
Abstract
Hypertension is one of the most important modifiable risk factor for cardiovascular morbidity and mortality and is highly prevalent. Recent guidelines and advisory statements have recommended lower thresholds and goals for patients with hypertension. However, approximately two-thirds of hypertensive patients do not achieve the goals. Poor adherence to anti-hypertensive medication regimens is a common cause of the practice-outcome gap. Monotherapy is also associated with difficulty to control blood pressure (BP) as most of hypertensive patients require 2 or more antihypertensive agents to effectively reduce BP. Therefore, current guidelines have recommended the use of combination therapy early in the management of hypertension or as first-line treatment. Fixed-dose combinations offer many advantages, such as convenience of use and fewer adverse events. Blockage of two or more BP regulatory systems also provides a more effective and physiologic BP reduction. Similar to other combinations, fixed-dose combination tablets containing dihydropyridine calcium channel blockers and angiotensin receptor blockers bring together two distinct and complementary mechanisms of action.
Introduction
Hypertension remains the leading cause of mortality and the third largest cause of disability in both developed and developing countries.1,2 Worldwide, 7.6 million premature deaths, 54% of stroke and 47% of ischemic heart disease were attributed to high blood pressure (BP) in 2001. 3 Overall, 26.4% of the adult population in 2000 had hypertension and 29.2% were projected to have this disease by 2025. The number of adults with hypertension in 2025 was predicted to as many as 1.5 billion people worldwide. 4
Significant cardiovascular (CV) risk reduction can be achieved with BP reduction.4,5 Observational studies have shown that mortality from ischemic heart disease and stroke in persons 40 to 89 years of age increases in log linear fashion with increases in both systolic (SBP) and diastolic BP (DBP). 6 For each increase in SBP of 20 mmHg or in DBP of 10 mmHg over the entire range from 115/75 mmHg, there is a twofold increase in mortality related to coronary artery disease and stroke.
BP control is the most important single issue in the management of hypertension and is rarely achieved with one drug. Although the awareness and control of hypertension have increased, approximately two-thirds of patients do not achieve the goal of < 140/90 mmHg. Approximately 65% of hypertensive patients need ≥2 antihypertensive agents to achieve BP control. For example, in the Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack (ALLHAT) 7 and in the Losartan Intervention For Endpoint (LIFE) 8 trials, >70% and >90%, respectively, required ≥2 antihypertensive agents to achieve goal BP (< 140/90 mmHg).
Based on clinical trials, recent guidelines have recommended the use of combination therapy early in the management of hypertension in patients with comorbidities that require prompt BP reduction or as first-line treatment (for persons with BP > 20/10 mmHg above goal).9,10
Importance of Adherence
Patient adherence is the ability and willingness of an individual patient to take medication as prescribed, complete recommended tests and consultations, follow health-related advice, and attend scheduled clinic appointments. 11 Poor adherence to medication regimens contributes to the practice-outcome gap, in which clinical guidelines are implemented but expected benefits are not realized. Adherence rates are higher in patients with acute conditions. However, chronic conditions, such as hypertension, have low adherence rates. Clinical trials report average adherence rates of only 43 to 78% among patients receiving treatment for chronic conditions.12,13 Poor adherence to the antihypertensive treatment can be partially explained due to the absence or few symptoms related to hypertension, side effects of medications and complexity of treatment, such as multiple medications. 14
Adherence rate is inversely related to the number of drugs given. For example, patients are more adherent when they take a combination as a single tablet than if they are given the same drugs as two separate pills, even when dosed once daily. 15 A meta-analysis of 9 studies with different diseases compared fixed-dose combinations versus free-drug components of the regimen separately. Fixed-dose combinations improved the adherence rate by 26% compared with free-drug component regimens. A subgroup analysis of the 4 studies done with hypertensive patients showed that fixed-dose combinations decreased nonadherence to treatment by 24% compared with free-drug combinations. 16
Complexity of the dosing regimen/number of drugs is also related to patient adherence, i.e. there is a clear inverse relationship between complexity of the treatment and adherence. For example, among 198 Canadian hypertensives randomized to diltiazem twice-daily compared to amlodipine once-daily, those on the once-daily regimen took the medication more regularly than those on the twice-daily dosing. 17
Role of Fixed-Dosed Combination Therapy in the Treatment of Hypertension
Fixed-dose combination therapy is an efficacious, safe and cost-effective method for decreasing BP in most patients with essential hypertension. 18 Fixed-dose combinations offer many advantages such as increased compliance, convenience of use, additive or synergistic effects, and reduction of adverse events.
As many pathophysiologic factors contribute to high BP, the combination of agents with different (and complementary) mechanisms of action provides more complete blockage of pressor mechanisms with less activation of counter-regulatory mechanisms.
Combining two antihypertensive agents with complementary mechanisms of action produces significantly greater BP reduction than either of the components as monotherapy.19–21
Fixed-dose combinations also increase adherence to antihypertensive treatment. For example, adherence to a fixed-dose combination of the calcium channel blocker (CCB) amlodipine with the angiotensin converting-enzyme (ACE) inhibitor benazepril has been compared to adherence to free-dose combination therapy. Hypertensive subjects receiving once-daily, single-capsule, fixed-dose combination of amlodipine/benazepril demonstrated significantly greater adherence than subjects receiving an ACE and a CCB as separate components (80.8 vs. 73.8%, respectively). 22 The average annual cost of CV-related care per subject was also significantly lower in hypertensive patients receiving the fixed-dose.
Combinations with ACE inhibitors- or angiotensin receptor blockers (ARBs) and thiazide diuretics are the most commonly used fixed-dose combination because of an additive effect on BP reduction related to complementary mechanisms of action of the components and the favorable vascular, metabolic, cardiac and renoprotective effects of the ACE inhibitors and ARBs.9,23,24 Randomized controlled clinical trials that compared the combination versus monotherapy with either ACE inhibitor or HCTZ have generally demonstrated greater BP-lowering efficacy with low-dose combinations over higher-dose monotherapy with either single agent.25,26
Appropriate combination therapy improves tolerability if one component is able to neutralize the adverse effects of the second agent. For example, the peripheral edema caused by the dihydropyridine CCB amlodipine is reduced with ARBs or ACE inhibitors.27–29 In a prospective, randomized, double-blind study 1,079 hypertensive patients were assigned to receive amlodipine/benazepril or amlodipine or nifedipine monotherapy. Although the incidence of edema was 15% in the high-dose nifedipine group and 24% in the high-dose amlodipine group, it was greatly reduced in patients treated with any dose of combination therapy (1.5%-3.8%) or low-dose CCB (4.9%-5.4%). 27
Olmesartan
ARBs selectively block the binding of angiotensin II to the AT1 receptor in vascular smooth muscle and other cell types. 30 Olmesartan lowers BP rapidly and effectively in hypertensive patients. An analysis of 7 randomized, double-blind, placebo-controlled studies compared the safety and efficacy of olmesartan monotherapy to placebo in patients with essential hypertension. 31 Olmesartan produced dose-dependent BP reductions in both DBP and SBP within 1 week of initiating treatment, and the response was nearly maximal within 2 weeks.
Olmesartan reduces BP more effectively than other ARBs at traditionally recommended starting doses. 32 In a multicenter, randomized, double-blind trial, 588 patients received once-a-day therapy with the recommended starting doses of losartan, valsartan and irbesartan. This study showed a significantly greater reduction in sitting cuff DBP at trough with olmesartan (11.5 mmHg) than with losartan, valsartan, and irbesartan (8.2, 7.9, and 9.9 mmHg, respectively, p < 0.005 olmesartan vs. losartan; p < 0.05 olmesartan vs. valsartan and irbesartan). 33 The reduction in mean 24-hour SBP with olmesartan (12.5 mmHg) was significantly greater than those with losartan and valsartan (9.0 and 8.1 mmHg, respectively) and equivalent to the reduction with irbesartan (11.3 mmHg). The reduction in mean 24-hour DBP with olmesartan (8.5 mmHg) was significantly greater than reductions with losartan and valsartan (6.2 and 5.6 mmHg, respectively, p < 0.05) and showed a trend toward significance when compared to the reduction in DBP with irbesartan (7.4 mmHg; p = 0.087).
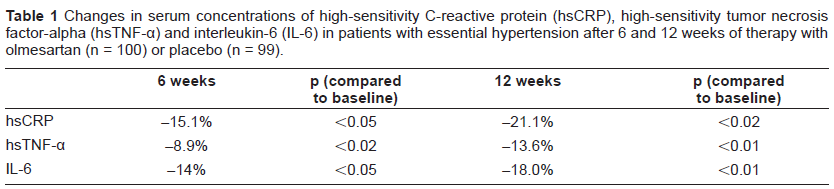
Pleiotropic effects, such as vasoprotective and antiinflammatory effects, beyond BP reduction have been described with Olmesartan. In the EUropean Trial on Olmesartan and Pravastatin in Inflammation and Atherosclerosis (EUTOPIA) study, investigators compared the antiinflammatory effects of olmesartan alone and in combination with pravastatin in patients with essential hypertension and microinflammation. 34 Olmesartan significantly reduced serum levels of tumor necrosis factor-alpha (TNF-α), high-sensitivity C-reactive protein (hs-CRP), monocyte chemotactic protein-1 (MCP-1), and interleukin-6 (IL-6) compared to placebo independently of BP reduction (Table 1). Treatment with pravastatin alone did not significantly alter inflammation markers. In the Multicenter Olmesartan Atherosclerosis Regression Evaluation (MORE) study, carotida intima media thickness (IMT) and plaque volume were evaluated in 165 hypertensive patients with carotid artery disease and increased CV risk. 35 Patients were randomized to receive olmesartan or atenolol for 2 years. Although both treatments reduced IMT similarly, preferential decrease in plaque volume of larger plaques was seen with olmesartan. These changes occurred despite similar reductions in BP, suggesting an antiatherosclerotic action of olmesartan that is independent of its BP lowering effect. Finally, the Vascular Improvement with Olmesartan medoxomil Study (VIOS) evaluated if olmesartan reverses abnormal remodeling of resistance vessels and has favorable effects on central hemodynamics compared to the beta blocker atenolol despite equivalent BP control. 36 Olmesartan reversed small resistance vessel remodeling virtually back to normal, while atenolol had little to no effect on the vascular wall in spite of the presence of nearly physiological BP control. Although olmesartan has favorable effects on surrogate endpoints, results of outcome trials are not yet available. The Randomized Olmesartan and Diabetes Microalbuminuria Prevention (ROADMAP) study is evaluating the effect of the ARB olmesartan medoxomil on the incidence of microalbuminuria in 4400 patients with type 2 diabetes and normoalbuminuria. 37 ROADMAP, will also assess the effects of olmesartan on fatal and non-fatal CV events.
Changes in serum concentrations of high-sensitivity C-reactive protein (hsCRP), high-sensitivity tumor necrosis factor-alpha (hsTNF-α) and interleukin-6 (IL-6) in patients with essential hypertension after 6 and 12 weeks of therapy with olmesartan (n = 100) or placebo (n = 99).
Amlodipine
Dihydropyridine CCBs act by decreasing calcium entry to cells through the L-type calcium channel. 38 It decreases the availability of intracellular calcium in arterial smooth muscle cells and consequently prevents actin and myosin from interacting, resulting in vasodilation. 39 Furthermore, dihydropiridine CCBs also facilitate natriuresis by increasing renal blood flow, dilating afferent arterioles, and increasing glomerular filtration pressure.
Amlodipine is a long-acting 3rd generation dihydropyridine CCB that is the most commonly used agent in its class for the treatment of hypertension.40,41 Amlodipine effectively reduces BP and CV morbidity and mortality. The Valsartan Antihypertensive Long-Term Use Evaluation (VALUE) trial compared the effects of amlodipine and valsartan as first line therapy in reducing CV outcomes in hypertensive patients at high CV risk. 42 Amlodipine treatment was associated with a more prompt and larger BP reduction than valsartan treatment, particularly early in the trial when participants were on monotherapy. Amlodipine treatment also significantly reduced the incidence of nonfatal myocardial infarction compared to valsartan treatment.
In the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA) study, the amlodipine-perindopril regimen was more effective in reducing BP and preventing CV events than the atenolol-bendroflumethiazide regimen. 43 BP was, on average, 2.7/1.9 mmHg lower in the amlodipine group than in the atenolol group during 5.7 years of follow-up and amlodipine-based treatment was superior in preventing fatal and nonfatal stroke and total CV events compared to atenolol-based treatment. Amlodipine ± perindopril was also superior in reducing procedures and all-cause mortality compared to atenolol ± bendroflumethiazide.
Although amlodipine is effective in reducing BP and CV morbidity and mortality, it does not reduce heart failure. In the ALLHAT, over 40,000 high risk hypertensive patients were randomized to receive chlorthalidone, amlodipine, lisinopril or doxazosin. 44 Amlodipine was as effective as chlorthalidone in reducing the primary combined endpoint of fatal coronary heart disease or nonfatal myocardial infarction. Furthermore, amlodipine was effective in reducing end-stage renal disease and combined coronary heart disease events. However, heart failure was 38% more common in patients assigned to amlodipine than patients assigned to chlorthalidone in the absence of concomitant therapy with ACE inhibitors or ARBs in either group. There was a small but significant difference in SBP between the groups.
Amlodipine is also effective in decreasing left ventricular mass in hypertensive patients. In the Effects of Amlodipine and Lisinopril on Left Ventricular Mass and Diastolic Function (ELVERA) trial, which compared amlodipine to lisinopril therapy in 166 elderly hypertensive patients, amlodipine and lisinopril reduced left ventricular mass and improved diastolic function to a similar extent after 2 years of follow-up. 45
Olmesartan-Amlodipine Combination
Recent studies have demonstrated the synergism between ARBs and CCBs in vascular protection. In an experimental study, inflammatory vascular remodeling injury was induced by a polyethylene tube placed loosely around the left femoral artery of mice. 46 Those animals were subsequently treated with olmesartan monotherapy or in combination with CCBs (nifedipine, amlodipine and azelnidine) or HCTZ. The combination of olmesartan with CCB significantly inhibited neointimal formation, oxidative stress and inflamatory markers.
The pharmacokinetic profile of amlodipine and olmesartan have been studied after coadministration of amlodipine besylate and olmesartan medoxomil concomitantly as separate dosage forms and together in a fixed-dose combination tablet in healthy volunteers. 47 The mean steady-state pharmacokinetics of amlodipine and olmesartan were similar when olmesartan medoxomil 40 mg/day and amlodipine 10 mg/day were administered separately or concomitantly demonstrating that, from a pharmacokinetic perspective, the two drugs are suitable for coadministration in a fixed-dose combination.
The combination of olmesartan and amlodipine in a single tablet effectively reduces BP and attenuates the adverse events of the amlodipine component in patients with hypertension. In the Combination of Olmesartan medoxomil and Amlodipine besylate in Controlling High blood pressure (COACH) study, 1,940 subjects with mild to severe hypertension (seated DBP ranging from 99/120 mmHg) entered in an 8-week, double-blind, multi-center, randomized, placebo controlled, parallel group, factorial study. 48 The study compared BP reduction with placebo, monotherapy with amlodipine 5 or 10 mg, olmesartan medoxomil 10, 20, or 40 mg, and combination therapy with amlodipine/olmesartan medoxomil at doses of 5/10, 5/20, 5/40, 10/10, 10/20, and 10/40 mg. All combinations produced greater mean BP reductions than either drug alone. The highest dose combination, amlodipine 10 mg plus olmesartan 40 mg, reduced SBP by 28.5 mmHg and DBP by 19.4 mmHg, compared to 18.9 and 13.3 mmHg, respectively, for amlodipine alone. The proportion of patients that achieved the BP goal after 8 weeks was higher within patients that received combination therapy than those treated with monotherapy. The addition of olmesartan to amlodipine also decreased the amlodipine-related adverse effects. The frequency of edema was 36.8% in patients treated with amlodipine 10 mg monotherapy and 23.5% in those treated with amlodipine 10 mg plus olmesartan 40 mg. All combinations of amlodipine 10 mg with olmesartan demonstrated less peripheral edema than amlodipine 10 mg monotherapy.
Combination of olmesartan and amlodipine is also effective in patients that remained hypertensive after amlodipine monotherapy. In a double-blind, parallel-group, multicenter study, patients with moderate to severe hypertension (mean BP at baseline 164/102 mmHg) that had failed to respond to treatment with open-label amlodipine 5 mg for 8 weeks were randomized to receive amlodipine 5 mg plus placebo or a combination of olmesartan medoxomil (10-40 mg) plus amlodipine 5 mg for a further 8 weeks. 49 Patients in whom both SBP and DBP were ≥140/90 mmHg at week 16 had their medication increased to olmesartan medoxomil/amlodipine 20/5 mg, 40/5 mg or 40/10 mg. More than 70% of patients on active combination therapy achieved BP goal (< 140/90 mmHg or < 130/80 mmHg for patients with diabetes) by week 24 and all combination regimens were well tolerated (Fig. 1).
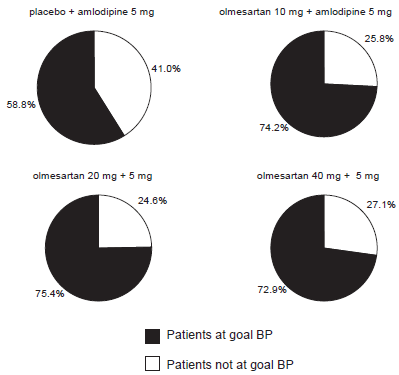
Percentage of patients who achieved target BP (< 140/90 mmHg or < 130/80 mmHg for patients with diabetes). (Modified from Volpe M, Brommer P, Haag U, Miele C. Efficacy and tolerability of olmesartan medoxomil combined with amlodipine in patients with moderate to severe hypertension after amlodipine monotherapy: a randomized, double-blind, parallel-group, multicentre study. Clin Drug Investig 2009;29:11-25).
Moreover, the combination of olmesartan with amlodipine results in a better metabolic and anti-inflammatory effects than the combination of olmesartan with hydrochlorothiazide. The former combination significantly decreased insuline resistance and inflammatory markers such as TNF-α, hs-CRP, IL-1 and IL-6. 50
Conclusions
Combination therapy has become widely accepted by health care providers for the treatment of hypertension and is recommended by current guidelines. Fixed-dose combinations offer many advantages such as increased compliance, convenience of use, additive or synergistic effects, and reduction of adverse events. Effective combination therapies, such as olmesartan plus amlodipine, block two or more BP regulatory systems providing more effective and more physiologic BP reduction than most monotherapies.