
Abstract
Hepatocellular carcinoma (HCC) is the fifth most common malignancy worldwide with approximately 500,000 new cases per year, ranking as the third cause of cancer deaths. Until the very recent past no systemic therapy was available for patients with advanced HCC. However, advances achieved in the understanding of the molecular cancer biology and the subsequent introduction of molecularly targeted agents have disclosed promising and interesting possibilities for the treatment of this highly vascularized tumor in which the inhibition of angiogenesis is likely to represent the main potential therapeutic target. In this regard, sorafenib, an oral multikinase inhibitor endowed with significant activity against several tyrosine-kinase receptors involved in blood vessel development, has shown to be very active in the treatment of advanced HCC. This review makes a survey of pharmacology, mode of action, pharmacokinetics, clinical value and safety of sorafenib when employed in the treatment of advanced HCC.
Introduction
Hepatocellular carcinoma (HCC) represents one of the leading solid organ malignancies worldwide, accounting for 6% of all tumor types. Approximately 60% to 80% of incidence relates to its common association with cirrhosis from heavy and long-lasting alcohol consumption, chronic hepatitis virus infections (hepatitis B virus [HBV] in Asia and Africa and hepatitis C virus [HCV] in the Western countries), and aflatoxin exposure. Consequently, the management of this tumor becomes even more difficult because of the presence of this underlying liver disease.1,2 Surgery is the mainstay of HCC treatment 3 but at presentation, more than 80% patients present with multicentric HCC and advanced liver disease or comorbidities that restrict the therapeutic measures to BSC. 4 As far as the treatment of advanced disease is concerned, to date no single agent or combination chemotherapy have demonstrated any advantage in terms of both overall survival and quality of life. Also the hepatic arterial infusion and chemoembolization, which in some instances resulted in an increase of response rate, did not show any benefit in terms of overall survival. 5 Lastly, no treatment has been identified for severe advanced disease whose prognosis is very poor and is measured in months. 2
In the very recent past, however, the significant advances achieved in the understanding of cell-cycle regulation and tumorigenesis have identified new targets for therapeutic intervention and have disclosed new and very promising perspectives for the treatment of this disease. In particular, the potential targets for HCC include the vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), and hepatic/c-met signalling pathways. Neovascularization is one of the most important factors and there is a close relationship between VEGF expression and HCC vascularization compared to non-cancerous liver tissue. 6 It has been demonstrated that VEGF is overexpressed in HCC and correlates with a decrease in disease-free survival and overall survival, and with an increase of portal-vein invasion which are associated with later stage of disease, high grade and poor prognosis. Moreover, it has been observed that also Ras mutations are overexpressed in HCC tumors6–8 demonstrated that dual inhibition of Raf and VEGFR2 reduces cells growth and vascularization of hepatocellular carcinoma in experimental model. 9
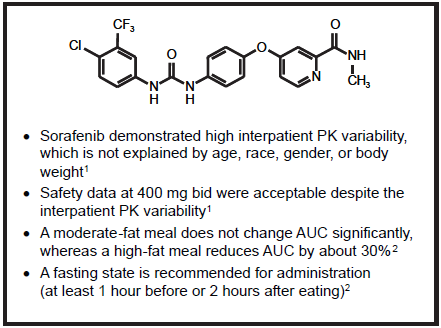
Structural formula and pharmacokinetic properties of Sorafenib.
Sorafenib (Nexavar®, Bayer/Onyx), an oral mutikinase dual-action inhibitor able to target Raf kinase and vascular endothelial growth factor receptors so preventing both tumor cell proliferation and angiogenesis, has been extensively studied in HCC. Following a series of preclinical and clinical studies carried out in this tumor type which clearly demonstrated a high level of activity, the unquestionable results of two pivotal randomized phase III clinical trials have acknowledged sorafenib as the only and the unique drug presently available and recommended for the treatment of advanced HCC.5,10 This review summarizes the main characteristics of sorafenib running through the series of results achieved in the management of HCC.
Pharmacology, Mode of Action and Pharmacokinetics of Sorafenib
Due to the lack of understanding of the molecular mechanisms underlying tumorigenesis, cytotoxic chemotherapy has represented for many years the only medical approach to cancer treatment. 7 In the last decades of the past century, however, advances in molecular biology have led to the identification and characterization of genetic elements (gene mutation, gene amplification and/or overexpression) whose normal function is to control cell growth and/or differentiation, which, when altered, play a fundamental role in human cancer pathogenesis. This occurs through the activation of abnormal complex signaling networks mainly involving growth factors receptors and signal-transduction pathways. Consequently, large drug discovery programs have been activated and devoted to the identification of biologically specific therapies able to target the cancer-specific pathways, 1 also in the assumption that the new targeted agents, theoretically sparing normal cells, could provide a higher therapeutic index on account of better safety benefits over the standard cytotoxic chemotherapy. 7
The first proof of concept that gene is a valid anticancer target goes back to 1989 when it was demonstrated that the disruption of
Early investigations carried out in cell lines have shown that sorafenib directly inhibits downstream Raf kinase isoforms (wild-type Raf1, B-Raf and mutant b-raf V600E). The subsequent discovery that the drug is also able to block the autophosphorylation of several tyrosine-kinase receptors such as VEGFR1, 2 and 3, PDGFR, c-Kit and RET, has led to the settlement that sorafenib is a dual-action drug capable to inhibit both tumor-cell proliferation and tumor angiogenesis. 7 It is likely that the mechanism of action of this drug has not yet been completely elucidated since, as it has been demonstrated in a wide range of tumor models, it seems able to increase also the rate of apoptosis.11,12
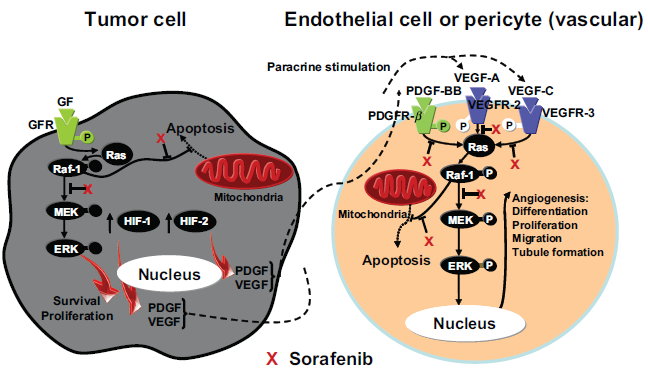
Sorafenib targets both tumour-cell proliferation and angiogesis. Wilhelm S, et al.
Starting from the very early stages of the disease, HCC appears as a complex heterogeneous hypervascular tumor in which the overexpression of proangiogenic factors like VEGF, PDGF and angiopoietin-2 has been largely demonstrated. Experimental studies have shown that targeting angiogenesis is a top priority objective in this tumor in which vascular endothelial growth factor (VEGF) is responsible for the enhancement of development and of metastases.13,14 Besides that, there is evidence of aberrant activation of several signaling cascades such as EGFR, Ras/extracellular signal-regulated kinase, phosphoinositol 3-kinase/mTOR, hepatocyte growth factor/mesenchymalepithelial transition factor, Wnt, Hedgehog, and apoptotic signaling. 8 Additionally, the HCV core proteins, frequently involved in cellular transformation, elicit high basal Raf-1 activity in hepatocytes thus increasing the risk of neoplastic conversion.15,16 Therefore, on account of its ability to inhibit angiogenesis and RAF kinase pathway, sorafenib has been identified as a suitable and ideal candidate for studies in HCC.
The pharmacokinetic evaluation of sorafenib in humans was carried out in 60 patients with advanced refractory solid tumors by testing single and repeated orally administered doses of the drug ranging from 100 to 800 mg bid. Notwithstanding an inter-individual variability of the pharmacokinetic profile likely due to different individual levels of absorption of the drug and/or of entero-hepatic circulation, results showed that there was no dose-dependent relationship in pharmacokinetic parameters when testing the doses of 400, 600 and 800 mg considered as the therapeutic ones. Maximum mean values of AUC and Cmax were reached between 2.5 and 12.5 hours following the administration of a single dose of 600 mg bid, with only marginal differences as compared to the dose of 400 mg bid. 17 Further increase of the dose to 800 mg bid did not result in any increase of the AUC0-12 and Cmax values. Substantial accumulation of sorafenib in plasma (2.5 to 7-fold) has been observed after repeated administrations: steady-state plasma concentrations were achieved after seven days.17–19
Food intake before dosing slightly modifies the pharmacokinetic parameters: on the contrary, the fat content of the meal seems to have some influence.18,19 Mean AUC and Cmax values are reduced of about 29% and 38% respectively when sorafenib is administered following a high-fat meal, while an increase of about 14% of the AUC and a decrease of 17% of Cmax have been observed when sorafenib is given with a moderate-fat meal. 19
Sorafenib highly binds to plasma proteins (99.5%) with a binding affinity which is linear and independent of the drug concentration.
19
It primarily binds to serum albumin and, to a lesser extent, to α-globulins, β-globulins and LDL, while does not bind to γ-globulins and α1-acetic glycoprotein.
20
Metabolism of sorafenib has been extensively evaluated both in
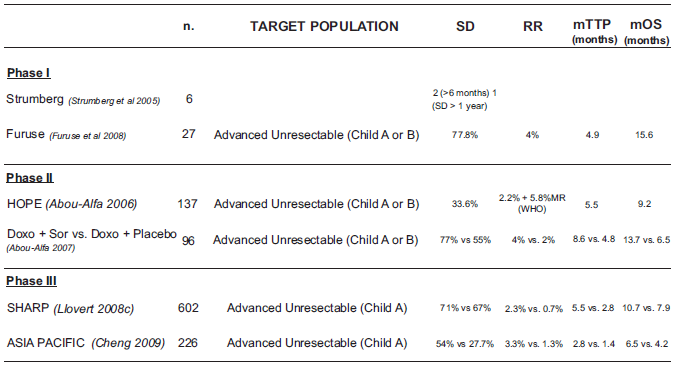
A summary of all phases clinical studies of Sorafenib in HCC.
Studies
Efficacy Studies
Preclinical studies
Notwithstanding sorafenib was initially recognized as a CRAF inhibitor, 23 additional studies have also demonstrated that it is a potent inhibitor of other kinases such as BRAF (wild-type and mutant), VEGFR2, VEGFR3, PDGFR-β, FLT3, Ret and c-Kit.23,24 This evidence clearly appeared in preclinical models where a dose-dependent activity against a wide range of tumor types, including HCC, in terms of cell-growth inhibitory effects, induction of apoptosis, and down-regulation of the antiapoptotic protein Mcl-1 through a Raf/MEK/ERK-independent mechanism was observed.11,24
As far as HCC is concerned, preclinical studies have demonstrated that Raf/MAPK-ERK kinase (MEK)/extracellular signal regulated kinase (ERK) pathway plays an important role. The over-expression of activated MEK1 in HCC cell lines, which enhances tumor growth and survival by preventing apoptosis, suggested that targeting the MEK signalling pathway could be an appropriate approach to the treatment of HCC.25,26 An evaluation of the direct effects of sorafenib carried out
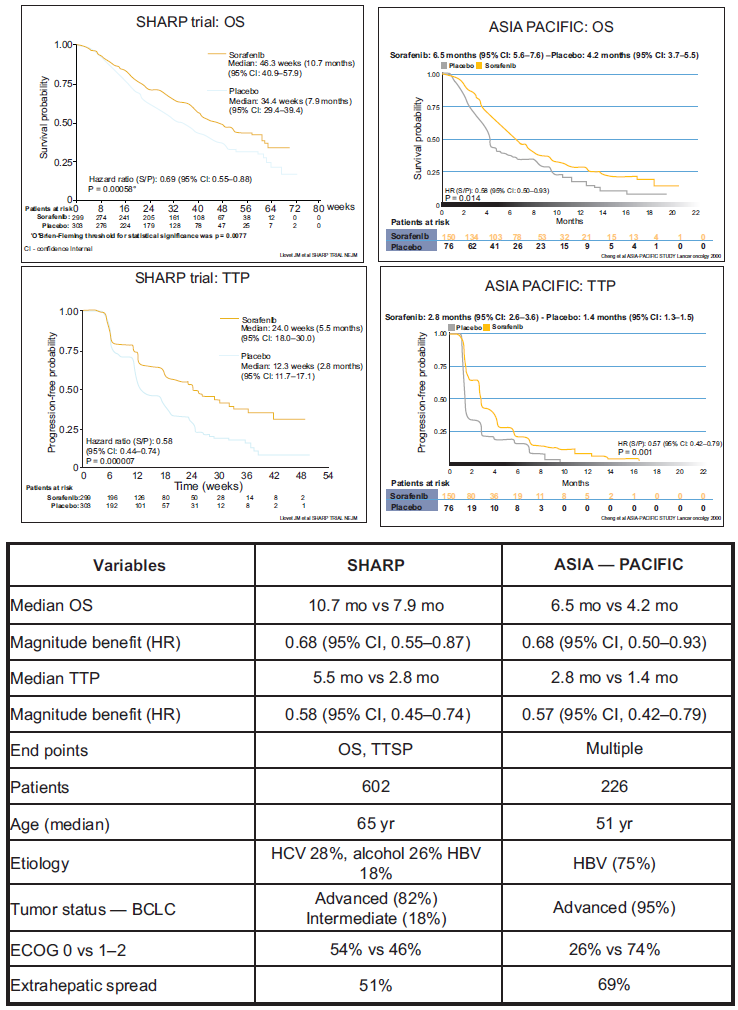
Comparison between the two phase III studies of Sorafenib in HCC: SHARP trial and ASIAN-PACIFIC trial.
Clinical studies
Preliminary remarks
Since in most cases of HCC the concomitant presence of cirrhosis substantially affects the evaluation of the stage of the disease and, afterwards, the choice and the outcome of treatment, the measure of the extent and severity of hepatic dysfunction represents a crucial aspect which cannot be left out. Consequently, the TNM cancer staging system cannot be considered adequate and satisfactory to properly define a situation resulting from the concurrence of quite a lot of factors. Therefore, several systems for a better definition of the stage of the disease and prognosis have been proposed. Even though in a retrospective analysis of patients with advanced HCC carried out by the Memorial Sloan-Kettering Cancer Center the CLIP (Cancer of the Liver Italian Program) and GRETCH (GRoupe d'Etude et de Traitement du Carcinoma Hépatocellulaire) scoring systems seemed to satisfactorily fulfill the requirements for a valid definition, 2 nowadays the Barcelona-Clinic Liver Cancer (BCLC) classification, which links tumor stage with treatment strategy, has been acknowledged and endorsed by AASLD (American Association for the Study of Liver Diseases) and EASL (European Association for the Study of the Liver) as the standard one for clinical management of HCC. 3
Another very important aspect, which deserves to be clarified and which calls for the choice of new more suitable and reliable alternatives so far not yet undeniably identified and still matter of evaluation and discussion, relates to the assessment of tumor response when using the molecularly targeted agents. Likewise other targeted agents, in all studies carried out with sorafenib in different tumor types RECIST (Response Evaluation Criteria in Solid Tumors) criteria, which grade the tumor response on the basis of the extent of tumor shrinkage, have been used: this resulted in a rather limited rate of complete and/or partial responses and in a striking rate of stable diseases. This goes off because the RECIST criteria, originally developed to assess responses to cytotoxic drugs, are not appropriate as indicators of activity of sorafenib and of other targeted agents whose mechanism of action lies in a block of cell growth without necessarily inducing cell lysis. As a matter of fact, tumor scans have shown that most cases graded as stable disease on the basis of the lack of tumor shrinking represent on the contrary a consistent response to treatment as a necrotic area inside the tumor burden, usually spreading from centre to the periphery, has developed.
Phase I
Two single-agent phase I trials 27 evaluated sorafenib at doses ranging from 50 to 800 mg/day in 69 and 27 patients with a variety of advanced refractory solid tumors. Among 6 evaluable patients with HCC, 2 stable disease lasting >6 months, 1 stable disease lasting >1 year and 1 partial response >6 months have been observed. Even if the majority of patients experienced at least one adverse event, the grades of toxicities were mostly mild to moderate. 18
Another phase I single-agent disease-oriented trial was carried out in 27 Japanese patients with advanced unresectable HCC (Child–Pugh class A or B). They received at first a single dose of sorafenib of 200 mg (n = 13) or 400 mg (n = 14) followed by a 7-day rest period: subsequently, the same doses of sorafenib (200 or 400 mg bid) have been administered for 28 consecutive days in 4-week cycles. Out of 27 patients evaluable for efficacy, of whom 10 treated with 200 mg bid and 11 with 400 mg bid, 1 (4%) achieved a partial remission (PR) and 21 (77.8%) had stable disease (SD) evaluated according to RECIST criteria. Median Time To Progression (TTP) was 4.9 months. Median Overall Survival (OS) in all intent-to-treat 27 patients was 15.6 months. The authors concluded that, in Japanese patients with advanced HCC, sorafenib at the doses of 200 mg and 400 mg bid is generally well tolerated showing a consistent anti-tumor activity. 22
An open-label, uncontrolled, phase I trial evaluating the combination of sorafenib with doxorubicin also showed a good level of efficacy of this regimen in the treatment of patients with advanced HCC. 28
Phase II
An open-label, multicentre, phase II trial evaluating sorafenib single agent at the dose of 400 mg bid continuous dosing was carried out in 137 previously untreated patients with advanced, inoperable HCC Child–Pugh class A or B. The evaluation of patients on the basis of an independent assessment showed PR in 3 (2.2%) patients, minor responses in 8 (5.8%) and SD lasting for at least 16 weeks in 46 (33.6%). Median TTP was 5.5 months and the OS was 9.2 months. 1 The latter figure appears particularly interesting since it compares favorably with those of other studies evaluating combination regimens with conventional cytotoxic agents (PIAF [cisplatin, interferon alpha-2b, doxorubicin, fluorouracil] or doxorubicin plus cisplatin) in HCC patients2,3 where median overall survival rates accounting for 8.9 and 7.3 months respectively have been reported. 1 In addition, in a small group of patients (33), pretreatment tumor phosphorylated ERK (pERK) levels have been correlated with the TTP: results show that patients who had tumors expressing more intense pERK staining had also a longer TTP. 1
Another phase II, randomized, double-blind, placebo-controlled study evaluated the combination doxorubicin + sorafenib
Phase III
Two pivotal large phase III trials have been carried out to definitely assess the efficacy and safety of sorafenib in advanced HCC.
The study SHARP (
The ASIA-PACIFIC study is an international phase III, multicentre, randomized, double-blind, placebo-controlled trial which has evaluated sorafenib
Differently from the SHARP trial, the main etiological factors in this study were Asian ethnicity and hepatitis B virus. Following stratification according to macroscopic vascular invasion and/or extra-hepatic spread, ECOG PS and geographic region, patients have been randomized in a 2:1 ratio either to sorafenib 400 mg bid (n = 150) or to placebo (n = 76) treatment. Study endpoints included OS, TTP, PFS, TTSP, disease control rate (CR + PR + SD ≥ 6 weeks) and safety. The primary endpoint was not defined. Similarly to SHARP study, also the ASIA PACIFIC trial showed a superiority of sorafenib as compared to placebo in terms of OS, PFS, TTP and disease control rate, further demonstrating the efficacy of this drug also in patients with different ethnicity and different leading etiological factors. Results, reviewed and validated by an independent DMC, indicated statistically significant differences as regard TTP (2.8 months for sorafenib
Safety
Similar rates of drug-related adverse events in terms of both incidence and category, the most common being represented by dermatological, constitutional and gastrointestinal symptoms, have been observed in the phase II and phase III studies carried out in patients with advanced HCC treated with sorafenib1,5,10 In the large open-label phase II study where 137 patients have been treated, no grade 4 drug-related adverse events have been observed. As for the grade 3 events recorded in ≥10% of all patients, they accounted for 5.1% hand-foot skin reactions (HFSR), 0.7% rash/desquamation, 9.5% fatigue, 8.0% diarrhea, 1.5% anorexia and 0.7% stomatitis.
In the phase III SHARP trial, the overall incidence of adverse events of any grade and from any cause was 80% in the sorafenib group and 52% in the placebo group; they mainly consisted of gastrointestinal, constitutional and dermatologic symptoms. On the contrary, the overall incidence of serious adverse events from any cause was similar in the two study groups accounting for 52% in the sorafenib group and 54% in the placebo group: in relation with the particular features of the disease they were mainly represented by hepato-biliary events (11% and 9%, respectively), hemorrhagic events (9% and 13%), variceal bleeding (2% and 4%), renal failure (<1% and 3%). The most frequent drug-related grade 3 adverse events included diarrhea (8% in the sorafenib group
The drug-related adverse events recorded in the ASIA-PACIFIC study are in line in terms of incidence and category with those observed in the SHARP study, being the grade 3-4 represented by HFRS (11%), diarrhea (6%), fatigue (9%), and hypertension (2%).
Worth nothing is the fact that, with exception of the hepatobiliary adverse events strictly related to the presence of liver disease, all the drug-related events appeared in the studies on HCC correspond in terms of both incidence and type to those gathered when using sorafenib in other studies in different tumor types such as the treatment of renal cell carcinoma e.g. phase III TARGET study. 30
It is likely that some adverse events typical of sorafenib and of other targeted agents could be related to the particular mechanism of action of these drugs. Dermatological toxicity, HFRS in particular, represents one of the major features following the treatment with sorafenib: the mechanism of onset has not yet fully understood but almost certainly we are dealing with a side effects strictly connected with the anti-kinase activity.2,3 Analysis of cumulative event rate from the phase III pivotal studies carried out with sorafenib in all tumor types suggests that rash and HFSR usually appear during the first 6 weeks of treatment with sorafenib and they get worse as the treatment goes on. 30 Management of these dermatologic toxicities may include topical therapies for symptomatic relief, temporary treatment interruption and/or drug dose modifications, or, in case of increase of severity or persistence, permanent discontinuation of sorafenib.31–33 In rare instances, yellow skin discoloration, mainly on hands and feet, has also been observed during sorafenib treatment: however, generalized skin discoloration has not been reported. 34 Also the increase of incidence of arterial hypertension seems to be related to the mechanism of action of tirosyne-kinase inhibitors: hypertension has been reported in a fairly considerable percentage of patients treated with sorafenib (5% of patients treated in the SHARP study and 12% in the TARGET study). It occurred early in the course of treatment, it was usually mild-to-moderate, and, in the majority of cases, it was controlled with standard anti-hypertensive therapies.30,35
Also cardiac toxicity seems peculiar of drugs targeting tyrosine-kinase patways. In the SHARP study, ischemia/infarction was observed in 3% of patients treated with sorafenib and in 1% in the placebo group: similarly, in the TARGET study, the incidence of treatment-emergent cardiac ischemia/infarction events was higher in the sorafenib group (2.9%) as compared to placebo group (0.4%). As regards other signs of cardiac toxicity, the incidence of decreases of LVEF values following treatment with sorafenib has been very little: only in a single patient a drop of 10% of LVEF was reported. In the sorafenib safety database, the incidence of congestive heart failures is <2%. 36
Quality of Life
No data on quality of life of HCC patients treated with sorafenib are presently available, mainly on account of the fact that a reliable evaluation of this parameter in patients bearing this tumor type is really extremely difficult to carry out. As previously mentioned, in both phase III pivotal studies in HCC5,10 the assessment of the TTSP using the FSHI-8-TSP scoring system failed to demonstrate any difference between the cohorts of patients treated with sorafenib and placebo. Therefore, at least for the time being, the only evidences it is possible to rely on are the level of tolerability of the treatment and its level of acceptance by patients. In this regard, data of the SHARP trial, which show that the rate of discontinuation of the study drug due to adverse events was similar in the two study groups (38%
Conclusions
To date, sorafenib represents the first and the only systemic therapy able to prolong survival in patients with advanced HCC: evidences coming from pivotal clinical trials led to the approval of this drug by the International Regulatory Authorities (FDA and EMEA) as the new reference standard treatment for patients with advanced HCC. 3 The clinical benefit obtained with sorafenib in HCC with a decrease of risk of death of 31% is similar in size to the ones obtained using other molecular targeted therapies in other tumor types such as trastuzumab in breast cancer, bevacizumab in colorectal cancer, erlotinib in non-small-cell lung cancer, which induced decreases in the hazard of death ranging from 25% to 35%. 8
Current knowledge leaves unsolved some important issues.
It is necessary to increase the Overall Survival benefit highlighted in the phase III trials, though an 0.69 HR it is comparable with the above mentioned therapies a 3 months increase in survival is not changing this disease natural history. Combination trials with sorafenib and other target agents have been planned in advanced HCC. 3 It is also important to plan sorafenib development in adjuvant therapy after potentially curative treatments, as resection and local ablation, due to the crucial need of an adjuvant therapy for high recurrence rate in this tumor. 3
Another important point, is the lack of prospective trials on biomarkers for sorafenib. Two retrospective analysis from HOPE 1 and SHARP 5 exclude VEGFR as possible biomarker; so it is difficult to understand if a positive correlation between sorafenib clinical effect and HCC vascularization exists. A biomarker should anticipate the real efficacy of a drug on a certain patient. This should optimize the public health expenditure, given the high cost of new biological therapies. Searching a good biomarker candidate it is difficult due to the lack of knowledge of sorafenib mechanism of action in human HCC.
No doubt however that the positive results of sorafenib represent an advancement in the care of patients for whom no effective therapy was previously available: nonetheless, this represents only the first step for a further development of this drug in advanced disease in combination with chemo-embolization or other molecularly targeted therapies, and, almost certainly, in the near future also in the adjuvant setting in earlier stages of disease after surgery. 8
Disclosure
The authors report no conflicts of interest.