
Abstract
Objective
The present study aimed to determine the time course of aminoglycoside-induced serum creatinine (SCr) elevation and compare that in patients treated with amikacin (AK) and those treated with gentamicin (GM).
Methodology
A one-year, non-interventional prospective study of patients with normal baseline renal function and were administered either GM or AK. The study was carried out at the internal medicine department of Al-Watani governmental hospital. Outcome of interest was the time course of serum creatinine elevation during the course of aminoglycoside therapy. Data were entered and analyzed using Statistical Package for Social Sciences (SPSS 16).
Results
The study was performed in 94 patients, who had to be administered GM or AK by intravenous injections. In both groups, the significant rise in SCr was detected on the 4th day of therapy. However, GM induced up to 32% increase while AK induced up to 19.5% increase in SCr from baseline levels. In the course of AK treatment, patients on single dosing frequency and those <65 years of age did not show a significant increase in SCr levels during the 6-day therapy. In the course of GM therapy, patients on single frequency dosing, younger patients and females showed a significant elevation in SCr on the 5th day while elderly, males and those on multiple dosing showed a significant elevation on the 4th day of therapy. However, all patient categories on GM therapy showed similar extent of SCr elevation.
Conclusion
In patients with normal renal function, GM and AK showed similar time course but different extent of SCr elevation. Amikacin induced no SCr elevation when given in single dosing frequency or when given to younger patients. Such effects were not observed with GM.
Introduction
Aminoglycosides, like amikacin (AK) and gentamicin (GM) have been widely used in clinical situations because of their efficacy and low cost. However, aminoglycosides present a serious drug induced nephrotoxicity which is linked to their accumulation in renal cortex and their capacity to bind the phospholipids and to induce intracellular lesions.1–4 Evidence suggests that aminoglycoside-induced nephrotoxicity occurs after a few days of therapy. Patients treated with aminoglycosides for 4 consecutive days preceding nephrectomy showed that GM had significant tissue accumulation, lysosomal overloading, and loss of lysosomal phospholipase A1 while AK induced significantly lower lysosomal overloading and no loss of phospholipase A1 activity. 5 Several animal studies confirmed that AK produced less nephrotoxicity than GM.6–8 However, in the clinical settings, the time course and capacity of aminoglycoside to evoke nephrotoxic effects may be influenced by variables including duration of drug administration, its dose, original status of renal function, frequency of administration, coexisting diseases and drugs administered in parallel and gender of the patient.9–11 Several studies investigated and compared the nephrotoxicity of GM and AK in the clinical settings and reached different conclusions.12–14 However, we previously reported that in patients with initial normal renal function, GM was significantly more nephrotoxic than AK and that multiple dosing of GM was more nephrotoxic than single dosing. However, AK induced nephrotoxicity was not significantly dependent on dosing frequency. 15 We also reported that gender differences in aminoglycoside induced nephrotoxicty were seen with AK where females were more vulnerable to nephrotoxicity and that such gender differences did not exist with GM. 16 Furthermore, in most of these published studies including our previously published reports, the time course of SCr elevation and factors affecting such time course were not fully investigated. Therefore, the aims of the present study were to determine the time course of aminoglycoside-induced elevation of SCr in hospitalized patients with normal baseline renal function and to compare the time course of SCr elevation between patients treated with GM and those treated with AK.
Patients and Methods
The study was conducted at Al-Watani hospital, a 100-bed facility located in Nablus city, Palestine. The hospital is a governmental referral hospital that serves the general population in northern Palestine. The hospital includes all major medical departments. However, there is no specific infectious unit in the hospital and patients with suspected infections are treated in the internal medicine department. The aminoglycosides are commonly used in the hospital as an empiric therapy and in infections caused by Gramnegative bacilli, e.g. intra-abdominal, urinary tract, and most nosocomial infections.
Study design
This is a non-interventional prospective study of all patients receiving aminoglycoside treatment, particularly amikacin (AK) or gentamicin (GM), in the internal medicine department during a 12-month period. The study took place between September 01, 2006 and August 31, 2007 and was approved by medical ethics committee and the health authorities.
Study population
The screened patients were those hospitalized due to infections, mainly infections of respiratory tract, abdomen and urinary tract that had to be treated with antibiotics of aminoglycoside group by intravascular route.
Selection criteria
Inclusion criteria for this study were: patients with initial serum creatinine level ≤1.2 mg/dL, administration of AK or GM for not less than six days, availability of serum creatinine levels obtained before initiation of the treatment and during therapy up until the sixth day of the study and finally, had no AK or GM in the previous month.
Data extraction
Demographic, clinical, laboratory and medications administered were obtained from the patients’ medical charts. Information collected at baseline included age, gender, previous hospitalization or aminoglyside use, presence of other factors predisposing to renal disease (such as diabetes mellitus, hypertension, peripheral vascular disease, congestive heart failure). Dose and frequency of aminoglycosides administration were obtained from patient's medical chart. Administration of aminoglycosides every 24 hour was considered as single daily dosing while administration every 8-12 hours was considered as multiple daily dosing. The researcher did not set the criteria for the use of single and multiple dosing. The decision to use single or multiple was made by the physician in charge based on the clinical status of the patient and severity of the condition. Serum creatinine level (SCr) was measured at the commencement of AK and GM course in all patients. Uses of potentially nephrotoxic drugs that were given to >10% of the study patients were included in the analysis.
Study outcome
The outcome of interest in this study was changes in SCr levels during aminoglycoside therapy. Serum creatinine levels were measured daily by laboratory medical technologists by the following method: A sample of 2 mL venous blood was drawn in a plain test tube and spun for five minutes. Then, 5 micro liters of serum were taken from the supernatant and treated with picric acid according to Jaffe method. 17 The intensity of the color was measured at 510 nm which is directly proportional to the serum creatinine concentration.
Statistical analysis
Continuous variables were described using mean ± standard deviation (SD) while categorical variables were expressed as frequency and percentage. Differences in the mean serum creatinine level and the baseline SCr were tested using one sample T test or the Wilcoxson test whatever appropriate based on the normality test of the tested data. Comparison between SCr levels between groups was carried out using independent sample T test or Mann-Whitney U test depending on the Q-Q normality test for each set of data. Data analysis and graphics were carried out using Statistical Package for Social Sciences (SPSS 16).
Results
Description of the sample
During the 12-month study period, 94 patients met the inclusion criteria. Forty-five patients (47.9%) received GM, 49AK (52.1%). Baseline demographic, clinical and laboratory data of the patients are presented in Table 1. The majority of the patients were males (52, 55.3%). The average age of the patients was 63.84 ± 14.59 years and their average body weight was 77.86 ± 15.95 kg. The most common chronic disease present in the study sample was diabetes mellitus (42, 44.7%) followed by hypertension (33, 35.1%). Furosemide was the only potentially nephrotoxic medication that was concomitantly administered in more than 10% of the patient. No significant difference in the administration of furosemide was observed between GM and AK group (P = 0.26). No other potentially nephrotoxic medications were concomitantly administered. The patients were administered GM or AK mainly due to chest infections and urinary tract infections. The average hospitalization duration was 8.52 ± 1.52 days. The majority (51.1%) of the patients in the GM group were administered a dose of 240 mg/day while the majority (55.1%) were administered a dose of 1000 mg/day.
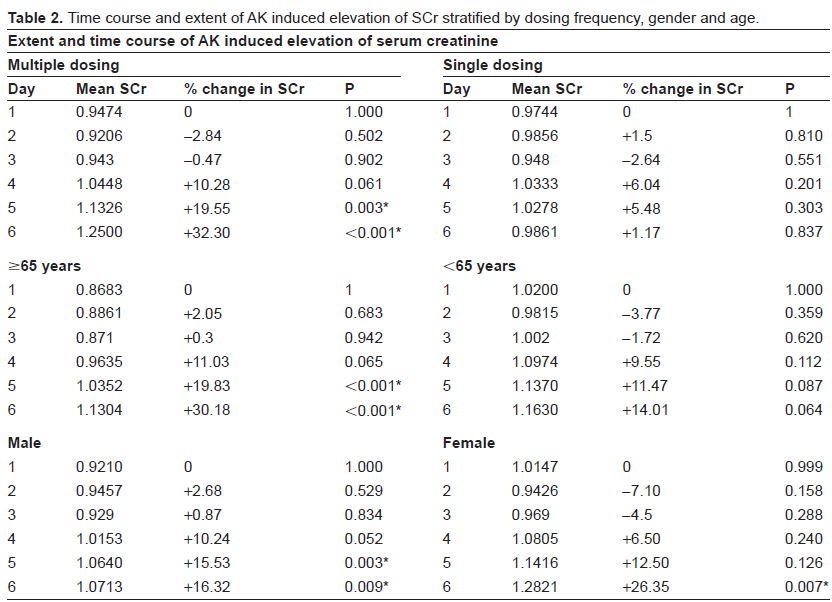
Time course and extent of aminoglycoside induced elevation of SCr.
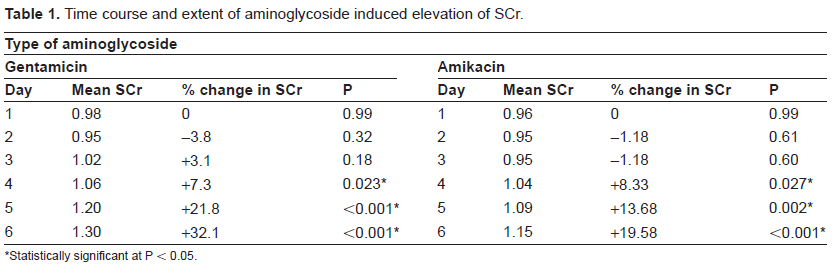
Statistically significant at P < 0.05.
Time course of AK and GM induced SCr elevation
Significant elevation in SCr from baseline value was observed on the 4th day of treatment for GM (P = 0.023) and AK (P = 0.027). The maximum percentage of change in SCr levels from baseline values was 32.1% for GM and 19.58% for AK (Table 1). The difference in the extent of SCr elevation between GM and AK at the 6th day of therapy was significant (P < 0.001) although the baseline SCr value between the two groups was not significantly different.
Variables affecting the time course of AK-induced SCr elevation
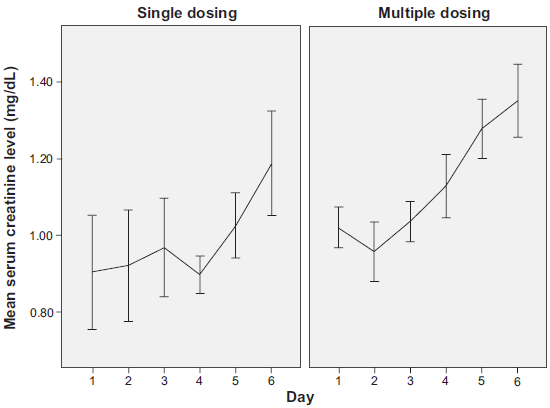
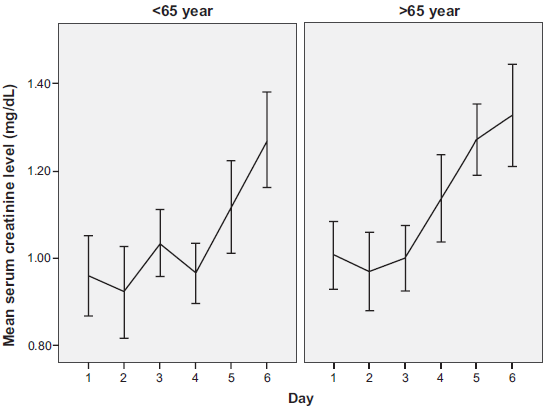
The effect of frequency of dosing, gender and age on the time course of AK induced SCr elevation was investigated (Table 2 and Figs. 1–3). Patients on single AK dosing frequency did not show a significant elevation in SCr levels from baseline value during the 6-day therapy. On the other hand, patients on multiple AK dosing showed a significant elevation of SCr from baseline value from the 5th day (P = 0.003). Multiple AK dosing induced a maximum change in SCr levels of 32.3% from baseline value (Fig. 1). Patients receiving AK and were less than 65 years of age also did not show a significant elevation in Scr levels from baseline value during the 6-day therapy (Fig. 2). In contrast, elderly patients (≥65 years) showed a significant elevation of SCr from baseline value on the 5th day of therapy and reaching a maximum change of 30.18% on the 6th day of therapy. When data regarding elderly patients (≥65 years) were stratified with frequency of dosing, elderly patients on AK single dosing frequency did not show any significant elevation of SCr from baseline value.
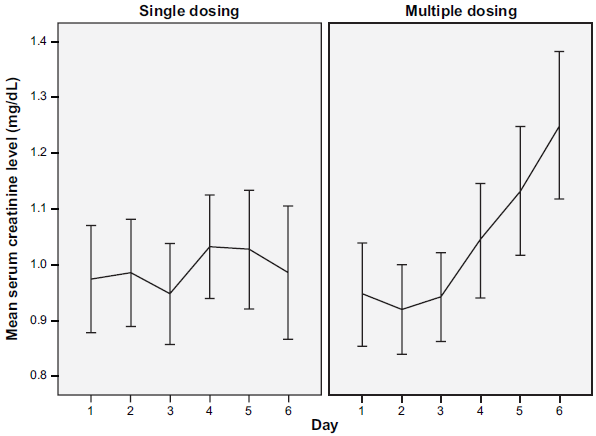
Time course of AK induced SCr elevation after single and multiple dosing frequency dosing.
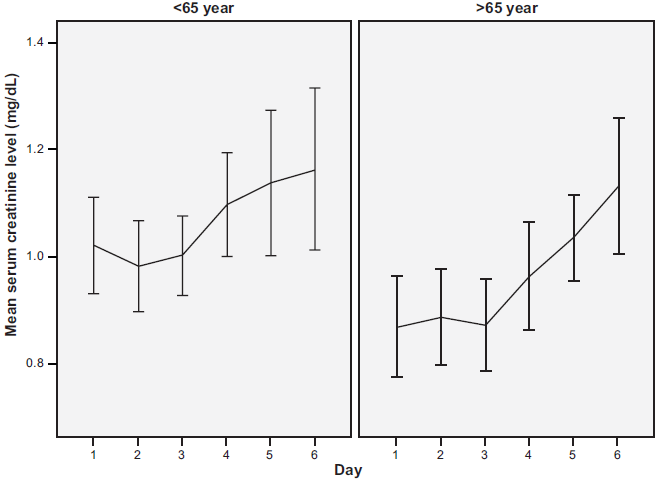
Time course of AK induced SCr elevation in elderly patients (≥65 years) and young (<65 years) patients.
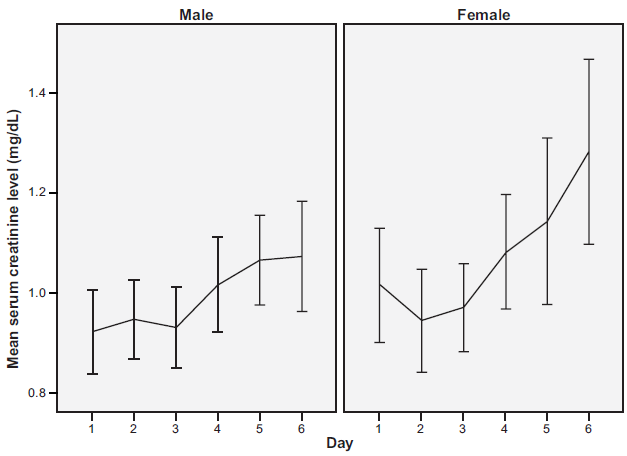
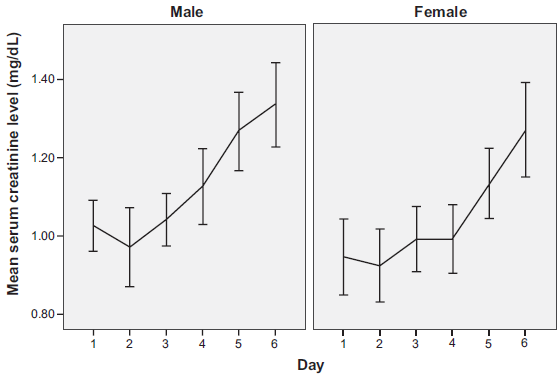
Time course of AK induced SCr elevation in male and female patients.
Time course and extent of AK induced elevation of SCr stratified by dosing frequency, gender and age.
With regard to gender, both males and females showed a significant elevation in SCr from baseline value during the 6 day therapy (Fig. 3). However, males showed the significant elevation in SCr at earlier time course than females (5th day for males versus 6th day for females). Despite that, females on AK showed higher SCr elevation than males on the 6th day of therapy (26% for females versus 16% for males).
Variables affecting the time course of GM-induced SCr elevation
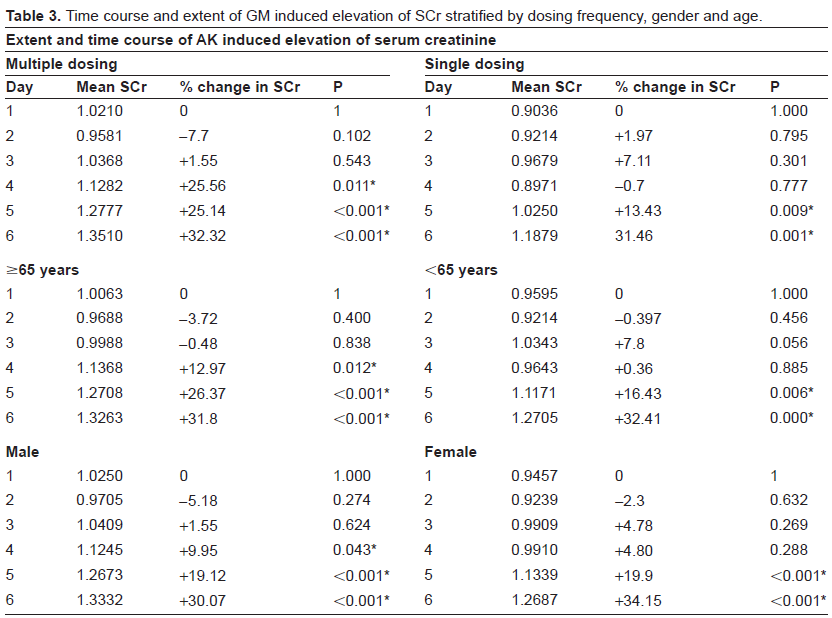
The effect of frequency of dosing, age and gender on the time course of GM induced SCr elevation was also investigated (Table 3 and Figs. 4–6). Patients administered GM as multiple dosing frequencies showed significant elevation in SCr levels starting on the 4th day while on the 5th day for those administered GM as single dosing frequency (Fig. 4). However, at the 6th day of therapy, the extent of SCr elevation was similar between those administered GM multiple and single dosing. Multiple GM dosing induced a maximum change in SCr levels of 32.32% from baseline value while single dosing induced a maximum change of 31.46% (P = 0.57). It is noteworthy that this magnitude of change is approximately similar to that induced by AK multiple dosing. Both elderly and younger patients showed a significant elevation in SCr levels from baseline value during the 6-day therapy (Fig. 5). However, elderly patients (≥65 years) showed a significant elevation of SCr from baseline value on the 4th day of therapy while those <65 years showed a significant rise in SCr on the 5th day of therapy. Similarly, no differences in the extent of SCr elevation were observed at the 6th day of therapy between younger and elderly patients receiving GM (31.8% versus 32.4%, P = 0.64). With regard to gender, both males and females showed a significant and similar extent of elevation in SCr from baseline value during the 6 day therapy (Fig. 6). However, males showed the significant rise in SCr at earlier times than females (4th day for males versus 5th day for males).
Time course of GM induced SCr elevation after single and multiple dosing.
Time course of GM-induced SCr elevation in elderly patients (≥65 years) and young (<65 years) patients.
Time course of GM-induced SCr elevation in male and female patients.
Time course and extent of GM induced elevation of SCr stratified by dosing frequency, gender and age.
Discussion
In this study, hospitalized patients treated with either GM or AK showed significant elevation in SCr as early as the 4th day of therapy. Furthermore, variables like age, gender and frequency of dosing affected the time course of SCr elevation in both AK and GM treated patients, but differently. The time course elevation of SCr observed in this study is in agreement with previous studies. Animal studies have shown that at least several days of aminoglycoside administration are needed before evidence of nephrotoxicity occur.18,19 A study on 25 patients using urine N-acetyl-D-glucosaminidase (NAG) activity as a marker of renal tubular injury have also demonstrated that significant injury to proximal tubules occurred in the very early days of aminoglycoside treatment although the most significant injury occurred following the 7th day of therapy. 20
Regarding dosing frequency, our study showed that for both AK and GM, SCr elevation was delayed or did not occur with single dosing. In AK group, single dosing made lesser extent of SCr elevation than multiple dosing. In the GM group, single and multiple dosing produced the same extent of SCr elevation but multiple dosing showed the significant rise in SCr at an earlier time than single dosing. This is not contradictory to earlier findings that multiple dosing with GM is more nephrotoxic than single dosing.15,21 Nephrotoxicty as defined by many researchers is an increase of 0.5 mg/dl from baseline value. In this study, the number of patients reaching the highest extent of SCr elevation in single and multiple dosing is not necessarily the same as the number of patients meeting the definition of nephrotoxicity. Therefore, technically, the extent and time course of SCr elevation does not necessarily reflect nephrotoxicity.
Aminoglycosides are traditionally administered every 8 hours. However, recent reviews have suggested that administration in larger and less frequent doses (for example, 4-7 mg/kg body weight once per day) offers several advantages, possibly including reduced toxicity. 22 A Meta-analysis study of 21 randomized clinical trials identified through MEDLARS (1966 to January 1995) and included 3091 hospitalized patients mostly with normal baseline renal function concluded the following: Once daily administration of aminoglycosides in patients without pre-existing renal impairment is as effective as multiple daily dosing, has a lower risk of nephrotoxicity, and no greater risk of ototoxicity. 23 The authors of the Meta analysis further recommended that given the additional convenience and reduced cost, once daily dosing should be the preferred mode of administration. Another meta analysis study carried out to assess the relative efficacy and toxicity of single dosing, compared with multiple dosing of aminoglycosides among pediatric patients have concluded that randomized evidence supports the general adoption of single dosing of aminoglycosides in pediatric clinical practice. This approach minimizes cost, simplifies administration, and provides similar or even potentially improved efficacy and safety, compared with MDD of these drugs. 24
In this current study, younger patients on amikacin or gentamicin showed delayed significant elevation in SCr suggesting that elderly patients are more susceptible to aminoglycoside nephrotoxicity. However, it was noteworthy that elderly patients on amikacin showed no significant elevation in SCr during the 6-day therapy. Advanced age has long been held to be an important risk factor in the development of aminoglycoside-related toxicity.25,26 For this reason many physicians avoid use of aminoglycosides in the elderly. However, intolerance to antibiotics of other classes and the emergence of organisms that exhibit resistance to other antibiotics has necessitated retention of aminoglycosides in the clinical practice for elderly patients.
In the current study, gender has a different effect on SCr elevation time course in patients treated with AK or GM. Males on AK showed an earlier significant rise in SCr compared to females. However, females showed greater extent of SCr rise than males. Actually, the SCr levels in females (mean = 1.28) on AK was significantly higher than those in males (mean = 1.071) at the 6th day of therapy (P = 0.035). This is in agreement with previous study that has shown that hospitalized female patients were significantly more susceptible to nephrotoxicity with amikacin than male patients. 16 These data might suggest that although males show earlier signs of nephrotoxicity than females, yet, females show greater extent of nephrotoxicty than males when treated with amikacin. With regard to gentamicin, human females were reported to be affected by gentamicin nephrotoxicity more than males. 27 Other workers, however, have found that male humans are more susceptible than females to the morphologic and functional effects of gentamicin nephrotoxicity. 28 The mechanisms underlying gender differences in aminoglycosides induced nephrotoxicity are difficult to explain. However, such difference could be ascribed to hormonal and/or pharmacokinetic differences between both sexes. Several correlations between renal brush border membrane binding affinity of aminoglycoside and aminoglycoside nephrotoxicity have been cited including the greater binding affinity in male versus female rats. 29 However, this correlation contradicts our finding that females were more susceptabile to nephrotoxicity than males. In conclusion, more investigation is needed to study the impact of gender on aminoglycide induced nephrotoxicity.
In conclusion, no differences were observed between AK and GM induced SCr elevation time course in general. Elevation in serum creatinine levels are greatly reduced or even abolished when AK is administered in single dosing or to patients less than 65 years of age. In case of GM, age, gender and frequency of dosing change the time course of SCr elevation but did not affect the extent of SCr elevation.
Disclosure
The author reports no conflicts of interest