
Abstract
Golimumab (GLM) is a fully human monoclonal antibody with amino acid sequences of the light and heavy chains identical to those of infliximab, that binds specifically to both the soluble and transmembrane bioactive forms of human TNF-α, thereby inhibiting the biological activity of TNF. GLM was studied in an extensive program of RCTs that included one study in phase I and one in phase II, and studies in phase III including patients failing MTX (GO-FORWARD), failing other anti TNF (GO-AFTER), MTX naïve patients (GO-BEFORE), and one study with IV GLM in patients that remained active in spite of receiving MTX. These studies showed that GLM is effective and safe for the treatment of RA, with a efficacy and safety profile very similar to the other classic anti TNF biologics, and determined the approval by the FDA in April 2009 for use in moderately-to-severely active RA in combination with methotrexate (MTX) when given to adults. In comparison to other biologics for RA, GLM has some advantages: first, it's less frequent administration (every 4 weeks); and second, its subcutaneous route of administration, which allows patients to self administer the drug at home. Currently, GLM represents an option to RA active patients desiring less frequent injections and to patients in whom the previous treatment with other TNF-α inhibitors failed.
Introduction
Rheumatoid arthritis (RA) is a chronic and progressive systemic inflammatory disease, affecting 0.2% to 2% of the population worldwide.1–3 Several studies have shown that progressive and persistent inflammation can lead to joint damage, disability, and increased morbidity and mortality in patients with RA.
The concept of “window of opportunity” involves the use of early aggressive treatment in an attempt to stop the natural course of the disease.4,5
In the last years significant progress in the pathophysiology of RA has led to the identification of tumor necrosis factor α (TNF-α) as the main inflammatory mediator.6,7 The development of TNF-α inhibitors has been a significant advance in the treatment of RA and other chronic inflammatory diseases. These drugs have improved outcomes in RA, reducing morbidity and mortality. Actually there are five drugs available for the management of RA patients: Etanercept (Enbrel®), soluble dimeric p75 TNF-α receptor/ Fc fusion protein; Infliximab (Remicade®), a chimeric mouse/human anti-TNF-α monoclonal antibody (mAb); Adalimumab (Humira®), humanized anti-TNF-α mAb; Certolizumab pegol (Cimzia®), a pegylated Fab-fragment of an anti-TNF-α antibody; and Golimumab (Simponi®), a human anti-TNF-α mAb.
Golimumab was approved by the FDA in April 2009 for use in moderately-to-severely active RA in combination with methotrexate (MTX) when given to adults, and alone or in combination with MTX when used in adult patients with active Psoriatic Arthritis (PsA), and adult patients with active Ankylosing Spondylitis (AS). 8
This review will focus on Golimumab (GLM) in the management of RA.
Mechanism of Action
GLM is a human immunoglobulin (Ig) G1-kappa monoclonal antibody that binds specifically to both the soluble and transmembrane bioactive forms of human TNF-α, thereby inhibiting the biological activity of TNF. Being a fully human monoclonal antibody, GLM resembles adalimumab, but its amino acid sequences of the light and heavy chains are identical to those of infliximab. 9 It was shown that was able to modulate the biological effects of TNF in several bioassays, such as the expression of adhesion proteins responsible for leukocyte infiltration (E-selectin, ICAM-1 and VCAM-1) and the secretion of proinflammatory cytokines (IL-6, IL-8, G-CSF and GM-CSF). 9
Pharmacokinetics
The median time to reach maximum serum concentrations (Tmax) of GLM fluctuate from 2 to 6 days, both in healthy subjects and in patients with active RA following subcutaneous (SC) injection.
GLM is distributed primarily in the circulatory system with limited extravascular distribution. Median terminal half-life values were approximately 2 weeks in healthy subjects and patients with active RA.
In cross-studies comparing mean AUCinf values following an IV or SC administration of GLM, the absolute bioavailability of SC GLM was estimated to be approximately 53%.10,11 Administered SC to patients with RA every 4 weeks, GLM serum concentrations reached steady state by Week 12. Concomitant use of MTX has shown higher (52%) concentrations of GLM compared with GLM alone, and decreased anti-GLM antibody incidence from 7% to 2%.10,11 Based on this data for RA, GLM should probably be used with MTX. The concomitant use of NSAIDs, oral corticosteroids, or sulfasalazine does not appear to influence the clearance of GLM.
Pharmacokinetic (PK) analyses showed that there is no need to adjust the dosage of GLM according to patient's weight, gender, age or ethnicity. 10 No formal study on the effect of renal or hepatic impairment on the PK of GLM has been conducted. There are no studies on the effect of renal or hepatic impairment on the PK of GLM.
Pharmacodynamics
In clinical studies, decreases in C-reactive protein (CRP), interleukin (IL)-6, matrix metalloproteinase 3 (MMP-3), intercellular adhesion molecule (ICAM)-1 and vascular endothelial growth factor (VEGF) were observed following GLM administration in patients with RA, PsA, and AS. 10
Clinical Studies
GLM was studied in an extensive program of RCTs that included one study in phase I and one in phase II, and studies in phase III including patients failing MTX (GO-FORWARD), failing other anti TNF (GO-AFTER), MTX naïve patients (GO-BEFORE), and one study with IV GLM in patients that remained active in spite of receiving MTX. We would summarize these studies.
Studies Phase I
The PK properties and safety of GLM were assessed in a placebo-controlled, dose escalating Phase 1 study of subjects with RA. 11 Six different doses (0.1, 0.3, 1, 3, 6 and 10 mg/kg) given as a single intravenous (IV) infusion were studied; six subjects were included in each group. The median half-life was approximately 11–19 days in subjects who received 3 mg/kg or higher doses. Subjects were followed up for 16 weeks after the infusion of GLM. Adverse events (AE) were generally mild to moderate and headache was the only AE that appeared to correlate with the dose. 11
Studies Phase II
A Phase 2 multicenter, randomized, double-blind, placebo-controlled study was conducted to test the efficacy of GLM in 172 patients with active RA despite MTX therapy. 12 Patients received MTX and either placebo or SC GLM (50 or 100 mg) every 2 or 4 weeks (total of five study groups). The proportion of patients meeting the ACR 20% improvement criteria at week 16 was the primary study end point. At week 20, patients in the placebo group began an open-label treatment with IV infusions of infliximab (3 mg/kg), with induction at weeks 20, 22, and 28 followed by maintenance therapy every 8 weeks through week 44, and patients originally assigned to receive GLM injections every 2 weeks remained blinded but had the interval increased to every 4 weeks through week 48. 12
Results
When all GLM plus MTX dose groups were analyzed combined, 61% of patients achieved an ACR 20 response at week 16 compared with 37% of patients in the placebo plus MTX group (P < 0.010). In addition, 79% of patients in the group receiving 100 mg GLM every 2 weeks achieved an ACR 20 response (P < 0.001 vs. placebo).
Safety
Adverse events (AE) were reported by 85% of patients in the placebo group and 86% of patients in the combined GLM groups at week 20. The most common AE in the combined GLM groups were nausea, headache, injection-site erythema, and worsening of RA disease activity. Serious adverse events (SAE) were reported by 6% of patients in the placebo group and by 9% of patients in the combined GLM groups. The overall rate of infection in each one of the GLM groups was not greater than that observed in the placebo group. The safety profile of GLM during the follow up period through week 52 was similar to that during the placebo-controlled period. There were no cases of tuberculosis (TB), lymphoma or deaths. Four GLM-treated patients had malignancies (non melanoma skin and lung cancer). Of the 107 GLM-treated patients with evaluable samples, 6.5% developed antibodies to GLM.
Conclusion
After this trial it can be concluded that GLM plus MTX was able to effectively reduce signs and symptoms of RA in patients with an inadequate response to MTX.
Studies Phase III
In the first phase II study 12 no difference in efficacy could be distinguished among the four different arms studied. The dosages of 50 mg and 100 mg every four weeks were chosen for further evaluation in the phase III program. The characteristics of these studies are summarized in Table 1.
Phase III trials.
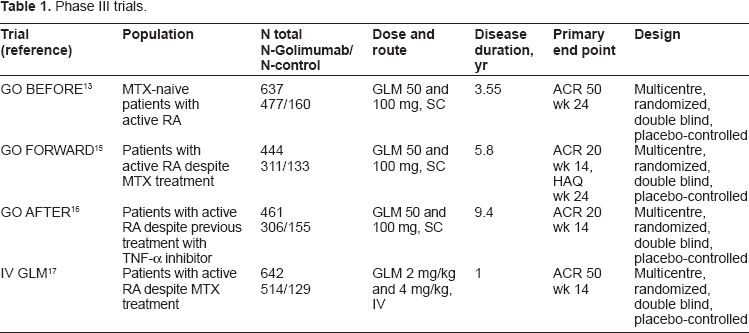
The
By intent-to-treat (ITT) analysis, the primary end point was not achieved. However, three patients never received the treatment and were excluded in a modified ITT (mITT) analysis where the primary endpoint was achieved: the proportion of patients treated with GLM 50 mg + MTX achieved a significantly greater ACR 50 response at week 24 than those treated with MTX alone. 13 GLM alone was non inferior to MTX alone. The additional benefit of adding GLM to MTX in this patient population was modest, but similar to what has been observed in previous studies of other TNF-α antagonists in patients with early RA who had not been previously treated with MTX.
Safety
The incidence of SAE and serious infections was low and similar across treatment groups, with the exception of a higher incidence of serious infections with GLM 100 mg plus MTX (4% vs. 1%–2% in the other treatments). Two patients died. One patient in group 3 was diagnosed of tuberculosis (TB) of the spine, but a review of that patient's record indicated that the spinal lesion was present prior to entering the study. Again, in this study the overall incidence of antibodies to GLM was low (6%).
Conclusion
GLM administered SC at a dosage of 50 or 100 mg every 4 weeks plus MTX reduced signs and symptoms of active RA in patients naïve of MTX or biologic anti-TNF therapy.
The
The co-primary endpoints were the proportion of patients with ACR 20 at week 14 and the change from baseline in HAQ-DI score at week 24. There was an early escape for those patients in groups 1, 2 and 3 that did not achieve at least 20% improvement in both swollen and tender joint counts at week 16.
GLM plus MTX and GLM plus placebo were compared with placebo plus MTX for the first 24 weeks of the study. 15 At this visit, all patients remaining in the placebo arm (group 1) began receiving GLM 50 mg injections in a blinded fashion. Patients in groups 2, 3 and 4 continued to receive their originally assigned treatment. Injections continued to be administered SC every 4 weeks up to week 48, with final study assessments at week 52. 14
Results
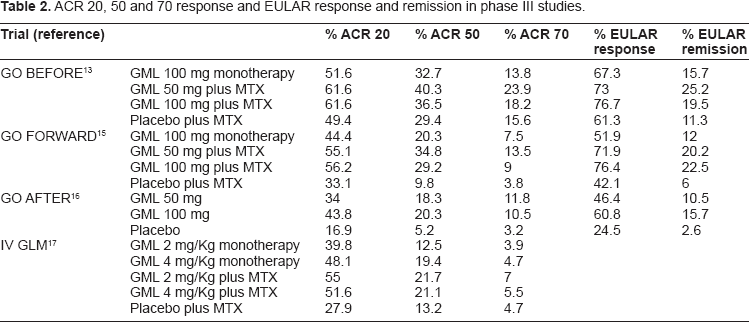
Overall, 444 patients were randomly assigned to treatment. At week 16, 41 patients (31%) in group 1, 36 patients (27%) in group 2 and 15 patients (17%) in group 3 entered early escape. Although fourteen patients (16%) in group 4 met the criteria for early escape at week 16, they continued with the same treatment according to the protocol that did not allow for predetermined escape in this group. Results are shown in Table 2. Similar percentage of patients in each group by ITT analysis achieved an ACR 20 response at week 52. 14
ACR 20, 50 and 70 response and EULAR response and remission in phase III studies.
Safety
Any AE occurred in a high percentage of patients in each group (74% group 1, 81% group 2, 79% group 3 and 86% group 4) through week 52; however, of these only 4.5%, 12%, 8% and 18% were SAE, and only 1%, 4%, 2% and 7% were serious infections, respectively. 14 TB pleuresy was reported in one patient. Patients who received the 100 mg dose of GLM with or without MTX appeared to have greater rates of SAE and serious infections compared with the other groups.
Two patients died (1 from sepsis and another because of acute hepatic failure) and malignancies (basal cell cancer, squamous cell skin cancer, breast cancer) were reported in seven patients. 14
Five of 236 patients with evaluable samples (2%) had antibodies to GLM at week 24 that did not appear to affect response as 2 of these patients (40%) achieved an ACR 20 response and one patient (20%) achieved an ACR 50 response at week 24.14,15
Conclusion
GLM 50 mg or GLM 100 mg administered every four weeks in combination with MTX in patients with active RA despite MTX therapy significantly reduced signs and symptoms of RA and improved physical function.
The
The primary end point was the proportion of patients achieving an ACR 20 response at week 14 for the combined GLM groups.
Results
All patients had been treated previously with at least one TNF-α inhibitor: 115 patients (25%) had been treated with two TNF-α inhibitors, and 43 patients (9%) had previously received all three commercially available TNF-α inhibitors. Previous TNF-α inhibitors were discontinued because of lack of effectiveness (58%) or other reasons (intolerance, accessibility issues [53%]). 16
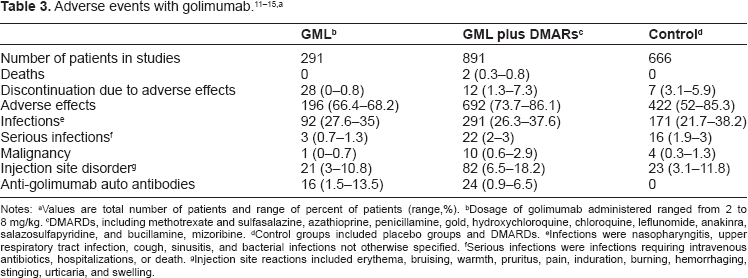
bDosage of golimumab administered ranged from 2 to 8 mg/kg.
cDMARDs, including methotrexate and sulfasalazine, azathioprine, penicillamine, gold, hydroxychloroquine, chloroquine, leflunomide, anakinra, salazosulfapyridine, and bucillamine, mizoribine.
dControl groups included placebo groups and DMARDs.
eInfections were nasopharyngitis, upper respiratory tract infection, cough, sinusitis, and bacterial infections not otherwise specified.
fSerious infections were infections requiring intravenous antibiotics, hospitalizations, or death.
gInjection site reactions included erythema, bruising, warmth, pruritus, pain, induration, burning, hemorrhaging, stinging, urticaria, and swelling.
Significantly more patients in each of the GLM-treated groups achieved ACR 20, ACR 50, ACR 70, DAS28 remission and DAS28 (EULAR) response at weeks 14 and 24 than did those on placebo 16 (Table 2). Forty six percent of patients on placebo and 27% on 50 mg GLM received rescue therapy at week 16, of whom, 22 (31%) and 10 (25%) patients, respectively, achieved ACR 20 at week 24 after GLM dose adjustment; 42 (27%) patients on 100 mg GLM met the criteria for rescue therapy at week 16, but their GLM dose was not changed, and 15 (36%) of these patients went on to achieve ACR 20 by week 24. 16
Safety
Adverse events were frequent in all groups occurring in 72% of patients in placebo group and in 74% of patients in combined GLM group; of these, only 10% and 6%, respectively, were SAE. 16 Treatment with GLM did not increase frequency of serious infections or concentration of antibodies to GLM. Three patients developed cancer (pancreatic cancer, squamous cell carcinoma of the skin and lymphoma); no patients developed TB or an opportunistic infection. Only one death occurred during the study. 16
Conclusion
This study showed that GLM reduced the signs and symptoms of RA in patients with active disease despite previous treatment with other TNF-α antagonist(s).
Intravenous GLM
An IV preparation of GLM was evaluated in a phase III, multicenter, randomized, double-blind, placebo-controlled, 48-week trial in patients in whom RA remained active despite treatment with MTX. 17 Patients were randomly assigned to receive blinded IV infusions of placebo plus MTX, 2 mg/kg GLM with or without MTX, or 4 mg/kg GLM with or without MTX, every 12 weeks. At weeks 16 and 24, the same criteria than in previous trials (patients with <20% improvement from baseline in both the swollen and tender joint counts) were used for an early escape and dose regimen adjustment in a blinded manner. Patients completing the week 48 infusion could continue receiving GLM (50-mg SC injections every 4 weeks) during an open-label 40-week extension, which began following the week 48. The primary end point was the proportion of patients meeting the ACR 50 response at week 14.
Results
Six hundred and forty three patients were randomized and treated with GLM with or without MTX (514 patients) or placebo plus MTX (129 patients). The primary study end point was not met (at week 14, an ACR 50 response was observed in 21% of the patients treated with GLM plus MTX compared with 13% of the patients treated with placebo plus MTX [P = 0.051]). However, GLM therapy was efficacious in reducing many measures of RA disease activity. All components of the ACR response score were significantly improved with GLM with or without MTX treatment compared with placebo at week 14. 17 The addition of MTX enhanced and prolonged the efficacy of IV administered GLM. By week 24, significantly more patients treated with GLM plus MTX had achieved an ACR 50 response; this difference was not evident at week 14 (16% vs. 13%) or week 24 (10% vs. 9%), suggesting a slow mechanism of synergy between both drugs. 17
Safety
As shown with SC administration, antibodies to GLM were detected in a low percentage of patients (~5% and ~7% at weeks 24 and 48, respectively). 17 Concomitant use of MTX was associated with a lower incidence of antibodies to GLM. The most commonly reported adverse event trough week 48 were infections (48% of patients treated with GLM with or without MTX and 41% of patients receiving placebo plus MTX), but only 3.7% in all GLM treated patients suffered serious infection. Two cases of TB occurred in patients who initially had negative results for TB at screening. Five deaths were reported after week 24 and were distributed fairly equally among the active arms of the trial. There was not apparent association between GLM treatment and the onset of malignancies. A small number of GLM-treated patients had elevated levels of transaminase enzymes. 17
Conclusion
The primary trial end point was not met. However, IV administered GLM plus MTX appeared to provide benefit in the long-term reduction of RA signs/symptoms in MTX-resistant patients when other outcomes were assessed. There were no unexpected safety concerns.
Radiographic Progression
Recently, Emery et al analyzed the effect of Golimumab on radiographic progression in Rheumatoid Arthritis. 18 Patients participating in the GO-BEFORE study (MTX-naïve patients n = 637) and in the GO-FORWARD study (patients with active RA despite MTX n = 444) were included in this study. Radiographic progression was a co-primary endpoint in the GO-BEFORE study and a secondary endpoint in the GO-FORWARD study (the GO-AFTER study did not include radiographic evaluations). Radiographs of the hands and feet were taken at baseline, week 28, and week 52 in GO-BEFORE and at baseline, week 24 (week 16 for patients who entered early escape), and week 52 in GO-FORWARD. Radiographs were scored by two independent readers in each study using the van der Heijde modification of the Sharp score.
Results
At baseline, approximately 96% to 97% of patients in GO-BEFORE and approximately 87% to 92% of patients in GO-FORWARD had a modified Sharp score > 0; median modified Sharp scores were greater in GO-FORWARD than in GO-BEFORE, which was expected for a patient population with a longer disease duration. The co-primary endpoint in the GO-BEFORE study was met. Patients in GLM 50 mg plus MTX (group 3), or GLM 100 mg plus MTX (group 4) groups had significantly less radiographic progression than patients in placebo plus MTX (group 1) group over the 52 weeks. 18 GO-BEFORE subgroup analyses were consistent with the primary endpoint results. One hundred ninety three patients had established RA with disease duration > 3 years. Among these patients, those in the combined groups 3 and 4 had significantly less change from baseline to week 52 in modified Sharp score compared with those in group 1 (P = 0.029). In another subgroup analysis, mean changes in the modified Sharp score from baseline to week 52 were larger, indicating more radiographic progression in patients with screening CRP ≥ 1.5 mg/dL than in patients with screening CRP < 1.5 mg/dL. The GO-BEFORE study demonstrated that GLM in combination with MTX inhibited radiographic progression significantly better than MTX alone. 18 The difference in radiographic progression between the GLM monotherapy group and MTX alone, however, was not statistically significant. Overall, the benefits of the combination of GLM plus MTX were comparable for the 50 mg and 100 mg dose groups. In the GO-FORWARD study, minimal radiographic progression was observed in all treatment groups, and no statistically significant differences were observed between the placebo plus MTX group and the GLM groups with or without MTX. 18 Patients in groups 1 (placebo plus MTX) and group 3 (GLM 50 mg plus MTX) with screening CRP levels ≥ 1.5 mg/dL showed slightly more radiographic progression at week 24 than did those with screening CRP levels < 1.5 mg/dL. Patients in the GO-FORWARD study had more radiographic damage at baseline compared with those in the GO-BEFORE study. 18 However, patients in GO-BEFORE had higher baseline CRP levels and greater radiographic progression during the study than those in GO-FORWARD, despite having lower baseline radiographic damage. Thus, GLM effectively inhibited radiographic progression in patients with more established RA when they had higher disease activity and more radiographic progression. In conclusion, minimal radiographic progression was observed in all treatment arms of the GO-FORWARD study, which precluded the adequate assessment of the effect of GLM on radiographic progression in patients with established disease. Results of the GO-BEFORE study showed that GLM plus MTX inhibited radiographic progression not only in patients with early RA, but also in a subset of patients with more established disease (.3 years). 18
Patient Preference
In comparison to other biologics for RA, GLM has some advantages: first, its less frequent administration (every 4 weeks) compared to the other SC biologics (etanercept administered weekly, adalimumab every 2 weeks, and anakinra every day; and second, its subcutaneous route of administration, which allows patients to self administer the drug at home, compared to infliximab, abatacept, and rituximab, which requires special infusion units for IV administration, and are personal dependent and time consuming.
There are few studies assessing patients’ preferences in biologic therapies, and none specifically looking at GLM. Scarpato et al used a questionnaire to identify the determinants of anti-TNF-naive patients’ preferences for the route of administration of anti-TNF agents. 19 After assessing 802 patients with RA, they found that intravenous and subcutaneous (s.c.) routes of administration were preferred by 50.2 and 49.8%, respectively. 19 Patients dissatisfied with current therapy due to side effects preferred s.c. administration (P¼0.029), whereas patients choosing the i.v. route had slightly higher scores on ‘today pain’ (P = 0.047) and ‘articular pain’ (P = 0.023) of the Rheumatoid Arthritis Disease Activity Index (RADAI). 19
We recently studied patient preferences for biologic agents in RA using a discrete choice experiment. 20 Attributes importance ranking was in the following order: cost, systemic adverse events, frequency of administration, efficacy, route of administration, local adverse events and serious infection. Oral route of administration was preferred, but there was no difference between s.c. and iv routes. 20
There still much more that needs to be studied relate to patients’ preferences.
Place in Therapy
Although GLM was not tested against other TNF-α inhibitors in controlled trials, its efficacy is unlikely to be superior to other available TNF-α inhibitors. Currently, GLM represents an option to RA active patients desiring less frequent injections and preferring subcutaneous route of administration, and to patients in whom the previous treatment with other TNF-α inhibitors failed. It might also be an option for patients without response to another monoclonal antibody, such as adalimumab, due to the development of anti adalimumab antibodies. 21 These patients are expected to respond to a switch in the TNF inhibitor and GLM would probably be one of the less immunogenic options available.
Conclusion
GLM is a human immunoglobulin (Ig) G1-kappa monoclonal antibody that binds specifically to both the soluble and transmembrane bioactive forms of human TNF-α, thereby inhibiting the biological activity of TNF. Although still more controlled trials are needed for comparison between GLM and other DMARDs (non MTX), between GLM and other biologics, and more time is needed to appreciate longer-term safety data, to date, GLM exhibits a favorable safety profile, which is quite similar to the other TNF-α inhibitors on the market. Combined with MTX, GLM seems to be a new treatment option to RA patients with active disease who did not respond to MTX or other anti-TNF α biologics.
Disclosures
Author(s) have provided signed confirmations to the-publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.