
Abstract
Rosiglitazone is a member of the Thiazolidinedione class of drugs with a potent insulin sensitizing action. The drug has been extensively used and many early warnings on its potential risks were ignored mostly due to an aggressive commercial strategy. In 2007 some papers raised doubts on the cardiovascular safety of the drug and started a serious dispute. Irrespective of the real existence of this risk the story of Rosiglitazone led to the unveiling of many other side effects and emphasizes the need for a more accurate evaluation of any drug before is approved by the regulatory authority.
The story of Rosiglitazone can be conveniently divided in 2 periods, before and after a controversial paper by Niessen. 1 This paper changed the attitude of many physicians towards the drug. Furthermore this paper paved the way for an unremitting discussion among medical professionals and scientists on the role of the pharmaceutical companies and the use of surrogate end points. A simple search of Pub Med with the word “Rosiglitazone” returned 2753 titles.
It is probable that all the uncertainty concerning the use of this drug and its possible risks derive from the ruthlessness of the producer, trying to find an all inclusive marketing position for the molecule. Unfortunately this led to the widespread and unwary prescription of the drug.
When Rosiglitazone entered the market was under the unfortunate legacy of its predecessor, Troglitazone (Rezulin), which the FDA withdrew due to unwanted hepatic side effects on 08-08-03.
2
Mechanism of Action
Rosiglitazone belongs to the thiazolidinedione (TZD) class of antidiabetic agents and improves glycemic control by improving insulin sensitivity. The drug is an extremely selective and potent agonist of the peroxisome proliferator-activated receptor-gamma (PPARγ). In humans, these receptors are located in key target tissues for insulin action such as adipose tissue, skeletal muscle, and the liver. The activation of PPARγ nuclear receptors regulates the transcription of insulin-responsive genes involved in the control of glucose production, transport, utilization and regulation of fatty acid metabolism, but this list may well be not all inclusive and unfortunately no other possibly untoward effects can be excluded with certainty. Rosiglitazone reduces blood glucose concentrations and reduces hyperinsulinemia in the experimental animal through increased sensitivity to insulin's action in the insulin dependent tissues. Part of this action is mediated by an increase in the insulin-regulated glucose transporter GLUT-4 in the adipose tissue. Rosiglitazone is predominantly metabolized by Cytochrome P450 and is more than 99% bound to plasma proteins, primarily albumin.
In monotherapy studies, a greater therapeutic response was observed in females and this can be explained on the basis of the greater fat mass since PPARγ, the molecular target of Rosiglitazone is expressed in adipose tissue. In more obese patients, gender differences were less evident. Rosiglitazone can be administered with or without food.
Hepatic Impairment
Oral clearance of Rosiglitazone was significantly lower in patients with moderate to severe liver disease (Child-Pugh Class B/C) compared to healthy subjects. Elimination half-life for Rosiglitazone was about 2 hours longer.
Significant drug Interactions have been demonstrated for drugs that inhibit, induce, or are metabolized by Cytochrome P450. To the contrary a single administration of a moderate dose of alcohol did not increase the risk of acute hypoglycemia in type 2 diabetes mellitus patients treated with Rosiglitazone.
The Debate on the Safety of Rosiglitazone
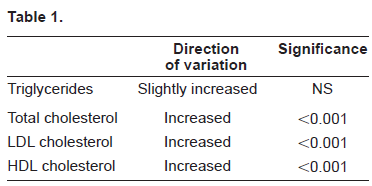
Before the metanalysis of Niessen, mostly according to the laws of the market, there has been a flurry of publications in favor of the beneficial effects of Rosiglitazone. This in part reflects the current trend to push the drugs on the market before there is definitive clinical proof of effectiveness and safety, and this also holds true for the recently marketed Ezetimibe. 3 In 1998 a beneficial effect of Rosiglitazone on the pancreatic β cells in Zucker rats, a strain of obese rats with insulin resistance, altered β cell morphology and a marked tendency to develop diabetes was demonstrated. 4 On the basis of some experimental data the hypothesis was generated that such beneficial effect could occur also in the human pancreas.5–6 One of the most intriguing observations is that Rosiglitazone can re-entrain the disrupted insulin pulsatile secretion of type two diabetics, a fact too often overlooked. 7 In one study by Lupi et al 8 Rosiglitazone prevented the Free Fatty Acid (FFA) induced functional damage to β cells in vitro. However the main effect of Rosiglitazone is its action on insulin resistance, mediated through the affinity with the PPARγreceptor in insulin sensitive cells. Rosiglitazone binds to PPARγ 9 acting on the expression of the molecules involved in insulin signaling and glucose transport systems. 10 Rosiglitazone is a potent member of the Thiazolidinedione class, with a binding affinity for PPARγ that is 100-fold greater than that of Pioglitazone and 190-fold greater than that of Troglitazone. 11 This is indirectly confirmed by the greater response to the treatment of the obese subjects with the more pronounced markers of insulin resistance. 12 The great power of Rosiglitazone as an insulin sensitizing agent is probably the basis for its efficacy in PCOD,13,14 a condition of severely reduced insulin sensitivity. The same mechanism holds true for psoriasis and other diseases in which insulin resistance is prominent. 15 The drug has bees recently demonstrated to be useful in Alzheimer's disease with an uncertain mechanism. 16 The effect of Rosiglitazone on the lipid pattern in the body has been explored in comparison with Pioglitazone, 17 and is summarized in Table 1.
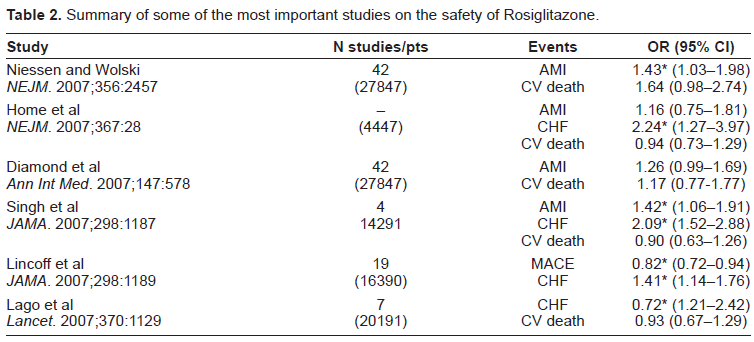
Summary of some of the most important studies on the safety of Rosiglitazone.
Rosiglitazone significantly increased the total VLDL particles and all the subfractions, large, medium and small, increased the LDL particles and caused a minor and nonsignificant decrease in number of the small LDL particles. The HDL particle number was also slightly decreased. Furthermore Freed et al demonstrated an increase in total plasma and LDL apoB lipoproteins with Rosiglitazone treatment. 18
In summary Rosiglitazone was associated with unfavorable variations in the lipid pattern. In the same study Pioglitazone performed much better with the lipid profile. It should be noted however that this elegant study was protracted only for 6 months, and in the longer run the results might have turned out different. Substantially similar results were obtained in a smaller study of shorter duration, 19 and it is likely that these adverse changes in the lipid pattern have a bearing on the cardiovascular effects of the drug.
Contrary to its negative effects on the lipid profile Rosiglitazone performs very well on the blood glucose control and this is largely expected in view of its potency. In a study in which Rosiglitazone or placebo were added on top of insulin 20 HbA1c decreased >0.7% or > 1% on 4 and 8 mg daily dose respectively. However the change in HbA1c is a poor surrogate for cardiovascular outcomes in Type 2 diabetes, accounting for only 5 to 15% of the reduction in ischemic risk. 21 Rosiglitazone has been used in various settings and combinations, even too many and in 2006 nearly 37% of the market share of the oral euglycemic medications was held by Rosiglitazone. 22 One indication widely accepted in the U.S.A is in association with insulin, 12 although this may pose additional risks.
The turning point of the fortune of Rosiglitazone was the publication of the data from the metanalysis by Niessen in 2007, 1 but this is only the tip of the iceberg. Niessen and Wolski in their paper conclude that “Rosiglitazone was associated with a significant increase in the risk of myocardial infarction and in the risk of death from cardiovascular causes with borderline significance”. However this paper deserves a closer scrutiny: a metanalysis is fraught with methodological difficulties. In this case the inclusion criteria were a study duration of >24 weeks, the use of a control group not receiving Rosiglitazone, and the availability of outcome data for myocardial infarction or death for cardiovascular causes. Throughout these studies the inclusion/exclusion criteria were not the same, and both protocols and drug dosages were different. The authors included all these studies because the Cochrane Q test, used to test the heterogeneity across the trials gave a p > 0.1 nominal value. However it should be considered that the Q test is a questionable choice in these circumstances. 23 Furthermore the authors could not obtain the original data and were not able to discern whether the same patient had both events, acute myocardial infarction and death, and in all these studies except the DREAM study the criteria for adjudication of myocardial infarction or death from cardiovascular causes were not reported. They could not obtain time to event and data for cardiovascular accidents and Strokes were not reported. A look at table 1 of their paper (clinical trials included in the metanalysis) discloses that at least 4 included subjects treated with Rosiglitazone plus insulin, a total of 918, and the association of these two drugs carries such a high risk that even if allowed by the FDA was not accepted in other countries. From the same table is apparent that one study targeted subjects with Alzheimer's disease (study AVA100193 n = 124) and two subjects with psoriasis (Study 49653/234, n = 61 and 4965/331, n = 325) who did not have diabetes. Of greater concern is the inclusion of study 49653/211 (n = 114) with subjects having congestive heart failure, a condition that in itself is a contraindication to the use of Rosiglitazone. As expected this group of subjects had the greatest number of myocardial infarctions (five) and deaths from cardiovascular causes (three). Forty-eight studies were originally included in the metanalysis, but six were discarded because did not report any myocardial infarction or death from any cardiovascular cause. We do not know more details on these studies, but the exclusion, warranted or not, certainly weighted on the results against the safety of Rosiglitazone. Among the remaining 42 studies 26 were unpublished and we do not know why, and if they were peer reviewed. The studies included came from three sources, 1-submitted to the FDA for approval, 24 2-from the Glaxo_SK clinical trial registry, 25 3-ADOPT and Dream trials.26,27 None was designed to evaluate the cardiovascular effects of the drug. When we examine the results we see that the odds ratio for myocardial infarction was 1.43 in the Rosiglitazone group (CI = 1.03-1.98, P = 0.03) and 1.64 (0.98-2.74, p = 0.06) for death from cardiovascular causes. The CI of this second value is extended across the unit and is barely acceptable as significant. The authors had to use the Odds Ratio (OR) because they did not have the time to event data, but the OR may not be the best way to represent the risk at an individual level. It should also be observed that in those trials in which Rosiglitazone was compared to placebo there was statistical difference in risk of Myocardial ischemic events, but the difference disappeared in those studies in which was compared to an active diabetes drug. There are many more consistent objections to the validity of the paper by Niessen and are elegantly clarified in a paper in Annals of Internal Medicine. 27 These authors conclude that the risk for myocardial infarction and death from cardiovascular disease for diabetic subjects taking Rosiglitazone is uncertain: “Neither increased or decreased risk is established.”
Prompted by this paper there was a flurry of publications. Home et al conducted an interim analysis of the RECORD trial
29
that was specifically designed to measure the effects of treatment with Rosiglitazone plus Metformin or Sulfonylurea on cardiovascular outcomes, and was planned with the interventions of some employees of the Glaxo-Smith-Kline, which may be a cause for concern, and could not confirm the excess of cardiovascular problems for Rosiglitazone. However as Nathan points out
30
during the RECORD trial there was an unexpected high rate of drop out and a low rate of cardiovascular accidents that left the study underpowered at the time of the interim analysis. Furthermore the comparator drug was a combination of Metformin plus Sulfanylurea a that was associated with 96% increase in mortality among the diabetics in the UKPDS study.
31
Third at the time of the interim report
29
the curves of the cumulative incidence for the adjudicated primary events became separated in disfavor of Rosiglitazone from the 24th week up to the 60th, although the difference is not statistically significant. In addition looking at panel B that compares the adjudicated
Another metanalysis was published in September 2007 32 with more stringent criteria, using only trials specifically intended to monitor cardiovascular adverse events and the pooled data from 14291 diabetic subjects showed that Rosiglitazone significantly increased the risk of Acute Myocardial Infarction (RR 1.42 p = 0.02) versus control and of heart failure versus placebo (RR = 2.09, p < 0.001). There was no significant increase in the risk of cardiovascular mortality (RR = 0.9, p = 0.53).
More recently an interim analysis of the data of the Veterans Administration Diabetes Trial (VADT) designed to study tight blood glucose control and cardiovascular disease (CVD) risk in Type 2 diabetes, not yet published, was presented at the June 2008 ADA Scientific Sessions. The VADT was not designed to test the effect of one single drug, and thus Rosiglitazone was used in the intensive and conventional arm of the study. The Authors used a case control design and a time dependent covariate survival analysis that allowed them to calculate the Hazard Ratio rather than the Odds ratio. Of the 1791 subjects enrolled in the VADT study 16% (=297) received at any time point 4 mg/day of Rosiglitazone, and 79% (=1408) received 8 mg. The Authors conclude that there is no evidence that the use of Rosiglitazone increases the risk for cardiovascular mortality or morbidity in patients with type 2 diabetes mellitus. It should be mentioned that Glaxo Smith Kline had no role in the analysis or the presentation of the data.
On July 30 2007 the FDA Advisory Committee listened to a testimony by the Health Research group of Public Citizen that concluded that” 33 the evidence presented justifies the removal of the drug from the market, and due to the ubiquitous nature of PPRγ receptor sites in so many parts of the body it is hardly surprising that there are many other significant kinds of damage this drug is causing to patients.” During this testimony the HRG called attention to many other important side effects of the drug, viz. anemia, liver toxicity, peripheral oedema, heart failure, extremity fractures, macular oedema threatening vision, and increase in weight. It must also be emphasized that as far as 1999 in a pharmacology review of animal toxicity “Rosiglitazone produced various toxicities such as left atrial thrombosis, hydrothorax, cardiac hypertrophy and elevations of hepatic enzymes in the high dose group,” In the reviewer's opinion “it is not possible to anticipate potential human toxicities” … “these findings appear as long term clinical concern.”
The FDA adverse reaction reports filed since marketing to the end of 2006 lists 698 cases of heart failure with Rosiglitazone compared with 39 for the older diabetes drugs, although a greater alertness to glitazones may have played a role in this reporting. After adjusting for differences in the number of prescription for the 2 drugs the rate of heart failure reports for Rosiglitazone compared with Glucotrol was 15.2 times higher. 34
The unexpected effect on fractures first appeared in the ADOPT Study: 28 more specifically 60 women, (9.3%) in the Rosiglitazone group had fractures versus 30 (5.08%) in the Metformin and 21 (3.47%) in the Glyburide group, both p < 0.001 in comparison with Rosiglitazone. If ever one should have expected more broken bones in the Glyburide group more prone to hypoglycaemia. There was no statistically significant difference in men. The mean age of the female subjects in the Rosiglitazone group was 56.3 ± 10, thus there is a prevalence of postmenopausal women, and intriguingly the excess fractures were distally located (upper limb: humerus and hand; lower limb: foot), which is extremely uncommon in this age group and as such adds value to the observation. However in a case control study involving an older female population (60% of participants being over 60 y.o.) the fractures of hip and femur were significantly associated with thiazolidinedione therapy. 35 There are indications that higher levels of sex steroids are protective in men. 36 A recent metanalysis 37 revealed that for women of mean 55 years of age the 1-year number of subjects treated needed to harm is 55, and this figure decreases to 31 and 21 respectively at mean age 65 and 72. In the same paper the authors calculate that an excess 30000 fractures may have occurred out of 2 million thiazolidinedione users for more than one year. Among the proposed mechanisms of this effect are osteoclast differentiation, bone reabsorption38–41 and a negative effect on PTH.42,43
There is evidence that concerns had been raised much earlier and probably were ignored by the FDA. A memorandum from the Department of Health and Human Services, Public health Service, and FDA: Center for Drug Evaluation and Research 34 dated 07/16/2002 states that “data from this series provide evidence that TZD (Thiazolidinedions) may be associated with Hearth Failure to an extent not clearly defined in the product label.” 44
Personal Experience
We treated 189 subjects with Rosiglitazone from the introduction in our market, and this amounts to 1.2% of our type 2 diabetic population and is the same as throughout the country. From the start we were very cautious with the drug and monitored the fluid accumulation with the Body Impedance Analyzer and warned that if the fluid expansion in both the intra or extracellular compartment exceeded 2 liters the risk of heart failure could be very high. 45 Using this technique we only had one case of heart failure rapidly resolved upon suspension of the drug.
We also retrospectively evaluated our subjects for cardiovascular problems (mean 18 ± 4 months) and found only 2 episodes of angina, and no distal limb fractures (unpublished observation). Although we had no control group and thus this observation must be interpreted as it is, it is worth to mention that we used Rosiglitazone only in subjects under 50 years old, with a short duration of disease and monitored them closely. Furthermore we never used Rosiglitazone together with insulin. In this direction it is worthwhile noting that a further analysis of the Niessen's data demonstrates that while the risk difference of cardiovascular events for the overall populations was 1 event per 100-patient-years, in a high risk subgroup where Rosiglitazone was used with insulin the risk difference was 3 events per-100 patients-ys. Furthermore a subgroup analysis presented at an FDA staff Hearing on July 30, 2007 suggested that the risk of ischemic events with Rosiglitazone may be potentiated with the concurrent use of insulin or nitrates (
Conclusions
The data presented here and the numerous studies in the literature unfortunately do not resolve conclusively the doubts on the safety of Rosiglitazone. However there is sufficient evidence to raise concern and since there is the availability of other effective drugs it is difficult now to use Rosiglitazone lightly. The Glitazones are difficult drugs, yielding much less than they require in terms of cost, need for control of and incumbent risks. If Rosiglitazone is to be used at all probably should be limited to young people of male sex, with a short duration of disease, without any risk factor for cardiovascular disease, and planning for a close follow up of blood lipid levels, fluid accumulation, body weight and liver enzymes. In addition one should not forget that the PPARs have complex biological activity interacting with many genes and at present the effects of these interactions are not known. Nearly 50 investigational PPAR drugs have been filed for application unsuccessfully. It is very difficult at present to find a place for Rosiglitazone. In a recent poll at a website 49 asking professionals if Rosiglitazone should be removed from the market 56% of the respondents answered Yes, 44% no.
Disclosure
The author reports no conflicts of interest.