
Abstract
The ERBB2 or HER2 receptor is overexpressed in 25% of breast cancers and is associated with poor prognosis. Trastuzumab, a monoclonal antibody targeting HER2 has been demonstrated to improve survival when combined with chemotherapy for the treatment of HER2 overexpressing metastatic breast cancer (MBC). Further studies have endeavoured to clarify the optimum chemotherapy regimen in combination with trastuzumab for MBC and its use together with novel biological agents. This review summarises these data together with preclinical studies exploring the mechanism of trastuzumab action and causes of drug resistance. The frequent incidence of brain metastases in patients on trastuzumab is highlighted, and data on the continuation of trastuzumab following CNS and non-CNS progression reviewed.
Search Strategy
We searched Pubmed using the search terms ‘trastuzumab’ ‘metastatic breast cancer’ and ‘HER2’ to identify manuscripts relevant to this review. Further references were obtained from citations therein. We also searched the abstracts of recent meetings of the American Society of Clinical Oncology with the above strategies.
Background-HER2
Identification
The ERBB family includes four transmembrane tyrosine kinase receptors ERBB1-4 (also known as HER1-4), and 13 extracellular ligands. 1 Binding of ligand, or in some cases, overexpression of receptor, results information of receptor homo and heterodimers and activation of intracellular signalling through the Ras-Raf-ERK and PI3K-AKT pathways. These signals in general act to promote cell division, cell growth and inhibit apoptosis, amongst other effects. Given the key roles of the ERBB family and their downstream mediators in development and physiology it is unsurprising that these proteins are normally subject to tight regulation.
HER2 and its overexpression
The ERBB2 or HER2 receptor was identified over two decades ago as a cell surface receptor tyrosine kinase (RTK) with similarity to both ERBB1 (EGFR) and the avian erythroblastosis virus (AEV) transforming gene, v-erbB. 2 Unlike the other ERBB receptors, exists in a primed open conformation thatHER2 exists in a primed open conformation that permits formation of homo and heterodimers with consequent activation in the absence of ligand.3,4 Amplification of HER2 with consequent overexpression of the receptor occurs in approximately 25% of human breast cancers when quantified by fluorescence in-situ hybridization (FISH) or immunohistochemical staining (IHC).5,6 HER2 overexpression can induce formation of active HER2 homodimers 7 and has been validated as tumorigenic both in-vitro8–10 and in animal models. 11
HER2 overexpression in breast carcinoma is associated with poor prognosis5,12,13 and predicts decreased response to hormonal therapy14–17 and CMF chemotherapy 18 although it is associated with sensitivity to anthracycline-containing regimens.19–22
Trastuzumab-Preclinical Development
The overexpression of HER2 in breast carcinoma relative to normal tissue made HER2 an attractive target and a number of monoclonal antibodies against the receptor were developed in the 1980s and 1990s. These were demonstrated to inhibit tumour growth of murine xenografts both alone23,24 and in combination with doxorubicin, 25 cisplatin,25,26 paclitaxel 27 and other agents. 28 In order to circumvent the problem of formation of human anti-mouse antibodies (a limiting factor in the use of monoclonal antibodies) a humanised version of the most promising of these agents29,30 was made by fusing its antigen-binding loops to human variable framework and IgG constant domain. 31 This modification was demonstrated to enhance the ability of this antibody, known initially as humAb4D5-8, later trastuzumab, to promote antibody-dependent cell-mediated cytotoxicity (ADCC). 31
Trastuzumab-Mechanism of Action
The exact mechanism of action of trastuzumab remains unclear. However evidence exists to support a role for a number of non-mutually exclusive mechanisms.
Inhibition of HER2 dimerization
Structural investigations have demonstrated that trastuzumab binds HER2 at the juxtamembrane region, an interaction that may result in a steric barrier to receptor dimerization and thus, activation. 3
Antibody dependent cell-mediated cytotoxicity (ADCC)
The basic principle of ADCC involves recruitment of immune cells (especially natural killer (NK) cells) through Fc gamma receptors to an antibody bound to a cellular antigen. Following this, cytoplasmic granules are released, resulting in lysis of the target cell. Initial in-vitro evidence suggested that ADCC was induced by trastuzumab,31,32 and strong in-vivo evidence in support of this as a mechanism of drug effect was provided by the fact that mice deficient in cell-activating Fc gamma receptors on effector cells do not have a tumor response to trastuzumab. 33 Human studies have demonstrated the presence of a tumor lymphoid infiltrate following trastuzumab administration (Gennari, Menard et al 2004; Arnould, Gelly et al 2006) the extent of which correlated with response. 34
Downregulation of HER2
Some in-vitro studies have indicated that trastuzumab induces a downregulation of HER2 with a consequent decreased in PI3K-AKT signalling,23,35 although it is unclear whether this happens in-vivo. 34
Inhibition of HER2 shedding
When overexpressed, HER2 undergoes proteolytic cleavage resulting in the release of the extracellular domain leaving a truncated membrane-bound 95 kDa fragment 36 capable of signalling. Inhibition of HER2 ectodomain cleavage by trastuzumab may prevent this. 37
Membrane recruitment of PTEN
PTEN is a key negative regulator of the PI3K-AKT pathway, and mediates its action by dephosphorylation of phosphoinositides at the plasma membrane. PTEN is itself regulated by phosphorylation and HER2 signalling via Src was shown to result in a decrease of PTEN activity secondary to tyrosine phosphorylation. Trastuzumab has been demonstrated to prevent this inactivation and the resultant decrease in AKT activity would be predicted to limit its pro-growth and survival effects. 38
Inhibition of angiogenesis
Trastuzumab has been shown to reduce levels the key pro-angiogenic growth factor vascular endothelial growth factor (VEGF) 39 and its administration results in the normalization and regression of vasculature in HER2 overexpressing xenografts in mice through multiple mechanisms. 40
Inhibition of DNA repair
Given the efficacy of trastuzumab in combination with platinum salts as described below, it is interesting to note that it has been shown to block DNA repair induced by cisplatin. 41
Trastuzumab-Pharmacokinetics and Dose
Preclinical
Initial dose definition using the murine monoclonal mumAb4D5 demonstrated maximal tumor inhibition at concentrations of 1-23 μg/ml, and subsequent work defined a trough dose of 20 μg/ml as efficacious. As comparable results were anticipated for the humanized variant, trastuzumab, a serum trough concentration of 10-20 μg/ml was targeted in initial clinical studies.
Clinical-monotherapy
The initial phase II study of trastuzumab monotherapy treated 46 patients with metastatic breast cancer (MBC) overexpressing HER2. Trastuzumab was given by a weekly schedule, with a 250 mg loading dose followed by 100 mg each week, with aim of obtaining a trough dose of 10 μg/ml. Based on an assumption that trastuzumab had dose-related nonlinear pharmacokinetics, the mean serum half-life was calculated as 8.3 days. Adequate pharmacokinetics were obtained in 90% of patients. 42 A second phase II monotherapy study used a loading dose of 4 mg/kg with subsequent weekly dose of 2 mg/kg. The mean steady state concentration of trastuzumab was shown to be 59.7 μg/ml, with mean peak 100.3 μg/ml, and trough 25 μg/ml. Half-life was estimated at 6.2 days. 43 A third study investigated the effect of doubling of the dose to 8 mg/kg loading followed by 4 mg/kg weekly but found no difference in response rate. 44 Subsequent data have demonstrated that the half-life values calculated in these initial studies were a significant underestimation as they used a one compartment model and did not take into account the accumulation of trastuzumab that occurs with multiple doses. The revised half life using a two compartment model on data collected from 476 patients was 28.5 days, raising the possibility that a less frequent schedule than weekly would not result in detrimental outcome. 45 This was confirmed in a multinational phase II study which used a loading dose of 8 mg/kg followed by 6 mg/kg every 3 weeks for previously untreated MBC. Average drug exposure was equivalent to that seen in the pivotal weekly schedule and a similar response rate was observed (discussed further below). 46 In the absence of randomized evidence to indicate superiority of one over the other, both the weekly and 3 weekly schedules have been used in trials and in the clinic off-study.
Clinical-combination therapy
The non-overlapping toxicity profile of trastuzumab with most cytotoxic chemotherapy agents means that studies have employed it at the weekly or 3-weekly doses described above when used in combination. Trastuzumab pharmacokinetics do not appear to be affected by the concurrent administration of anthracyclines, cyclophosphamide or paclitaxel. 45
Trastuzumab for MBC-Clinical Experience
Monotherapy
The initial phase II studies of trastuzumab as monotherapy in MBC have been outlined above with regards to pharmacokinetics, and are detailed further in Table 1. All studies recruited women with MBC classified as HER2 positive 2+ or 3+ on IHC.
Studies of trastuzumab as monotherapy for MBC.
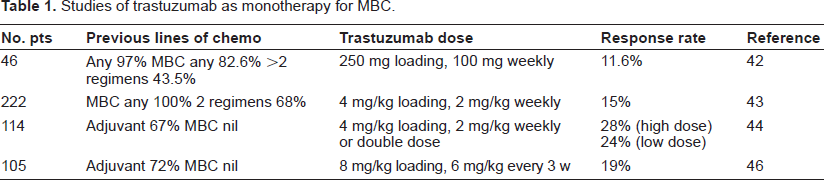
These studies comprised patients that had been largely previously treated with cytotoxic chemotherapy, in some cases extensively so including high-dose chemotherapy. As such the response rates demonstrated were encouraging, and provided clear evidence for the incorporation of trastuzumab into combination regimens for MBC. It is noteworthy that these trials included a significant number of patients with only HER2 2+ disease, a group subsequently shown to derive limited benefit from trastuzumab in the absence of gene amplification as discussed below.
In combination with chemotherapy
Chemotherapy with trastuzumab vs. chemotherapy alone- randomised evidence
The two randomised studies comparing chemotherapy plus trastuzumab with chemotherapy alone for HER2 overexpressing MBC are shown in Table 2. The pivotal phase III trial that led to FDA approval was conducted by Slamon and co-workers and published in 2001. In it 469 women with previously untreated MBC with HER2 overexpression scored as 2+ or 3+ by IHC were randomised to chemotherapy with or without the addition of trastuzumab. The chemotherapeutic regimen used depended on prior treatment; patients who had not previously received an anthracycline were treated with AC (doxorubicin 60 mg/m2 or epirubicin 75 mg/m2 plus cyclophosphamide 600 mg/m2, every 3 weeks) with or without trastuzumab (4 mg/kg loading dose, then 2 mg/kg weekly thereafter) while anthracycline pre-treated patients received paclitaxel (175 mg/m2 every 3 weeks) as single agent or combined with trastuzumab. Analysis confirmed the superiority of trastuzumab containing arms, with longer time to progression (7.4 vs 4.6 months, p < 0.001), higher response rate (50 vs 32%, p < 0.001), lower rate of death at 1 year (22 vs 33%, p = 0.008) and longer median survival (25.1 vs 20.3 months, p = 0.046). 47 In light of the fact that patients in the non-trastuzumab arms were allowed to crossover to trastuzumab at disease progression these survival data provide strong rationale for the incorporation of trastuzumab into front line therapy for HER2 overexpressing MBC.
Randomised studies of trastuzumab plus chemotherapy with chemotherapy alone for first-line therapy of MBC.
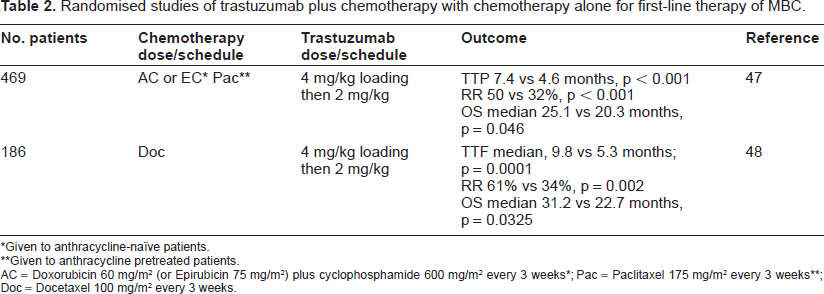
Given to anthracycline-naïve patients.
Given to anthracycline pretreated patients.
AC = Doxorubicin 60 mg/m2 (or Epirubicin 75 mg/m2) plus cyclophosphamide 600 mg/m2 every 3 weeks*; Pac = Paclitaxel 175 mg/m2 every 3 weeks**; Doc = Docetaxel 100 mg/m2 every 3 weeks.
The second, a randomized phase II, compared treatment with docetaxel (100 mg/m2 every 3 weeks) alone with the same regimen with addition of trastuzumab (4 mg/kg loading dose, then 2 mg/kg weekly). The study comprised 186 women with previously untreated MBC with overexpression of HER2 (initially defined as 2+ and 3+ on IHC, though this was subsequently restricted to 3+ only after initial data defined responders; 94% of the final study population had disease 3+ on IHC or FISH positive). Again, combination therapy was superior in terms of response rate (61% vs 34%, p = 0.002), time to treatment failure (median, 9.8 vs 5.3 months; p = 0.0001) and median overall survival (31.2 vs 22.7 months, p = 0.0325). 48 As in the Slamon trial patients in the control arm were permitted to crossover to trastuzumab at progression; in the 57% who did median survival was 30.3 months compared to 16.6 months in those who did not 48 –-though these results should be treated with caution given the obvious potential confounders. Combination therapy resulted in higher incidence rates of G3/4 neutropenia (32 vs 22%) and febrile neutropenia (23 vs 17%). 11% of patients in the combination arm developed a decrease in left ventricular ejection fraction (LVEF) >15% vs 6% in the docetaxel alone arm.
Optimal chemotherapy in combination with trastuzumab- randomized evidence
The addition of carboplatin to paclitaxel/ trastuzumab was investigated in a phase III trial comprising 196 patients with MBC who had not received chemotherapy for metastatic disease (roughly half in each group had been treated with adjuvant chemotherapy). The experimental group were treated with TCH (paclitaxel 175 mg/m2, carboplatin AUC6 every 3 weeks, trastuzumab 4 mg/k loading followed by 2 mg/kg weekly) and the control group received the same with omission of paclitaxel. There was an advantage for the experimental arm for response rate (52% vs 36%, p = 0.04), progression-free survival (13.8 vs 7.6 months, p = 0.03), with a trend towards improved overall survival at 4 years (38% vs 31%, p = NS). Grade 3/4 neutropenia was worse in the three drug arm (36 vs 12%, p = 0.0001) and the rate of febrile neutropenia was also increased (3% vs 1%). Thus, the authors reasonably concluded that TCH represents a useful treatment option in HER2 overexpressing MBC. 49 Interestingly however, a second randomised phase III study that substituted docetaxel for paclitaxel; (docetaxel 75 mg/m2, carboplatin AUC6, trastuzumab 8 mg/kg loading then 6 mg/kg every 3 weeks vs docetaxel 100 mg/m2 every 3 weeks, identical trastuzumab dose/schedule) failed to show a difference in response rate (72.5% both groups), duration of response (9.4 vs 10.7 months) and time to progression (10.4 vs 11.1 months, p = 0.57). 50 The reasons for this are not clear but may relate to the lower taxane dose in the 3 drug arm.
A randomized comparison between taxane (docetaxel or paclitaxel at investigator's choice) and vinorelbine in combination with trastuzumab for untreated MBC was attempted, unfortunately the study recruited poorly, and was closed early with no significant differences seen between arms. 51
Chemotherapy plus trastuzumab-non-randomized evidence
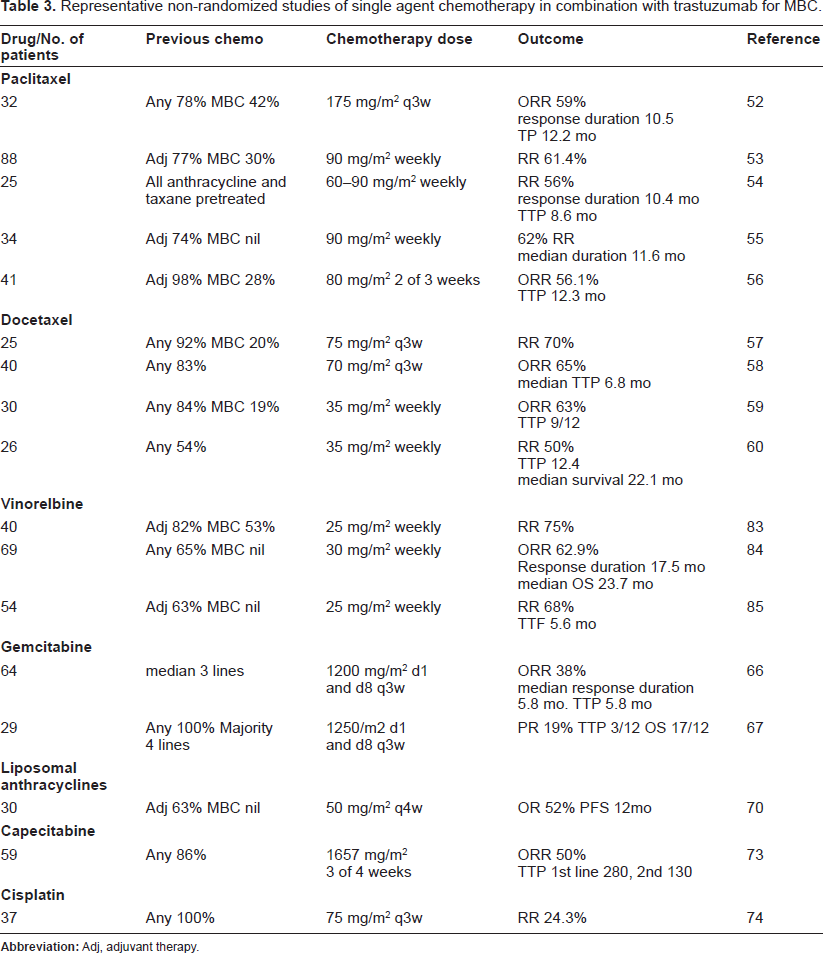
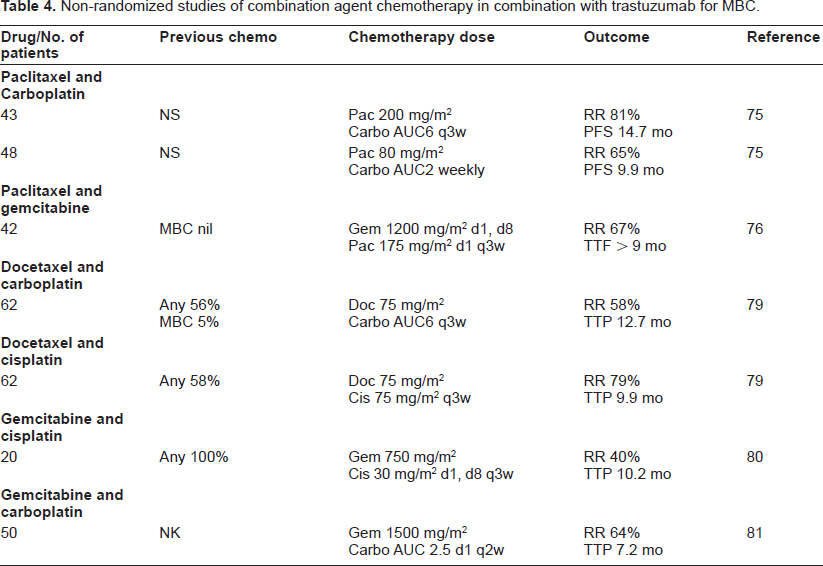
A large number of non-randomized phase II studies of trastuzumab in combination with single agent cytotoxic chemotherapy have been published and presented in abstract form. Response rates vary between studies according to levels of HER2 expression in tumors, patient characteristics and pretreatment but for commonly used chemotherapeutic agents combined with trastuzumab are as follows; paclitaxel 56%-62%,52–56 docetaxel 50%-70%, vinorelbine 43%-78%,61–65 gemcitabine 19%-38%,66,67 liposomal anthracyclines 46%-68%,68–71 capecitabine 45%-50%,72,73 and cisplatin 24.3%. 74 Toxicities are generally as expected for each drug, with the addition of trastuzumab-related cardiotoxicity (discussed below). In the absence of clear evidence for superiority of one agent over another, it would seem reasonable to base treatment decisions upon which agents a patient has already received, and the likely side effects of the intended drug. A number of combination chemotherapy regimens with trastuzumab have also been studied, a selection of which are summarised in Table 4. Response rates are as follows; paclitaxel and carboplatin: 65%-81%, 75 paclitaxel and gemcitabine: 53%-67%,76,77 paclitaxel and doxorubicin: 88%, 78 docetaxel and carboplatin: 58%, 79 docetaxel and cisplatin: 79%, 79 gemcitabine and cisplatin: 40%, 80 gemcitabine and carboplatin: 64%, 81 gemcitabine and vinorelbine: 50%. 82 The gain in response rate offered by combination therapy is at cost of greater toxicity; whether to elect for combination therapy vs single agent again depends on patient factors and must be made on an individual basis.
Representative non-randomized studies of single agent chemotherapy in combination with trastuzumab for MBC.
Trastuzumab in combination with other biologic therapies
Lapatinib is a small molecule dual inhibitor of the EGFR and HER2 receptors tyrosine kinase activity 86 that demonstrated preclinical synergy with trastuzumab.87,88 The combination was tested in a phase I study of 53 patients with heavily pretreated advanced or MBC (median no. of prior chemotherapy regimens 4, 92% previously treated with trastuzumab). Lapatinib was given at dose of 750-1500 mg/day, trastuzumab according to the standard weekly schedule. The response rate was an encouraging 22%, indicating that this regimen merits further investigation. 89 Another molecule with preclinical evidence of synergy with trastuzumab is pertuzumab; a antibody against a different region of HER2 and able to prevent dimerisation with HER3. 90 The two were combined in a phase I study and demonstrated a response rate of 18%, however cardiotoxicity was significant, and this requires further investigation before an informed decision about the risks and benefits of treatment can be reached. 91 The need for caution when extrapolating from preclinical evidence is exemplified by gefitinib however, a small molecule inhibitor of EGFR that demonstrated promising synergy with trastuzumab in xenograft assays.92,93 On this basis a phase I/II study was undertaken, however this closed at the first interim analysis due to low activity of the combination (RR 9%). 94 Other novel agents that have been combined with trastuzumab in early phase trials include celecoxib (no responses seen in a phase II study) 95 and the heat shock protein HSP90 inhibitor tansepimycin. 96
Monitoring Response to Trastuzumab-Serum Shed HER2
Cleavage of the HER2 receptor results in shedding of the extracellular domain (ECD) into the circulation, elevated levels of which predict resistance to hormonal and some chemotherapies. 97 Decline in the levels of circulating HER2 ECD with trastuzumab treatment has been shown to predict response59,98 and longer time to disease progression. 99
Continuation of Trastuzumab beyond Progression
Non-CNS disease
The favourable toxicity profile of trastuzumab when given as extended therapy 100 together with the evidence for its synergy with cytotoxic chemotherapy has led many oncologists to continue the drug beyond progression with addition of other agents. 101 A number of retrospective studies have shown that patients who continue trastuzumab may have responses to additional therapies102–105 and some have also suggested improved survival in such patients106,107–-a finding also demonstrated in a prospective cohort study. 108 However these results are not universal 109 and the lack of a control group together with potential for selection bias in these studies makes means that it is not possible to reach firm conclusions regarding the efficacy of this approach. More conclusive evidence in favour of continuation of trastuzumab was recently provided by a German study that randomised 156 patients with MBC and disease progression on trastuzumab to either capecitabine alone (2500 mg/m2 d1-d14 every 3 weeks) or combined with trastuzumab (standard 3 weekly schedule). Continued trastuzumab was associated with significantly improved response rate (48 vs 27%, p = 0.01), time to progression (8.2 vs 5.6 mo, p = 0.03) and a non-significant extension of survival (25.5 vs 20.4 p = NS). It is unfortunate that these data will not be added to by a randomized trial of vinorelbine alone or vinorelbine with continued trastuzumab after progression on taxane/trastuzumab combination, as this trial was discontinued due to poor recruitment.110,111
Non-randomized studies of combination agent chemotherapy in combination with trastuzumab for MBC.
Patients with disease progressing on trastuzumab have been shown to benefit from inclusion of Lapatinib in combination with further lines of systemic chemotherapy. 112 This approach has not been compared to continuation of trastuzumab in combination with the same chemotherapy and so the optimal management of HER2 positive disease beyond first progression is not yet defined.
Clearly, the decision to continue trastuzumab after disease progression must be taken on an individual basis, and should take into account patient, treatment, and ultimately economic factors.
CNS disease
A notable finding reported by a number of retrospective studies is the high incidence of brain metastases in patients treated with trastuzumab for MBC; 25 to 48.1% of patients113–120 compared with around 5% in historical series.121,122 The possible explanations for this include the extension of disease course trastuzumab provides, the inability of trastuzumab to cross the intact blood-brain barrier (BBB) and an a predilection of HER2 overexpressing breast cancer to spread to the CNS.113–115,119 It should be noted, however, that there there is some disagreement in the literature on this subject 116 (see Melisko for a recent review). 123 Irrespective of this, a common situation encountered is the development of CNS metastases while extracranial disease is responding or stable.113–115,119 An increasing body of evidence exists to suggest that continuation of trastuzumab after development of brain metastases in such patients is associated with favourable prognosis.114–116,118,124–127 Whether this is due to control of non-CNS disease or penetration of trastuzumab into the CNS via aberrant tumour vasculature is unclear, however it is reasonable to conclude that in patients with responding disease, the diagnosis of CNS metastases should not automatically result in cessation of trastuzumab therapy.
Trastuzumab-Toxicities
The principal toxicities of trastuzumab are acute infusion-related and cardiac. Early studies of monotherapy defined infusion-related chills (40% with initial dose, <3% recurrent), asthenia (23%), rash (20%), nausea (25%) and diarrhea (36%) as the most frequent side-effects;43,44 however cardiotoxicity was not clearly apparent until the phase III trial conducted by Slamon. In this cardiotoxic effects occurred in 27% of patients treated with concurrent trastuzumab and anthracyclines, 13% with trastuzumab and paclitaxel, and 5% of those with monotherapy. 47 This is manifest as a symptomatic, or asymptomatic decline in left ventricular ejection fraction at frequency of 0%-3% and 0%-20% respectively, depending on drug.48,49,53,59,85,128 Risk factors for its cardiotoxicity include current or previous anthracycline, advanced age 129 and low baseline LVEF. 130
Trastuzumab-induced decline in LVEF appears more reversible than that caused by anthracyclines, and generally improves with medical management, 131 indeed, in one study 88% of patients rechallenged with trastuzumab did not demonstrate recurrent cardiotoxicity. 132 Guidelines to minimise risk vary, but one published set (though designed for adjuvant therapy) advises avoidance of trastuzumab if baseline LVEF is ≥55% and 3 monthly echocardiography in patients on treatment, with consideration given to cessation if LVEF drops by > 10% or to <50%. 133 The decision on continuation of trastuzumab in patients with decline in LVEF and responding metastatic disease is a difficult one, and requires careful thought and discussion with the patient.
When to Initiate Trastuzumab
The decision of when to initiate trastuzumab treatment in patients with MBC is an individual one. Early use of chemotherapy with trastuzumab should be considered for patients with by estrogen receptor (ER) negative disease, visceral metastases, and a disease free interval of less than 2 years. As discussed above, upfront use of trastuzumab in the pivotal trial was associated with a five month improvement in median survival despite the subsequent crossover of patients in the control arm. 47 Patients with less aggressive disease keen to avoid the toxicities of chemotherapy are candidates for trastuzumab monotherapy, although this approach may be inferior to upfront combination treatment. 134
HER2 Testing
Benefit from trastuzumab is confined to patients with HER2 overexpression, 135 and analysis of early trials suggested that the drug is most active in pts with staining classified as 3+ on IHC or with gene copy no >2.0 on FISH. 44 Although there is good correlation between the two, 136 a common approach is to test with IHC and perform FISH on tumors that are 2+. 137
Resistance
The study of mechanisms of trastuzumab resistance and strategies to overcome this has been the subject of much research. Unlike other monoclonal antibodies, anti-trastuzumab antibodies do not occur with any significant frequency (0%-0.5%).43,44 One factor that has been associated with resistance is loss of the PTEN tumor suppressor. As stated above, this is a key negative regulator of the PI3K pathway through which HER2 signals. Trastuzumab-resistant cells often have low PTEN levels, 138 and in an elegant siRNA screen it was demonstrated that PTEN knockdown induced trastuzumab resistance in cells in-vitro. The same study showed that patients treated with trastuzumab who had activation of the PI3K pathway either through PTEN loss or through gain of function mutations in PIK3CA (the gene encoding the catalytic subunit of PI3K) had reduced progression-free survival. 139 Other work has shown that the response rate to taxane/trastuzumab combination therapy in patients with tumors lacking PTEN is significantly lower than in patients with normal levels of protein 11.1% vs 66.7%, a difference that was not seen in patients treated with taxane alone. 140 However, prospective studies are required to confirm these results before they can be used for clinical decision making.
A second mediator of resistance may be the type I insulin-like growth factor receptor (IGF-IR). IGF-IR expression in breast cancer cells in vitro causes trastuzumab resistance, 141 possibly through formation of IGF-IR/HER2 heterodimers, 142 and use of combination anti-IGF-IR therapy with trastuzumab had synergistic effects in breast cancer lines expressing IGF1R in vitro. 143 In one study of neoadjuvant trastuzumab with vinorelbine increased IGF-IR expression was associated with decreased response rate, 144 however another study found no link between expression and response rate to trastuzumab therapy in MBC. 145
Other factors implicated in trastuzumab resistance include decreased expression of the cell cycle regulator p27, 146 increased levels of the hepatocyte growth factor (HGF) receptor Met,144,147 increased phosphorylated EGFR 148 and elevated levels of the growth factors IGF-I, HGF and pleotrophin. 144
Conclusions and Future Directions
The development of trastuzumab is undoubtedly one of the major advances in medical oncology in the last 20 years. In addition, its use in HER2 overexpressing MBC provides proof of principle of an important advance in therapy; the targeting of novel agents to subgroups of patients with genetically defined tumor characteristics. Ongoing work will clarify the use of trastuzumab for MBC in the increasing number of patients who have already received the drug as adjuvant therapy, together with its use in combination with the many new agents entering the clinic.
Conflict of Interests
DNC and CGAP have received honoraria and travel expenses from Roche. No conflict of interest declared.