin or any component of the vaccine also should not receive it. 11 The vaccine is not recommended for women who are pregnant and it is important to note that the shingles vaccine is not a treatment for active cases of HZ or PHN.3,4
Research indicates that the vaccine is effective for at least six years and may last even longer. Common side effects reported from the vaccine includes redness, soreness, swelling or itching at the injection site, and headache. 12
Antivirals
Antiviral medications such as acyclovir, valaciclovir, and famciclovir are all safe and well tolerated in the aging population, however, adjustments maybe necessary in elderly patients who exhibit renal compromise. 10 These antivirals in a randomized controlled trials have shown equivalent efficacy in enhancing, the resolution of HZ and PHN. 10 Acyclovir, valaciclovir, and famciclovir are the only three medications approved by the Federal Drug Administration (FDA) for the treatment of HZ. 13
Tricyclic antidepressants
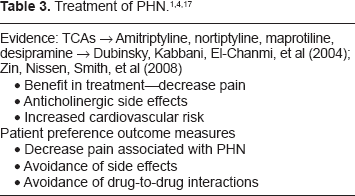
As outlined by the AAN, TCAs have been found to be of benefit in the treatment of PHN. Additional benefits of TCAs can be attributed to their sedative properties (antihistaminergic) and anxiolytic actions, given the fact that patient s who experience PHN frequently report sleep disturbances and anxiety. 10 Although, the efficacy of TCAs amitriptyline, nortriptyline, maprotiline, and desipramine has been established, practitioners must consider the anticholinergic effects associated with these medications when prescribing for the elderly. As cited by Hawksley, systemic review supports TCAs as the preferred choice of treatment for PHN, but use can be difficult in the elderly, the very patients most likely to suffer from PHN. 15 Adverse effects from TCAs include drowsiness, dry mouth, urinary retention, sedation and blurred vision as well as many drug-to-drug interactions. In the elderly, caution should be taken due to the occurrence of orthostatic hypotension, which increases the risk of falls and hip fractures. TCAs require special precautions when administered to patients with cardiovascular disease, due to the increased risk of arrhythmias, myocardial infarction and congestive heart failure. 16 In December of 2009, the NGC released new safety information that extreme caution should be used when prescribing desipramine to patients who have a family history of sudden death, cardiac arrhythmias, and cardiac conduction disturbances. 14
Anticonvulsants
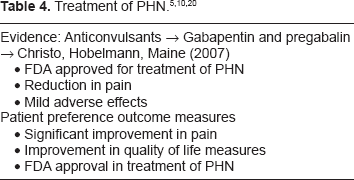
The roles of anticonvulsants, especially gabapentin, and pregabalin have been identified as effective in the treatment of PHN. Carbamazepine an older anticonvulsant is used less frequently in the management of PHN, due to intolerable side effects. Research from several randomized controlled clinical trials demonstrates that both gabapentin and pregabalin are effective at reducing pain, improving sleep patterns, and overall quality of life in patients with PHN. 15 In 2001, researchers studied 334 patients in a randomized, double blind, placebo-controlled trial, this study findings substantiated that one-third of the subjects in the gabapentin-treated group reported ≥50% reduction in pain as compared to the 14% in the placebo group. 10 From these findings the investigators concluded that “gabapentin treatment led to significant improvements in multiple validated pain and quality of life measures and was associated with few and generally mild adverse effects.” 10 When considering pregabalin and gabapentin the healthcare team should monitor the patient closely for side effects which include dizziness, somnolence, peripheral edema, headache, and dry mouth. 15 Both gabapentin and pregabalin have been approved by the FDA for the treatment of PHN. 13
Opioids
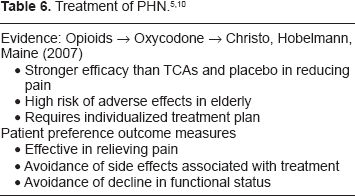
The role of opioids in the treatment of PHN has been questioned by many practitioners due to the risk of adverse effects in elderly patients. In one study researchers compared the efficacy of opioids with those of TCAs and placebo in patients with PHN. The findings concluded that patients preferred opioids over TCAs, and placebo; the patients reported greater pain relief with the opioids (38%) than TCAs (32%), or the placebo (11%). 10 Short term treatment with opioids can be effective in the treatment of acute pain associated with HZ and PHN, however, consideration should be given to long term treatment due to the addictive qualities of the medication.
In a randomized, placebo-controlled, double blind, crossover trial control-release oxycodone was shown to reduce persistent PHN pain by 50% compared with placebo among the 22 of 38 patients who completed the study. 10 The evidence supports the findings that opioids have a place in management of PHN, however, there are no specific dosage recommendations for opioid treatment. Each patient should be evaluated and treated according to their individual health needs and current health status. To ensure optimal pain control the patient's pain level should be assessed routinely through a comprehensive assessment, to identify any adverse effects or decline in functional status that could be associated with the treatment plan.
Topical lidocaine patches
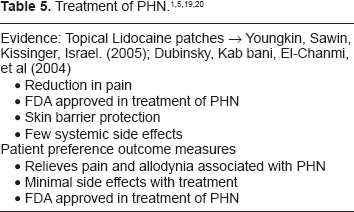
Based on the evidence found in the literature topical lidocaine is effective in reducing pain and allodynia associated with PHN.1,10 In three randomized, placebo-controlled studies of lidocaine patches a pain reduction benefit was reported in 91% of the subjects. 1 Additionally, the lidocaine patch offers protection against mechanical irritation of sensitized skin and can be considered effective in the relief of irritation in patients with marked allodynia. 10 Topical lidocaine patches have been approved by the FDA for treatment of PHN and considered an excellent adjunctive therapy for the elderly.
As outlined by the AAN, other treatment plans have been used; however, there is a lower/limited level of evidence to support their effectiveness in the treatment of PHN. The management of neurological symptoms associated with PHN which includes dysesthesia, paresthesia, hyperalgesia, hyperesthesia, and allodynia should occur between the patient and practitioner where an individualized treatment plan is developed to meet the unique needs of each patient.
Mechanism of Action, Metabolism and Pharmacokinetic Profile
Zostavax an adult vaccine is a lyophilized formulation of the Oka-Merck strain of live, attenuated varicella zoster virus (VZV). Live, attenuated vaccines produce few or no symptoms related to varicella zoster infection. 16 Inactive ingredients include sucrose, porcine gelatine, sodium chloride, monosodium L-glutamate, sodium phosphate dibasic, potassium phosphate monobasic, potassium chloride, MRC-5 cells (DNA and protein), neomycin, and bovine calf serum. 16 The increase in cell-mediated immunity is comparable with that observed with natural disease. VZV specific, cell-mediated immunity is long lasting, with a half life of 54 weeks. The onset of immunity occurs within 30 days of vaccination. 16
In a randomized, double blind, crossover trial researchers found amitriptyline, nortriptyline, maprotiline, and desipramine effective in lessening the pain of PHN. 6 The main mechanism through which the TCAs are thought to produce pain relief is inhibition of noradrenaline and serotonin reuptake in the central nervous system (CNS), which in turn activates descending analgesic pathways. 17 TCAs are involved in the suppression of neuronal hyperexcitability through several mechanism which include inhibition of sodium and calcium channels, inhibition of adenosine receptors and inhibition of NMDA receptors. 17
When evaluating the mechanisms of action and metabolism of anticonvulsants; gabapentin, pregabalin, and carbamazepine are considered. Gabapentin is thought to have a unique mode of action at calcium channel receptors in the spinal cord, and pregabalin, has similar structure and actions. 15 Gabapentin is readily absorbed after ingestion and not metabolised, therefore, the medication is primarily excreted unchanged in the urine. 13 Carbamazepine is metabolised by oxidation before excretion in the urine. Pregabalin is excreted through the kidneys and pharmacokinetic studies have demonstrated that apparent clearance is correlated with the patient's estimated creatinine clearance. 18 Researchers have also validated pregabalin as having greater analgesic properties than gabapentin. Several randomized, placebo-controlled studies have reported rapid pain reduction with pregabalin therapy. 10
Oxycodone an opioid agonist is thought to produce pain relief through putative K2-opioid receptors, although some studies claim that it is a μ-opioid agonist. 17 “Morphine produces its analgesic effects primarily through μ-opioid receptors.” 17 The onset of action for morphine sulphate is 15–60 minutes and can last for up to three to seven hours, similarly, the onset of oxycodone is 15–30 minutes with duration of four to six hours. Both medication experience extensive hepatic metabolism and are eliminated through the kidneys. 19 When considering opioids in the management of PHN the benefits must be weighed against the possible adverse side effects. According to the NGC new safety guidelines released in May 2010 when considering tramadole in the management of PHN update warnings have been included to emphasize the risk of suicide for patients who are addiction-prone, taking tranquilizers or antidepressant drugs and also warns of the potential for overdose in this subset of patients. 14
Few systemic side effects have been associated with topical lidocaine patches. The lidocaine patch produces an analgesic effect without causing local anaesthesia, meaning there is still normal sensation to the underlying skin. 10 The cause behind this effect has not been fully explained, but one theorist suggest that the “formulation delivers sufficient amounts of lidocaine to block sodium channels in small, damaged or sensitised pain fibres, but insufficient amounts to block sodium channels in large myelinated A-β sensory fibres.” 10 When prescribing topical lidocaine patches consideration must be given to the amount of lidocaine absorbed, which is directly related to the surface area of the skin covered and the length of time the patch is worn. The literature recommends a maximum of three patches to be worn at one time for no longer than 12 hours in a 24 hour period. 10
The pain associated with HZ and PHN are difficult to control in the elderly population, where pain medications offer their own set of risk and adverse effects. The elderly are more likely to experience adverse effects from new medication due to age related changes in pharmokinetics and pharmacodynamics. 4
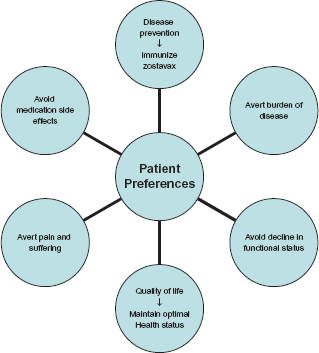
Patient preference
Healthcare practitioners and intra-professional teams who understand the burden of HZ from the patient's perspective are in a position to initiate preventive measures through education, immunization, and implementation of early treatment plans that can significantly reduce the incidence of PHN. Several prospective and retrospective studies have tried to define and quantify the burden of HZ and PHN.
In one retrospective, population-based study researchers found that HZ was more common in women than in men, in addition to older age and immune status; female sex was an independent risk factor for HZ, and also for PNH. 2 This is thought to be related to a different immune response that women have to the latent viral infection, which would account for their increased risk compared to men. 2 Economic burden of HZ from this study were identified by hospitalization rates and medication cost. There was a direct correlation between older age and hospitalization, with the rates of hospitalization increasing progressively for each decade up to 85 years. The direct cost associated with inpatient care for a single case of HZ was more than 20 times the cost for outpatient care and the direct cost associated with inpatient care for one episode of PHN was more than five times the cost for outpatient care. 2 Disease prevention measures that focus on immunization, and education plans can reduce the incidence and cost associated with HZ and PHN. Patients who are aware of risk factors such as female sex, older age, and altered immune status can avoid the pain and suffering of the disease, by receiving the Zostavax vaccine. Not only does the patient benefit but the overall economic burden of the disease is reduced.
Quality of life (QoL) is another important aspect of a patient's perspective that researchers have tried to measure to understand the burden of HZ and PHN. Pickering and Leplege, defines the aim of QoL measurement as a way to evaluate, with the best scientific approach, how people perceive changes in their health status in relation to various situations like preventive measures, drug, or nondrug treatments for pain. 20 The World Health Organization (WHO) defines QoL as “a state of complete physical, mental and social wellbeing, and not merely the absence of disease or infirmity.” 8 QoL tools rely on subjective data attained through standardized and validated health status questionnaires. When evaluating research data, QoL tools can complement other instruments that investigate health-related/medico-economic aspects or pain associated with HZ and PHN. 20
Research findings have shown that QoL outcomes are highly correlated to the severity of pain experienced with HZ and PHN. Many patients have reported poor physical functioning, affective components of pain to depression, and psychological impairment and overall pain burden to poor social and role functioning. 5 QoL outcome measures indicate that elderly patients may experience a permanent loss of independence; never fully regaining their lifestyles, interests and levels of activity. 5 Further complications associated with PHN includes loss of physical function (ability to perform activities of daily living), fatigue, anorexia, weight loss, reduced mobility, physical inactivity, sleep disturbances, and overall decline in health status. 5
In a recent research study, the authors sought to understand the value that community members and patient's placed on preventing HZ and PHN. The study evaluated the data (hypothetical scenarios) from community members not affected by HZ or PHN and patients with current experience of HZ or PHN. The questionnaires included time trade-off questions and willingness-to-pay questions. Overall, community members were found to be willing to trade substantial amounts of time or money to avoid HZ, even in the least severe scenarios. The results indicated that community members traded less money than patients who had experienced either HZ or PHN. 20 Patients who were male, with higher income that had experienced HZ or PHN were associated with higher willingness to pay to avoid HZ. 20 This information is consistent with other studies in which discrepancies were noted between health-state valuations of patients and health state valuations from the general public. 20 One explanation to this outcome is the fact that actually experiencing pain may change a person s idea of what the numbers 1 to 10 on a pain scale mean. 20 In an effort to provide safe and effective treatment, healthcare teams should consider patient preferences and perspectives for prevention and treatment of HZ and PHN.
Conclusion
The healthcare workforce has many opportunities to bring attention to this increasing healthcare problem. Reducing the incidence of HZ and PHN is the desired outcome for healthcare providers and patients in the 21st century. This goal is achievable through education, immunization, and implementation of early treatment guidelines. Effective healthcare teams who understand the value of disease prevention, and follow evidence-based practice guidelines can significantly reduce the burden of HZ and PHN, thereby, improving the quality of life for patients.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.