
Abstract
Tight glycemic control in type 1 and type 2 diabetes reduces the risk for microvascular complications, including retinopathy, nephropathy, and neuropathy. Yet, despite intensive insulin regimens, many insulin-dependent patients are unable to achieve euglycemic states. This review will focus on pramlintide, an equipotent amylin analog, and its role in the management of diabetes. Pramlintide lowers glucose through the same mechanisms as amylin: it slows gastric emptying, suppresses the postprandial rise of glucagon in patients with diabetes, and promotes satiety. Long-term clinical trials have shown that the use of pramlintide as an adjunct to insulin minimizes postprandial glucose excursions and reduces both HbA1C and body weight when compared to placebo. Although its effects on HbA1C are modest, pramlintide has gained popularity as a result of its relatively few contraindications, limited side effects, minimal risk for hypoglycemia, and potential for weight loss. The combination of insulin and pramlintide may provide an effective means for patients with diabetes to meet their HbA1C goals.
Diabetes affects 23.6 million people in the United States, or 8% of the population. Diabetic retinopathy is the leading cause of new cases of blindness in adults between the ages of 20 and 74, affecting between 12,000 and 24,000 patients yearly. It is also the leading cause of renal failure in the United States. In 2005, 46,739 people with diabetes began treatment for end-stage renal disease. The ADA estimates that 60% to 70% of patients with diabetes exhibit nervous system damage in the form of impaired sensation or pain in the extremities, slowed transit of food through the stomach, or carpal tunnel syndrome (ADA 2008).
It is well established that tight glycemic control in type 1 and type 2 diabetes reduces the risk for microvascular complications, including retinopathy, nephropathy, and neuropathy (DCCT 1993, UKPDS 1998). Furthermore, any decrease in the HbA1C appears to confer this advantage (DCCT 1996). Despite intensive insulin use, many insulin-dependent patients are unable to achieve euglycemic states (DCCT 1993; UKPDS 1998). Deterrents to goal HbA1C's include weight gain with insulin and difficulty controlling postprandial rises in blood glucose. 1 The weight gain caused by insulin is not only cosmetically undesirable but also increases cardiovascular risk and the incidence of metabolic syndrome. Insulin therapy alone is often unable to sufficiently mimic endogenous postprandial surges in insulin and amylin.
This review will focus on pramlintide, an equipotent amylin analog, and its role in the management of type 1 and type 2 diabetes. In 2005, the FDA approved its use at mealtimes for both type 1 and insulin-treated type 2 diabetes. In type 1 diabetes, it is used as an adjunct treatment in patients already optimized with preprandial insulin and basal insulin but unable to achieve target glucose levels. In type 2 diabetes, it is similarly used as an adjunct treatment in patients already using preprandial and basal insulin with or without concurrent sulfonylurea and/or metformin use. Since pramlintide is given as a mealtime subcutaneous injection, it mainly targets postprandial glycemic excursions. Although its effects on HbA1C are modest and it often causes transient nausea, pramlintide has gained popularity as a result of its relatively few contraindications, minimal risk for hypoglycemia and potential for weight loss. This paper will review pramlintide's mechanisms of action, clinical efficacy in terms of achieving goal HbA1C's and weight loss, safety and tolerability, patient satisfaction, and directions for future consideration.
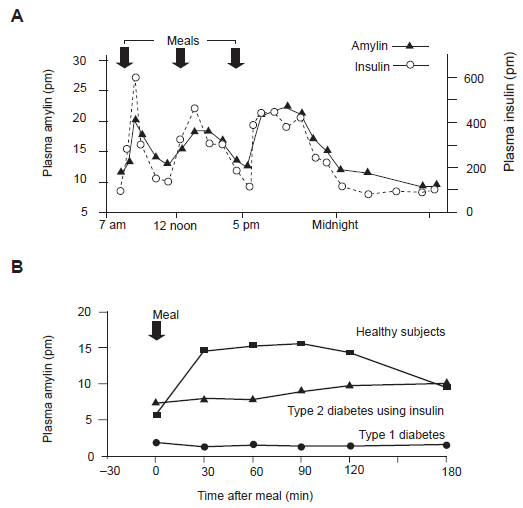
Amylin is a 37-amino acid polypeptide with a 6-amino acid ring structure that is co-secreted along with insulin by pancreatic β cells in response to a nutrient stimulus.1–3 Like insulin, it downregulates glucose levels. In healthy subjects, it is secreted in pulses every six to eight minutes. 4 However, amylin secretion appears to be diminished or absent in patients with type 1 and 2 diabetes (Fig. 1). 5 The severity of amylin deficiency closely coincides with the degree of insulin deficiency. 3 Native amylin is characterized as “glue-like” and unstable in solution. Therefore, native amylin was modified to form pramlintide, an injectable synthetic version of amylin. By replacing three amino acid residues ( 25 Ala, 28 Ser, and 29 Ser), pramlintide mimics amylin's physiologic properties in the form of a stable injectable product (Fig. 2).6–8
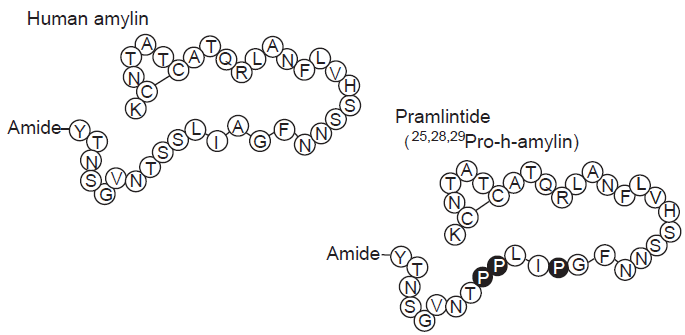
Amino Acid sequences of human amylin and the amylin analogue pramlintide. Reprinted with permission. 9
Pramlintide lowers glucose through the same mechanisms as amylin: It slows gastric emptying, suppresses the postprandial rise of glucagon in patients with diabetes, and promotes satiety.10,11
Gastric emptying occurs more rapidly in patients with type 2 diabetes when compared to controls. 12 This acceleration may be partially due to the decreased or absent amylin levels characteristic of diabetes. Pramlintide slows gastric emptying for both liquids and solids (Fig. 3A), thus limiting the rate at which nutrients enter circulation and decreasing postprandial glucose excursions. Pramlintide also suppresses the postprandial rise of glucagon. Glucagon is released by the alpha cells of the pancreas in response to hypoglycemia in order to stimulate hepatic glucose production. Postprandial levels of glucagon are abnormally elevated in type 1 and type 2 diabetes and cause both increased glycogenolysis and gluconeogenesis.13,14 Pramlintide has been shown to significantly reduce postprandial glucagon excursions when compared to placebo. (Fig. 3B)10,15 Finally, in patients with type 2 diabetes and in overweight patients without diabetes, a single pre-prandial injection of pramlintide has been shown to reduce food intake by 16%-23%. Pramlintide-treated patients experience increased levels of satiety when compared to controls (Fig. 3C). 16
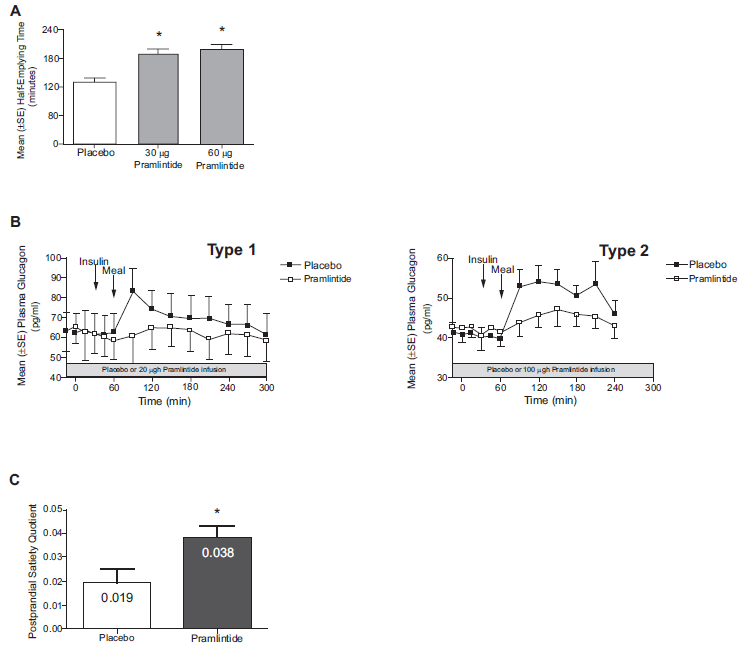
Pramlintide's 3 mechanisms of actions.
The two pivotal studies involving pramlintide use in patients with type 1 diabetes were performed by Ratner et al. and Whitehouse et al. In a multicenter, double-blind, placebo-controlled trial, Ratner et al. showed that pramlintide dosed TID or QID over one year led to A1C reductions in patients with type 1 diabetes of 0.29% (p < 0.011) and 0.34% (p < 0.001), respectively, compared to only a 0.04% reduction in a placebo group. 18 The proportion of test subjects who achieved a target A1C of < 7% was 3 times higher than control subjects. Weight loss tended to occur more in obese patients than in patients at ideal body weight. Ratner et al. also demonstrated positive effects on glycemic control when a subset of patients with A1C values < 8% were evaluated along with similar patients from other studies. 19
Whitehouse and colleagues conducted a multicenter, double-blinded, placebo-controlled trial analyzing the efficacy of adjunctive pramlintide on both glycemic and weight control in patients with type 1 diabetes. In a 52-week trial, they randomized patients with type 1 diabetes to receive premeal injections of placebo or 30 μg-60 μg of pramlintide in addition to existing insulin regimens. They found that the patients using pramlintide had a modest (<1%) but sustained reduction in A1C (Fig. 4). 20 The target A1C of less than 7% was achieved in 25% of patients taking pramlintide versus only 11.3% in the control patients without an increased incidence of hypoglycemic events. Test subjects experienced weight loss while the insulin-only control group gained weight. The weight loss was significant from week 13 onward.
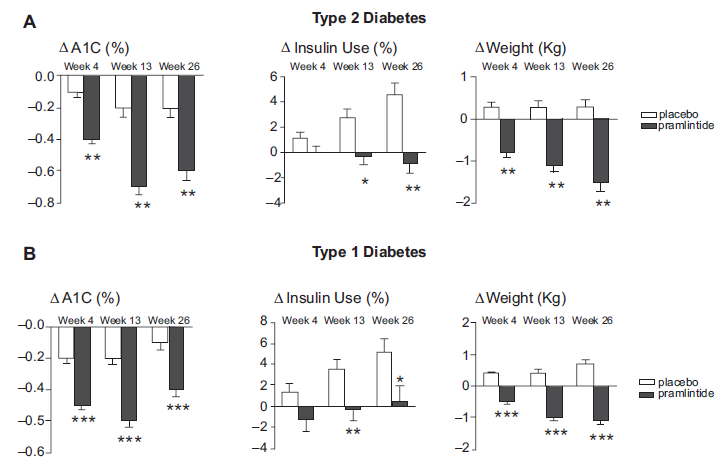
Results for combined pivotal studies with pramlintide in patients with type 1 and type 2 diabetes. The change in A1C, total daily insulin use and weight at 4, 13, and 26 weeks are expressed as mean ± SE, ITT observed.
In 2006, Edelman et al. evaluated pramlintide's ability to facilitate weight loss in patients with type 1 diabetes. They published the results of a 29-week, randomized, double-blind, placebo-controlled trial in which 296 patients with type 1 diabetes were treated with pramlintide vs. placebo. They reported that pramlintide treatment led to a significant reduction in weight (p < 0.0001) despite equivalent HbA1C reductions relative to a placebo. 21
Hollander et al. and Ratner et al. investigated the role of pramlintide in the treatment of type 2 diabetes. Hollander et al. studied the effects of pramlintide in patients with type 2 diabetes on insulin with or without a sulfonylurea or metformin in a double-blind, placebo-controlled, parallel-group study. Patients receiving pramlintide 60 μg TID, pramlintide 90 μg BID, or pramlintide 120 μg BID were evaluated at 26 and 52 weeks for change in HbA1C and body weight. They showed that 120 μg of twice daily pramlintide significantly reduced both HbA1C and weight. In addition, 9.4% of the pramlintide 90 μg BID group and 12% of the pramlintide 120 μg BID group achieved a HbA1C < 7% compared to only 4.1% of placebo patients. Furthermore, 42.4% the pramlintide 90 μg BID group and 45.7% of the pramlintide 120 μg BID group compared to only 27.6% of placebo achieved a HbA1C < 8%. 22
Ratner et al. compared pramlintide to placebo in patients with type 2 diabetes and showed that test patients were more likely to have reductions in HbA1C and body weight (Fig. 4). In a 52-week, double-blind, placebo-controlled, parallel group study, insulin-using patients were randomized to receive pramlintide 30, 75, 150 μg TID or placebo TID. The end points included changes in HbA1C, and body weight from baseline at weeks 13, 26, and 52 as well as changes in insulin use and proportion of patients attaining goal HbA1C values. Significant reductions in HbA1C were seen in the 75 and 150 μg groups at week 13 and 26. However, by week 52, the reduction in HbA1C was only significant in the 150 μg group. The proportion of patients attaining a goal HbA1C of < 7% was 12.7%, 13.4%, 19.2% and 11.1% in the pramlintide 30, 75, 150 μg and placebo TID groups, respectively. The proportion of patients attaining a goal HbA1C of < 8% was 45.1%, 46.4%, 54% and 37.6% in the pramlintide 30, 75, 150 μg and placebo TID groups, respectively. All pramlintide patients had significant reductions in body weight at weeks 13, 26, and 52, while patients in the placebo group actually gained an average of 1 kg by 26 weeks. 23
Riddle et al. assessed the efficacy of pramlintide in 212 patients who were sub-optimally controlled on glargine insulin with or without oral antidiabetes agents. 24 Patients were randomized to receive 60 mcg or120 mcg of pramlintide or placebo BID or TID for sixteen weeks in addition to their preexisting diabetes regimens. The primary endpoints included the change in HbA1C and a composite measure of overall diabetes control (including A1C < 7% or reduction by at least 0.5%, body weight neutral, hypoglycemic events). Patients receiving pramlintide had a significant reduction in HbA1C compared with placebo (−0.70 vs. −0.36, P < 0.050). More pramlintide than placebo-treated patients achieved the composite end point (25 vs. 7%; P < 0.001). Improvement in glycemic control was accompanied by progressive weight loss with pramlintide and weight gain with placebo (−1.6 +/- 0.3 kg vs. +0.7 +/- 0.3 kg; P < 0.0001). This study suggests that pramlintide may be a promising alternative to mealtime insulin in patients who desire weight loss and are not adequately controlled on basal insulin.
Pramlintide should be injected subcutaneously in the abdominal area or thigh immediately before meals. Pramlintide should not be mixed with insulin or injected at the same site as insulin. 25 For safety purposes, it is recommended to be given before a meal containing 250 calories, and the usual preprandial insulin dose should be halved at first and then uptitrated as tolerated to minimize hypoglycemia.25–28 In type 1 diabetes, several studies show that the rates of hypoglycemia are increased in pramlintide treated patients versus placebo.19–21,29 However, pramlintide does not appear to reduce the glucagon response to hypoglycemia. In fact, one study showed that none of the counter-regulatory hormones triggered by hypoglycemia, i.e. catechol-amines, growth hormone, cortisol, and glucagon, were attenuated by pramlintide. 30
Because pramlintide works in part by slowing gastric emptying, it may delay the absorption of oral medications. Therefore, oral medications should be taken either an hour before or two hours after an injection of pramlintide. Caution should also be used when patients are already receiving anticholinergics or agents that slow intestinal absorption, such as α-glucosidase inhibitors. Since nausea is more likely to be a problem in patients with gastroparesis, pramlintide is generally considered to be contraindicated in these patients. Pramlintide dosing does not need to be adjusted for the elderly or for patients with renal or hepatic impairment. However, there are no studies in dialysis patients and it has not yet been approved for use during pregnancy. It should not be used in patients who do not require insulin or are on basal insulin only. As of now, it is not approved for use with exenatide or Januvia. There are no reports to date of toxicity to major organs or any deleterious effects on the physical exam, hemodynamics, electrocardiograms, or laboratory tests.
The starting dose in type 1 diabetes is 15 μg, and this dose may be uptitrated in increments of 15 μg every three to seven days for a goal of 60 μg. In patients with type 2 diabetes, the initial dose is higher at 60 μg, and the target dose is 120 μg. Therapy is started at these lower doses to reduce the incidence of nausea. A small subset of patients may have intolerable nausea despite receiving the lowest doses. In most patients, however, the nausea, vomiting, and anorexia tend to resolve following the first 4-8 weeks of therapy. There have been some potential safety concerns involving proper dosing of pramlintide. Symlin has a concentration of 600 mcg/ml solution. When pramlintide was first introduced to the market, it was labeled as a 0.6 mg/ml solution. This was a possible source of confusion for patients since pramlintide is dosed in micrograms rather than milligrams. In addition, patients may be confused by the instructions to withdraw the medication in units using an insulin syringe. The product is currently labeled as containing 600 mcg/ml, and the advent of the SymlinPen has helped further simplify dosing. In 2007, Amylin Pharmaceuticals, Inc. developed two new prefilled pen-injector devices called the SymlinPen® 120 and the SymlinPen® 60. The SymlinPen® 120 can deliver 60 or 120 micrograms of pramlintide per dose, while the SymlinPen® 60 can deliver 15, 30, 45, or 60 micrograms of pramlintide per dose. Both pens can be stored at room temperature (though not to exceed 86° F) once they are in use. SymlinPen® 60 is formulated as a 1000 mcg/ml solution, and each box contains two 1.5 ml Syringes. The wholesale price for one box is $121.56. SymlinPen® 120 is formulated as a 1000 mcg/ml solution, and each box contains two 2.7 ml Syringes. The wholesale price for one box is $243.12 (Amylin Customer Support Center, 1-800-349-8919).
Marrero et al. conducted a survey of patient satisfaction in those patients receiving insulin only versus insulin plus pramlintide after 29 weeks. 29 Patients in the test group felt that pramlintide helped control weight gain and appetite as well as facilitate activities of daily living. They believed that the benefits of pramlintide outweighed the downside of the extra injections daily and would recommend this therapy to other patients. In light of the patient satisfaction described above, there is a potential niche for pramlintide among insulin-dependent patients with type 1 and 2 diabetes who are either unable to achieve euglycemic states with insulin alone or are frustrated by insulin-induced weight gain.
Recently, Heptulla et al. demonstrated the role of continuous subcutaneous replacement of amylin and insulin for a 24-hour period on glucose control in adolescents with type 1 diabetes. They hypothesized that pre and postprandial amylin replacement would normalize blood glucose concentrations. Their study compared continuous subcutaneous insulin monotherapy (part A) with continuous subcutaneous insulin and pramlintide infusions (part B). In part B, the prandial insulin boluses were reduced by 20%. The basal and prandial pramlintide were administered simultaneously using another pump, and the boluses were given as dual-wave boluses with 70% of the dose given immediately and 30% over the next hour. The patients on dual therapy showed a 26% reduction in postprandial hyperglycemia compared to the patients on insulin monotherapy. 31
Additional potential roles for pramlintide include monotherapy or adjunct therapy to other medications for weight loss. In a recent clinical observation study of overweight and obese subjects, the coadministration of metreleptin and pramlintide acetate for 20 weeks elicited significantly more weight loss (approximately 13%) than either treatment alone. 32 In a randomized 24-week single-blind study, the combination of pramlintide with sibutramine or phentermine led to a significant increase in weight loss (approximately 11 kg) when compared with pramlintide monotherapy (approximately 4 kg). 33
In summary, pramlintide is an amylin analog that plays a role in adjunct treatment of both type 1 and type 2 diabetes. Although it has only a modest effect on HbA1C reduction, pramlintide does appear to lessen post-prandial glycemic excursions and has a favorable effect on weight. The main limitation in the use of pramlintide is the necessity of additional subcutaneous injections in individuals who are already injecting upwards of four times daily. However, Riddle et al. showed that pramlintide may also potentially be used as an alternative to mealtime insulin in patients who are not adequately controlled on basal insulin. As pump technology improves and allows for injection of both insulin and pramlintide, one might predict that pramlintide will become even more appealing, especially in individuals with type 1 diabetes. Future considerations are likely to include the use of continuous subcutaneous pramlintide as well as dual-wave boluses of pramlintide to combat early postprandial hypoglycemia and late postprandial hyperglycemia. At that point, it will be important to conduct additional studies to examine both the long-term effects of pramlintide and also the effect of this medication on the development of diabetes-related complications. Other potential uses of pramlintide, including its potential role as a weight loss agent, continue to require further study.
Disclosure
The authors report no conflicts of interest.