
Abstract
Ulcerative colitis affects approximately 500,000 people within the U.S. For mild to moderate disease, 5-ASA is considered the first line medication to achieve both induction of remission and maintenance of remission. Since the use of sulfasalazine over 40 years ago, numerous new formulations have been created to minimize side effects and maximize drug delivery to the affected colon. Here, we have detailed the currently available 5-ASA formulations and explain why there is room for new and improved 5-ASA formulations. In addition, we will summarize the latest trials detailing the use of MMX mesalamine and where it may fit into the treatment algorithm for our patients with mild to moderate ulcerative colitis.
Epidemiology
Ulcerative colitis (UC) is a chronic inflammatory disease that involves the rectum and a variable portion of the colon. It is estimated that between 250,000-500,000 are affected with UC in the U.S. with an annual incidence of 7 per 100,000 per year. 1
The rectal mucosa is invariably affected. Confluent inflammation and shallow ulceration extend proximally from the anal margin. A patient may have proctitis, left sided colitis (the proximal limit being below the splenic flexure), extensive colitis (involving the transverse colon), or pan colitis. At any point in time, 50% of patients are asymptomatic, 30% have mild symptoms, and 20% have moderate to severe symptoms. 2 The symptoms include diarrhea containing blood and mucous, abdominal pain, fecal urgency, anemia, and weight loss. At a macro level, UC can have a significant impact on overall healthcare costs with an estimated $138 million in drug costs, and $192 million in hospital costs annually. 3 Current therapies focus on induction and maintenance of remission of symptoms. The standard for the induction and maintenance of mild to moderate disease is mesalamine (5-Aminosalicylic Acid derivative) therapy. Although it's exact mechanism of action remains unknown, studies suggest that it may work both as an anti-inflammatory and immunosuppressive agent. It prevents the formation of inflammatory agents by inhibiting both the cyclo-oxygenase and lipoxygenase pathways.4,5 Ahnfelt-Ronne et al demonstrated anti-oxidant properties that help mitigate tissue injury through it effects on free radical scavenging. 6 Several studies have also demonstrated that mesalamine may also act by inhibiting T-cell activation and proliferation, thus they may have some immunosuppressive qualities 7 . It is also thought to exert topical anti-inflammatory effects, therefore the goal is to deliver as much of the active drug to the affected portions of the colonic mucosa while minimizing systemic absorption in order to reduce adverse effects.
The molecular mechanisms responsible for the chemoprotective effects of mesalamine are not entirely understood. Recent studies suggest that 5-ASA may reduce the cancer risk by simply controlling inflammation through mechanisms that increase apoptosis, and decrease cellular proliferation by activating the peroxisome proliferator activated receptor γ (PPAR γ). 8
PPAR γ is highly expressed in colonic epithelium and can be activated by natural ligands (eicosanoids) and synthetic ligands (thiazolidinediones and NSAIDS). 9 PPAR γ is thought to play a regulatory role in carcinogenesis by regulating cellular proliferation and inducing apoptosis. Several studies have demonstrated inhibition of tumor by activators of PPAR γ, and terminal differentiation, inhibition of cell growth leading to G phase cell cycle arrest have also been displayed.10,11 They have demonstrated mesalamine caused a time and dose dependent decrease in both cell growth and proliferation through the PPAR γ dependent and independent pathways in colonocytes. 10
5-ASA Types
In mild to moderate colitis, mesalamine formulations have become first line therapy. Various formulations have been developed, each with a different delivery system. The goal of drug delivery is to avoid degradation and absorption in the upper gastrointestinal tract, so that the maximum concentration of drug can be delivered to the colon.
Sulfasalazine was originally used in rheumatoid arthritis patients. It was subsequently noted that patients with concomitant UC had an improvement in their colitis. 12
Sulfasalazine has been the main stay of UC treatment for the last 40 years. Sulfasalazine consists of sulfapyridine linked to 5-ASA by an azobond. When administered orally it is absorbed proximally in the stomach and small intestine. As a result, it requires higher dosing to achieve equivalent 5-ASA concentrations in the colon. A dose of 2-6 g/day can induce remission in about 50%-80% of patients. 13 A meta analysis also demonstrated that sulfasalazine was associated with a slightly higher and more significant rate of maintenance of UC remission compared with other formulations at six months, but similar at 12 months. 14 However due to the dose dependent adverse events related to the sulfa moiety, its use has become limited. Up to 30% of the Sulfasalazine users experience headache, nausea, dyspepsia and allergy. 15 Although there have been no reports to date regarding fetal injury, sulfasalazine impairs folate absorption and there is concern that it may cause an increase in birth defects. 16 Sulfasalazine can also cause impairment in sperm number and morphology, leading to reduced male fertility. This is reversible upon cessation of drug. 17
Because of its side effect profile, other 5-ASA drug delivery mechanisms have become popular. They include mesalamine with various pH-sensitive coatings (Asacol®, Proctor and Gamble pharmaceuticals, phoenix, AZ; Pentasa®, Shire Pharmaceuticals, Wayne, PA), azo-bond derivates which require colonic mucosa to release the active moieties (olsalazone, Dipentum®, UCB Inc., Symrna, GA), or attachments to inert carrier molecules (balsalazide, Colazal®, Salix Pharmaceuticals, Morrisville, NC).
Multiple meta-analyses have been done that have shown superiority of mesalamine to placebo.14,18 Sutherland et al. that 5-ASA at a dose of 2 gm/day was superior to placebo, and sulfasalazine in achieving remission. The outcome measures they used included endoscopic, global and clinical measures of improvement.
The most common side effects associated with pH-dependent release mesalamine in a six month study were headache, flu symptoms, diarrhea, rhinitis and abdominal pain (The Mesalamine Study Group 1996). Problems associated with rectal enemas include retention, burning sensation and bloating.19,20 Mesalamine can rarely cause hypersensitivity reactions. These range from generalized allergic reactions to fevers and rash. There are also rare reports of hepatitis, pancreatitis, pneumonitis and drug induced connective tissue disorder.21–23
Prior concerns with regards to nephrotoxicity by salicylates have been laid to rest, after recent studies demonstrated no reduction in glomerular filtration rate during maintenance therapy with mesalamine. 24 There have been case reports of allergic interstitial nephritis which has led to the common practice of periodic monitoring of renal function. 25
In rare instances, mesalamine can also cause worsening of colitis. 26 This is thought to be caused by enhanced bicarbonate secretion in the small intestine, which increases fluid volume received by the colon. This results in the colon being unable to resorb increased fluid volumes resulting in worsened diarrhea.
Compliance/Disease Activity/Medical Regimen Relationship
Most UC patients will relapse once after their initial diagnosis. 2 The efficacy of a maintenance regimen depends, in part, upon patient compliance.
To achieve therapeutic concentrations at the affected site, oral mesalamine formulations require multiple daily dosing with many tablets per dose in order to deliver a minimal aggregate dose of 2.4 g/day. Topical mesalamine enemas and suppositories are associated with leakage, retention and bloating making them uncomfortable for patients to use. 27
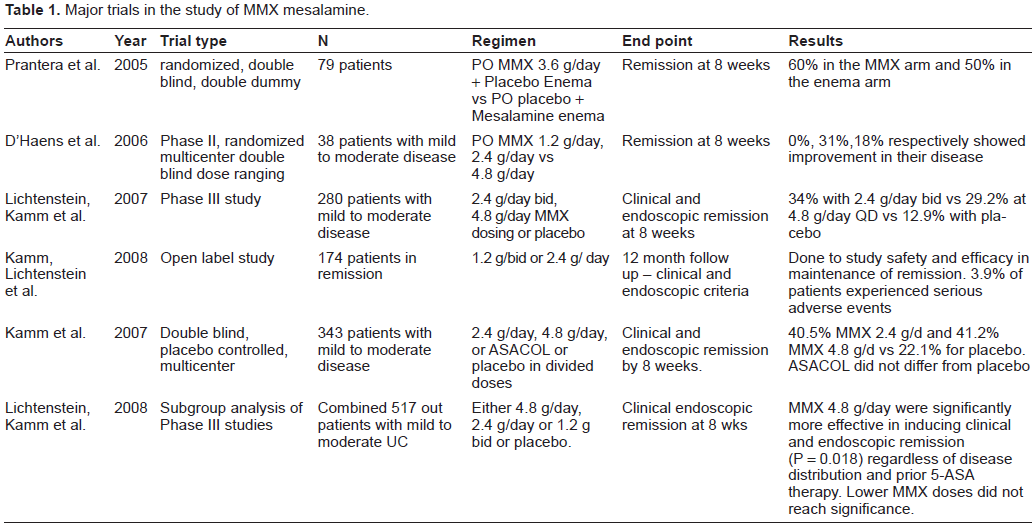
Major trials in the study of MMX mesalamine.
Patient non compliance to treatment regimens for chronic disease is widely recognized. Male gender, single status, full time employment, and taking more than four medications, complex dosing regimens were predictors for non adherence. 28 UC can be a waxing and waning disease. Patient adherence in periods of quiescence has been reported to be as low as 40%, and non adherence has been shown to be a predictor of relapse. 29 In a study assessing patients’ compliance via urine mesalamine levels and standardized questionnaires, 43% of patients took less than 80% of their prescribed medication. And 12% of patients had undetectable of levels of mesalamine in their urine.30,31 Reasons people sited for non compliance, included, forgetfulness, multiple pills, complicated scheduling regimens.
In an attempt to study compliance on a “once a day” pill regimen Kane et al. 29 compared 22 subjects on a once daily pH release therapy to the conventional 2 or 3 times daily in maintaining symptomatic UC remission. After three months 100% remained compliant in the experimental group compared to 70% of the conventional dosing regiment. However by six months the compliance rates between the groups were comparable as one patient from each arm relapsed. 29 Compliance rates reported in clinical trials of mesalamine are often high, however these rates my be reflective of the fact that that this is a supervised environment.32,34 There is room for improvement in creating a formulation to maximize drug delivery to the colon, to minimize the number of tablets to be ingested by patients, and for expected improvements in adherence rates to 5-ASA. 33
What is MMX
Multi-matrix (MMX) is a new formulation of mesalamine that is characterized by a polymeric matrix (MMX mesalamine, Lialda®, Shire, Wayne, PA). It has a lipophilic matrix that is dispersed within a hydrophilic matrix. It is coated with a film which undergoes pH dependent dissolution. The viscous mass hinders the diffusion and breakdown of the tablet, thus allowing dissemination of the mesalamine molecules in linear kinetics profile throughout the colon. The coating only begins to dissolve at a pH ≥ 7 usually at the ileum. At this point the hydrophilic part erodes and the active ingredient diffuses out of the lipophilic matrix. The release of 5-ASA is slow and gradual, and helps provide a consistent and homogeneous distribution along the different parts of the colon. 34
The hydrophilic matrix is also believed to adhere to the colonic mucosa, with 80% of absorption occurring in the colon. Moreover scintigraphic studies have shown active metabolite in the sigmoid colon 24 hrs after ingestion.
The challenge lies in delivering mesalamine orally to the left side of the colon. In a study by De Vos et al. 35 multiple biopsies taken at the same location throughout patients lower gastrointestinal tracts following cessation of one week therapy with different oral 5-ASA formulation, there was 1000 fold variation in mucosal concentrations. This was confirmed in a study by a'Albasio 36 which showed that the combination of oral and topical therapy is superior to oral therapy alone in maintenance regimens for treatment of left sided colitis.
Data of MMX in UC
A phase II, randomized, multicenter double blind dose ranging study by D'Haens et al. used three different dosages for the MMX given once daily for the induction of remission in 38 patients with mild to moderate disease. Remission at the end of week 8 was defined as UC-DAI score of 1 or less, at a score of 0 for rectal bleeding and stool frequency at least a one point reduction in sigmoidoscopy scores from baseline. 37 The greatest improvement was seen in the 4.8 g/d, although this was not significantly different from the 2.4 g/d group. All dosages were well tolerated and demonstrated an improvement in the symptoms score. Because the population size was limited the data did not reveal a true dose response curve, however MMX given at 2.4 g/day or 4.8 g/day was effective once daily treatment for mild to moderate UC in up to 31% of the study population. Additionally, in this phase II study, there was no placebo or comparator arm. Hence, no conclusions could be drawn regarding incremental benefit or superiority of one delivery system over another.
In a large randomized, double-blind, placebo-controlled, multicenter phase III study in patients with mild to moderately active ulcerative colitis compared bid dosing to MMX with the primary end point being the percentage of patients in clinical and endoscopic remission. 38 280 patients were studied and were either randomized to receive either MMX 4.8 g/day (either as once a day dosing or divided dosing on BID schedule) or placebo for 8 weeks. The primary end point of the study was clinical and endoscopic remission at week 8, defined as UC-DAI score of <1 and a score of 0 for no rectal bleeding and stool frequency, at least a one point reduction in sigmoidoscopy score from baseline At the end of week 8 both MMX mesalamine groups achieved statistically significant clinical and endoscopic remission compared with placebo (34% vs 12.9% with 2.4 g/day (P < 0.001), and 29.2% vs 12.9% with 4.8 g/day (P = 0.009). The percentage of patients achieving sigmoidoscopic improvement (defined as a change in mucosal appearance from baseline to week 8) were 61.4% and 69.7% vs 35.5% for placebo (P = 0.002). Interestingly, there does not seem to be a disadvantage to once daily dosing with this medication, which may be useful in improving adherence rates. This was confirmed in a second study showing no difference in maintenance of remission using either 1.2 g/bid or 2.4 g/day. 39
Kamm et al conducted a double blind, placebo controlled, multicenter clinical trial to evaluate MMX mesalamine vs Asacol with a placebo control. The trial consisted of 343 patients with active mild to moderate UC who received either 2.4 g/day or 4.8 g/day of MMX or ASACOL 2.4 g/day in divided doses or placebo for 8 weeks. The end point was clinical and endoscopic remission (UC-DAI < 1). At both doses of MMX mesalamine, 40.5% and 41.2% (P = 0.01, 0.007 respectively) achieved clinical and endoscopic remission at week 8 compared to the placebo group. Results of the ASACOL arm did not differ significantly from the placebo group 32.6% vs 22.1%. Endoscopic remission rates were higher in the MMX arms compared to placebo (2.4 g/day MMX 69%, 4.8 g/day MMX 77.6% Asacol 61.6% vs placebo at 46.5%.) P values = 0.003, <0.01), and = 0.047 respectively. 40 All forms of treatment were well tolerated. It is not clear why the 2.4 g/d dosing was chosen for the study, except for the statement that this complied with the approved dosing indication. It should be noted, that the ASCEND trials demonstrated the superiority of the 4.8 g/d over 2.4 g/d of ASACOL in the treatment of moderate ulcerative colitis.41,42 In addition, there is a large body of literature supporting the superiority of ASACOL over placebo, so the disparate results in this study needs to be seen as an outlier. 43
Data from two double blind, placebo controlled trials38,40 were analyzed to evaluate the efficacy and tolerability of MMX. 44 Patients were given either 4.8 g/day, 2.4 g/day (either daily or 1.2 g twice daily) or placebo. The percentage of patients in remission was similar, and significantly greater than placebo, stratified by disease extent, disease severity, gender and 5-ASA naive patients. Moreover patients transferring from low dose to MMX 4.8 g/day were significantly more effective in inducing clinical and endoscopic remission (P = 0.018). 44 This was one of the first studies to demonstrate efficacy regardless of the patient subpopulation.
Patients with active, mild to moderate UC who did not achieve clinical and endoscopic remission after 8 weeks of treatment with MMX Mesalamine (2.4 g/day or 4.8 g/day) in the phase III studies received MMX Mesalamine 4.8 g/day for 8 weeks. 304 patients were evaluated and 59.5% achieved remission at week 8. This trial suggests that a prolonged period of MMX mesalamine may be useful in some patients who want to avoid step up therapy. However, the trial did not use any control arms and there is no way to know how many of these patients improved as a result of the natural history of their disease as opposed to the beneficial effects of the MMX mesalamine. Currently, providers will still need to use their judgment about how long to continue MMX mesalamine therapy before considering an alternative or step up approach. 45
Conclusions
According to ACG guidelines, mesalamine is a first line treatment for the induction and maintenance of remission in patients with mild to moderate UC.
Numerous mesalamine formulations have been developed with the aim of decreasing proximal absorption and achieving high concentration at the affected colonic mucosa. Topical formulations have been limited because of poor patient acceptability and undesirable routes of administration. Other oral 5-ASA agents have limited compliance due to multiple dosing and often complex regimens. 3
The development of MMX was intended to increase colonic mesalamine concentrations, and to improve adherence, reduce relapse and improve quality of life. Current data supports the use of MMX mesalamine for treatment of mild to moderate UC by demonstrating at 2.4-4.8 g/day can induce remission and improve quality of life. The advantage of the one day dosing improves adherence and compliance, 30 thus decreasing the rate of exacerbation, health costs and improving quality of life, thought this has not been specifically demonstrated with MMX mesalamine.
Previous studies have suggested that the azo bond release mechanism may be more effective than the pH dependent release in some UC patients, based on the presumed failure of the initial pH dependent coating to dissolve in individuals who don't attain such a high pH in their colon, a possibility in patients with active colitis. 46 Theoretically MMX mesalamine may be subjected to the same failure as it employs a similar pH sensitive coating for its initial release.
Limitations in the current data exist. The available studies differ in the defining endpoints of remissions, techniques used to measure the endpoint of evaluation, use of comparator groups, and the relatively short follow up durations (8 weeks or less).
MMX may improve patient adherence given the once daily formulation, and achieve better patient outcomes in the long term. Large adequately powered trials comparing MMX with other 5-ASA formulations given once daily are required in order to draw appropriate conclusions. Further studies are needed to elucidate cost effectiveness, compliance, and long term outcomes of MMX mesalamine.
Disclosure
The authors report no conflicts of interest.