
Abstract
Fibromyalgia is a central sensitization disorder characterized by chronic widespread pain, nonrestorative sleep, fatigue, cognitive dysfunction as well as a number of somatic symptoms; that reduces physical/emotional function/quality of life. Treatment options include: Patients education, behavioral medicine strategies, (eg, cognitive behavioral therapy), physical medicine strategies (eg, exercise/aerobic and strength training), and pharmacologic agents.
Currently there are three agents approved by the US Federal Drug Administration for the treatment of Fibromyalgia: pregabalin, duloxetine, and milnacipran. Milnacipran is a norepinephrine-serotonin reuptake inhibitor that is only approved in the US for fibromyalgia. It has 3-fold increased selectivity for norepinephrine compared to serotonin. Milnacipran is well absorbed (85% bioavailability), has a half-life of 6-8 hours, and does not undergo cytochrome P450 metabolism. Milnacipran in doses of 50 mg PO BID to 100 mg PO BID has been shown to have efficacy for fibromyalgia. The most common adverse effect is nausea.
Introduction
Fibromyalgia (FM) is a central pain disorder that is somewhat controversial and appears to involve altered afferent processing, with subsequent enhancement of afferent input, especially the nociceptive types. 1 The “core” symptoms seen in FM and many other central sensitization disorders include widespread pain, fatigue, insomnia, cognitive/memory problems, and psychological distress. 2 Other symptoms include: stiffness, impaired physical function, headaches, and sexual dysfunction. (See Fig. 1). 3
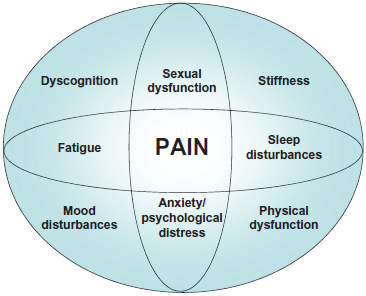
Fibromyalgia domains.
Currently there are three agents approved by the US Federal Drug Administration (FDA) for the treatment of FM: pregabalin, milnacipran, and duloxetine. Duloxetine is among the class of drugs known as serotonin-norepinephrine reuptake inhibitors (SNRIs), and represents an important pharmacologic therapeutic option for FM.
Fibromyalgia Syndrome
It appears that 2%-4% of the population suffers from FM, with the disorder being 2 times more prevalent among women than men.4,5 The disorder is predominantly diagnosed in patients aged 20-60 years (mean age, 49 years).4,5 FM negatively impacts the physical functioning of its patients, as evidenced by difficulties with multiple daily activities. 6 Panton and colleagues used the Continuous Scale-Physical Functional Performance Test (a validated test of 16 tasks in 5 domains that assesses functional performance of routine activities of daily living) to study three groups of women,–-one group in their mid-forties with FM, one healthy group in their mid-forties without FM, and one healthy group without FM with an average age of 71. 6 The young healthy women without FM had significantly higher functionality scores compared with young women with FM and older women. 6 There were no differences in functionality between young women with FM and older women. The pain disorder, however, seems to have the most significant impact on emotional health and social functioning. 7 The EPISER study demonstrated that patients with FM had similar physical impairment but worse psychological impairment than patients with rheumatoid arthritis. 7 Women with FM have lower quality of life (QOL) measures than women with other chronic disorders, including rheumatoid arthritis, chronic obstructive pulmonary disease, and diabetes mellitus. 5 Finally, FM appears to negatively affect personal relationships, career, and mental health. 8
Assessment of fibromyalgia
In 1990, the American College of Rheumatology (ACR) developed research criteria 9 requiring that an individual possess both a history of chronic widespread pain and ≥ 11 of 18 possible tender points on physical examination. The Manchester criteria 10 utilize a whole body diagram to indicate areas of pain, thereby obviating the necessity of tender points. However, both of these criteria are used predominantly for research/epidemiologic purposes. The use of tender points as diagnostic criteria began to fade as it fails to recognize the presence of other symptoms that need to be addressed to optimally manage FM patients. 11
In 2003 Wolfe et al conducted a study in which they mailed surveys to 12,799 patients with either rheumatoid arthritis, osteoarthritis, or FM. 12 They found that pain present in 19 primarily non-articular sites differentiated FM from the other two disorders.12,13 This study led to the proposal of diagnostic criteria that assessed chronic widespread pain without the use of trigger points. It expanded the definition of FM to include symptoms other than pain, such as fatigue, sleep disturbance, and cognitive dysfunction. 14 The criteria also include a separate measure of symptom-related severity, which is an important component in the adequate evaluation and management of FM patients. 15
The Fibromyalgia Impact Questionnaire (FIQ) is a validated, FM-specific instrument developed to assess the range of symptoms experienced by FM patients. 16 It was updated in 1997 and 2002 in part to improve the clarity of the scoring system. 17 It includes 20 questions that assess functionality with ADLs, work difficulty, general feelings of well-being, sleep quality and the degree of intensity of symptom complaints including pain, fatigue, depression, anxiety, and stiffness. 18 Bennett et al performed an analysis which demonstrated that a 14% change in the FIQ total score represented a statistically and clinically meaningful difference for the FM patient. 19
The Revised Fibromyalgia Impact Questionnaire (FIQR) is an updated version of the FIQ that has good psychometric properties, is easy to score, and can be completed in less than 2 minutes. 17 It has the same 3 domains as the FIQ: function, overall impact, and symptoms. It differs from the FIQ in that it has modified function questions and includes questions pertaining to memory, tenderness, balance, and environmental sensitivity. All questions are graded on a 0-10 numerical scale. 17 Each of the three domains of the FIQR correlated well with the related domains of the FIQ (r = 0.69 to 0.88, P < 0.01). The total scores of the FIQR and the FIQ were also closely correlated (r = 0.88, P < 0.001).
A new paradigm for diagnosing fibromyalgia
Before the 2010 American College of Rheumatology preliminary fibromyalgia diagnostic criteria, 20 the diagnosis of FM was straightforward for clinicians experienced in performing the tender point examination. After determining that the patient had widespread pain, the clinician would then perform an examination of 18 specific anatomic points as described by the 1990 ACR Classification Criteria. 9
The 2010 proposed ACR Diagnostic Criteria made diagnosis easier by eliminating the tender point examination, but included the evaluation of symptoms. The 2010 criteria altered the diagnosis of fibromyalgia by including symptoms as a central part of the syndrome. Thus, with these new 2010 criteria the patient's history became a predominant feature to FM diagnosis and the physical exam became relatively less important than with the 1990 criteria.20,21
Pain extent
The count of painful regions can be determined in a number of ways. The physician can simply interview the patient and record the locations of pain. Another way to get painful region data is to ask the patient to complete a checklist of painful regions or to use a manikin checklist.20,21
Non-pain symptoms
By contrast, the severity of four criteria symptoms (fatigue, unrefreshed sleep, cognitive problems, and somatic symptoms) must represent the physician's rating [from 0 to 3] after a clinical evaluation (See Table 1).20,21 The regular “review of systems” will often be sufficient to determine somatic symptom extent. Clinicians cannot simply count up symptoms.20,21
2010 CR preliminary diagnostic fibromyalgia criteria.
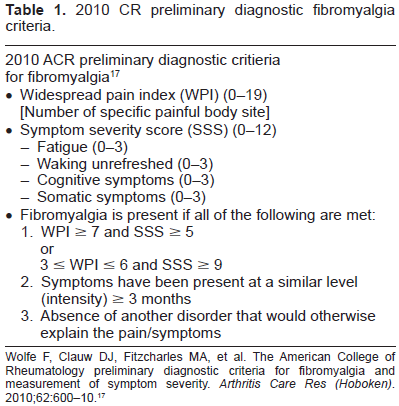
Wolfe F, Clauw DJ, Fitzcharles MA, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res (Hoboken). 2010;62:600-10. 17
Identification of disorders that can mimic FM (eg, hypothyroidism and inflammatory rheumatic diseases) or that are frequent comorbid conditions in patients with FM (eg, RA, osteoarthritis, systemic lupus erythematosus, myofacial pain syndrome, polymyalgia rheumatica, polymyositis, spinal stenosis, neuropathies, sleep disorders such as sleep apnea, and mood and anxiety disorders) is essential so that appropriate treatments can be initiated. 22
Pathophysiology of fibromyalgia
The precise mechanisms responsible for FM remain uncertain, but probably involve alterations in noceiceptive processing systems. It is likely that patients with FM have impaired descending inhibitory pathways, which normally function as endogenous analgesic systems to ameliorate pain in healthy subjects. These descending inhibitory pathways are mediated in part by the neurotransmitters serotonin and norepinephrine (See Fig. 2). 23
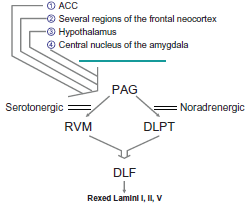
Descending inhibiting pain modulating circuits.
Russell and colleagues demonstrated that patients with FM have lower cerebrospinal fluid (CSF) levels of metabolites of biogenic amines (eg, serotonin and norepinephrine). 24 Further support comes from treatment studies which reveal that any agent that simultaneously raises both serotonin and norepinephrine (eg, tricyclic antidepressants, duloxetine, milnacipran, tramadol) has been shown to be efficacious in treating FM.25–29
Other mechanisms that may play a role in the pathophysiology of FM are the presence of augmented pronociceptive pathways in these patients. These pathways are mediated in part by substance P and the excitatory amino acid glutamate. 30 Studies demonstrate that patients with FM have significantly higher concentrations of substance P in CSF compared with healthy subjects.31–35 CSF levels of glutamate are also twice as high in patients with FM compared with healthy controls. 36 Furthermore, levels of the neurotrophic factors brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF) were increased in CSF of FM patients, however, this finding is not specific to FM (also found in patients with chronic migraine). 37
Although there is no direct evidence, it is hypothetically conceivable that microglial activation may contribute to FM pathophysiology.38,39 Microglial activation could lead to thalamic changes40,41 with resultant abnormal processing of ascending input in FM. 38 Thalamic changes in FM appear to be supported by neuroimaging studies42,43 and altered thalamic blood flow present in chronic pain states may normalize upon pain relief.44,45 Microglial activation coupled with thalamic changes may trigger neuronal hyperexcitability which in conjunction with diminished or inefficient descending inhibitory pathways in FM [(as evidenced by reduced diffuse noxious inhibitory controls [DNIC] in FM patients46–48 (or the now “preferred” term in place of DNIC, conditioned pain modulation [CPM]),49,50 may lead to central sensitization with the subsequent development of chronic pain. 38
Non-pharmacologic treatment of fibromyalgia
Non-pharmacologic approaches such as exercise, education, and cognitive-behavioral therapy have a positive impact in FM, but it is felt that these treatments appear to be underutilized in usual clinical practice.51,52
A review by Jones et al suggests that exercise appears to be beneficial in FM patients, especially with respect to reducing physical symptoms and improving functional capacity. 53 Exercise modalities studied included land and water aerobics, strength training, flexibility training, and various combinations of these. 53 The strongest evidence demonstrating benefit in FM is for aerobic and mixed-type exercises, with growing evidence for positive effects from strength training.54–57 Busch et al systematically reviewed 34 studies assessing the efficacy of exercise in FM. Meta-analysis of six of those studies provided moderate-quality evidence that aerobic-only exercise at intensity levels recommended by the American College of Sports Medicine has positive effects on global-well being, physical functioning, and potentially on pain. 58
Patient education has also been analyzed as a therapeutic option for FM patients. Rooks et al 59 completed a RCT with 207 participants with FM who were randomized to four groups: (1) aerobic and flexibility training group; (2) strength, aerobic, and flexibility training group; (3) the Fibromyalgia Self-Help Course; or (4) a combination of the previous three. The combination group was found to provide the most benefit. 59 Thus, education may be useful for FM patients when utilized with other multi-modal interventions.
Cognitive-behavioral therapy (CBT) combines aspects of both cognitive and behavioral interventions. Catastrophic thoughts, which are beliefs that the worst possible outcome is going to occur, may be associated with increased pain severity, reduced functional capacity, and affective distress in FM patients. 60 Cognitive therapy may focus on taking catastrophic thoughts and reframing them into more positive beliefs. 61 Behavioral therapy, in contrast, usually stresses the importance of operant behavioral change over inner thoughts and feelings. 61 Its goals are to increase adaptive behavior through positive and negative reinforcement, and to extinguish maladaptive behavior through punishment. 61 Affective CBT may include relaxation training, activity regulation, facilitation of emotional awareness, cognitive restructuring, and interpersonal communication training. Studies have demonstrated that both operant behavioral treatment (OBT) and CBT are effective modalities in treating FM.62,63
Bernardy et al 64 recently performed the first metaanalysis of the efficacy of CBT in FM. The systematic review included 14 out of 27 studies with 910 subjects and a median treatment time of 27 hours over a median time range of 9 weeks. The primary endpoints were pain, sleep, fatigue, and health-related quality of life (HRQOL). Secondary endpoints included depressed mood, self-efficacy pain, and healthcare-seeking behavior. 64 They demonstrated that CBT reduced depressed mood and self-efficacy pain post-treatment, but had no significant effects on pain, fatigue, sleep, or HRQOL after treatment or at follow-up. Furthermore, OBT was shown to significantly reduce the number of physician visits at follow-up. Thus CBT may be most beneficial in helping FM patients cope with pain and depression on their own and somewhat reduce dependence on health care providers. 64
Pharmacologic treatment of fibromyalgia
The majority of clinical trials evaluating FM therapy have included antidepressants of one class or another, especially the older, tricyclic antidepressants (TCAs). Uceyler et al performed a meta-analysis on the efficacy of antidepressants for treating FM. The authors found amitriptyline, studied in 13 randomized controlled trials (RCTs), to provide a moderate magnitude of relief to FM patients (pain reduction by mean of 26%, improvement in QOL by 30%). 25 Other RCTs demonstrate the effectiveness of amitriptyline (a TCA) and cyclobenzaprine (structurally similar to amitriptyline) in reducing the symptoms of pain, poor sleep, and fatigue. 18 Cyclobenzaprine, a centrally acting muscle relaxant, has been used to treat the musculoskeletal component and improve sleep in FM patients. 19
Most of the SNRIs clinically available for the treatment of FM have more of a significant impact on serotonin compared with norepinephrine activity (See Fig. 3).
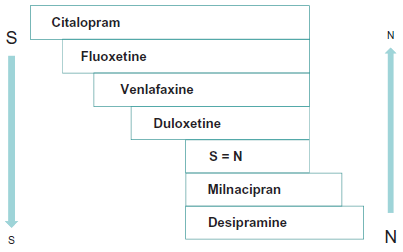
Relative activity on serotonin and norepinephrine reuptake among antidepressants.
SNRIs tend to be better tolerated than older TCAs. Venlafaxine, the first SNRI available in the US, tends to have clinically significant effects on norepinephrine reuptake only when used at higher doses. 65 Thus, venlafaxine could potentially be beneficial in FM patients when used at these doses. 65 Duloxetine and milnacipran are two SNRIs that are approved for the treatment of FM in the US (in 2008 and 2009, respectively) and have been shown to be efficacious in this disorder.66,67 The efficacy and tolerability of duloxetine will be discussed later in this paper. Milnacipran is one of the few SNRIs that inhibits norepinephrine reuptake more than serotonin reuptake. The standard dosing is 100 mg/day, which in selected patients can be increased to 200 mg/day based on responsiveness and tolerability. The usual half-life of milnacipran is 6-8 hours for the parent compound and 8-10 hours for d-milnacipran, the active isomer; thus twice-daily dosing is recommended. 68 Milnacipran has shown benefit in the treatment of FM, improving the symptoms of fatigue, reduced physical functioning, and discomfort.69–71
Pregabalin, approved for the treatment of FM in the US in 2007, is a gamma-aminobutyric acid (GABA) analog which binds to the alpha-2-delta subunit of calcium ion channels. The half-life of pregabalin is 5.5-6.7 hours in the presence of a normal creatinine clearance (CrCl). 68 The dosing for this agent, however, is dependent upon the patient's CrCl because elimination is a function of renal clearance. Decremental dosing changes are recommended in patients with impaired renal function. Dosing secondary to side effects is based on 1-week intervals focusing on patient responsiveness and tolerability. 68 Hauser et al conducted a systematic review evaluating pregabalin that included 5 studies. 72 There was strong evidence demonstrating reduction of pain, improvement in sleep, and improved HRQOL, but not depressed mood. 72 These studies potentially lack external validity in that patients with severe co-morbid depression and disability were excluded from participation. 73 The FREEDOM (Fibromyalgia Relapse Evaluation and Efficacy for Durability of Meaningful Relief) double-blinded trial 74 evaluated the durability of pregabalin in 1,051 FM patients in whom the drug initially worked. By the end of the double-blinded phase, 61% of patients in the placebo group had stopped responding compared with 32% in the pregabalin treatment group. 74
Gabapentin is another alpha-2-delta ligand and antiepileptic drug structurally similar to pregabalin, but not approved for the treatment of FM. However, the agent has shown potential benefit in clinical trials. Arnold et al found gabapentin (1,200-2,400 mg/day) to be effective and safe in FM. 75
Other centrally acting agents may show benefit in FM patients with a predominant symptom-type. For example, gamma-hydroxybutyrate, with its strong sedative qualities, may be clinically useful for FM patients with insomnia/sleep disturbance. 76 Pramipexole, a dopamine agonist used for Parkinson's disease, could be potentially useful for FM patients with concomitant restless leg syndrome. 77 Tramadol, which possesses some analgesic activity, may be utilized for FM patients with a significant pain component to their disease.29,78 Finally, tizanidine, an alpha-2-adrenergic agonist muscle relaxant, could be potentially used for FM patients with spasticity. 79
Pharmacologic overview of milnacipran
Milnacipran hydrochloride (C
The d-enantiomer has a half-life (t 1/2) of 8-10 hours and the l-enantiomer has at 1/2 of 4-6 hours. 85 There is no interconversion between d- and l-milnacipran. 80 Milnacipran seems to act exclusively presynaptically, inhibiting the uptake of 5-HT and NE. 85 In preclinical studies 86 and clinical trials,87,88 milnacipran at dosages of 50 to 400 mg/d was associated with minimal orthostatic hypotension, anticholinergic adverse effects, and sedation as predicted by its lack of appreciable affinity for α-1 adrenergic, muscarinic, or histamine receptors. 89
The recommended starting dose of milnacipran for the treatment of FM in adults in the US is a single 12.5 mg dose on day 1. 80 The drug is then titrated to the recommended maintenance dose of 100 mg/day (in two divided doses) over a 1-week period. The milnacipran maintenance dosage may be increased to 200 mg/day (in two divided doses) based on patient response. 80
The maintenance dose of milnacipran should be reduced by half (to 50 mg/day in two divided doses) in patients with severe renal impairment (CrCL between 5 and 29 mL/min [0.3-1.7 L/h]), and caution should be exercised in patients with moderate renal impairment. 80 In studies evaluating the effects of hepatic impairment on the single-dose pharmacokinetics of milnacipran, area under the curve (AUC) and t1/2 were similar in healthy volunteers and patients with mild to moderate impairment (Child-Pugh class A or B), 80 thus no dosage adjustments for milnacipran are recommended. 80
Patients discontinuing milnacipran treatment should have their dosage tapered and be monitored for withdrawal symptoms. 80 A period of at least 2 weeks should elapse between discontinuation of a monoamine oxidase inhibitor (MAOI) and the start of milnacipran treatment. Concomitant use of mil-nacipran and MAOIs is contraindicated due to the possibility of the rare, but serious, adverse event of serotonin syndrome. 80 The use of milnacipran in patients with uncontrolled narrow-angle glaucoma is also contraindicated. 80
All patients treated with milnacipran should be monitored for worsening of depressive symptoms and suicide risk. 80 Patients should also be monitored for elevations in heart rate and blood pressure prior to and during milnacipran treatment. 80
Preclinical support for analgesic properties of milnacipran
Milnacipran has displayed analgesic activity in several rodent models of pain. Milnacipran reversed hyperalgesia and allodynia following oral, intracerebral and intrathecal administration in rats, suggesting CNS-mediated, rather than locally-medicated, anti-nociceptive activity. 90
Berrocoso and colleagues evaluated milnacipran, in comparison with amitriptyline, on cold and mechanical allodynia in a rat model of neuropathic pain. 91 Acute amitriptyline (10 mg/kgi · p ·) was efficacious against mechanical, but less so against cold allodynia; under sub-chronic conditions, it was only active against mechanical allodynia. Milnacipran was found to be as efficacious as amitriptyline in a pre-clinical model of injury-induced neuropathy, and for the first time Berrocoso et al revealed that milnacipran is active acutely and sub-chronically against cold allodynia. 91
Efficacy of milnacipran
Milnacipran is only FDA approved for FM. The efficacy of milnacipran in the management of FM has been evaluated in four large, randomized, double-blind, placebo controlled multicenter, phase III trials of 370,92,93 or 6 71 months’ duration, three of which were conducted in the US70,71,92 and one in Europe. 93
Two early smaller preliminary trials demonstrated the benefits of milnacipran in improving pain and other FM symptoms,67,94 of which supported the use of twice-daily over once-daily milnacipran dosing.67,94
Mease and colleagues performed a 27-week, randomized, double-blind, multicenter study that compared milnacipran 100 and 200 mg/day with placebo in the treatment of 888 patients with FM. 71 “FM responders” met all three response criteria for improvements in pain, patient global impression of change (PGIC), and physical functioning; while “FM pain responders” met two of the response criteria for improvements in pain and PGIC. 71 After 3-months of a stable dose treatment with 100 mg/day or 200 mg/day(d), a significantly higher percentage of milnacipran-treated patients achieved the primary endpoint by meeting criteria as FM responders versus placebo (milnacipran 200 mg/day, P = 0.017; milnacipran 100 mg/day, P = 0.028). A significantly higher percentage of patients treated with milnacipran 200 mg/day also met criteria as FM pain responders versus placebo. 71 At 15 weeks, milnacipran 200 mg/day led to significant improvements over placebo in pain, PGIC, fatigue, and cognition. 71 At 27 weeks, a greater percentage of milnaciprain treated patients met criteria as FM and FM pain composite responders as compared to patients on placebo. 71
Clauw and colleagues performed a 15-week multi-center, randomized, double-blind, placebo-controlled trial that compared milnacipran 100 mg/d and mil-nacipran 200 mg/d with placebo in the treatment of 1196 patients with FM. 70 FM composite responders were defined as patients who had improvements in the following 3 domain criteria: pain; patients’ global impression of change; and physical function. Compared with placebo, significantly greater proportions of milnacipran-treated patients were FM composite responders and FM pain composite responders. 70
Arnold and colleagues performed a randomized double-blind, placebo-controlled trial to assess 1,025 patients with FM who were randomized to receive milnacipran 100 mg/day (n = 516) or placebo (n = 509). 92 Patients underwent 4-6 weeks of flexible dose escalation followed by 12 weeks of stable-dose treatment. The 2-measure composite response required achievement of ≥30% improvement from baseline in the pain score and a rating of “very much improved” or “much improved” on the PGIC scale. The 3-measure composite response required satisfaction of these same 2 improvement criteria for pain and global status as well as improvement in physical function on the SF-36) PCS score. 92 A significantly greater proportion of milnacipran-treated patients compared with placebo-treated patients showed clinically meaningful improvements, with respect to the 2-measure composite responder criteria and 3 -measure composite responder criteria after 12 weeks of stable-dose treatment. Milnacipran-treated patients also demonstrated significantly greater improvements from baseline on multiple secondary outcomes, including pain scores, PGIC scores, SF-36 PCS and mental component summary scores, FIQ total score, and Multidimensional Fatigue Inventory total score. 92
Branco and colleagues performed a 17-week treatment, randomized, double-blind, placebo-controlled, multicenter study that compared milnacipran 200 mg/day with placebo in the treatment of 884 European patients with FM. 93 Milnacipran 200 mg/day showed significant improvements from baseline relative to placebo in the 2-measure composite responder criteria and FIQ total score after the end of the stable dose period [ie, week 16]. Significant improvements were also observed in multiple secondary efficacy endpoints, including Short-Form 36 Health Survey (SF-36) PCS, SF-36 Mental Component Summary, Multidimensional Fatigue Inventory (P = 0.006), and Multiple Ability Self-Report Questionnaire (Table 2). 93
Descriptive characteristics of studies of milnacipan for fibromyalgia (FM).

Goldenberg and colleagues studied 449 patients who completed a 6-month lead-in study 95 enrolled in this 6-month extension study (87.7% of eligible subjects). 95 Patients initially assigned to placebo or milnacipran 100 mg/day were re-randomized (1:4) to either 100 mg/day (n = 48) or 200 mg/day (n = 192) of milnacipran for an additional 6 months of treatment. Patients initially receiving milnacipran 200 mg/day during the lead-in study were maintained at 200 mg/ day (n = 209). Goldenberg et al found that milnacipran safely and effectively improves pain and the multiple symptoms of FM (with improved FIQ total scores [eg, less stiffness or interference with activities of daily living/work, sleep, fatigue, and/or mood]), suggesting that milnacipran provides 1-year durable efficacy in this patient population. 95
Branco continued his 3 month study with the completers into a double-blind, 1-year extension study investigating the longterm efficacy and safety of milnacipran 100, 150, and 200 mg/day in the treatment of FM. 28 Over 1 year, milnacipran 100, 150, and 200 mg/day exhibited sustained improvement and safe therapeutic effects on pain, fatigue, sleep, and cognitive complaints. 28
Additionally, it appears that patients diagnosed with FM who remain on milnacipran therapy can achieve long-term pain relief; to at least three years. 96 After obtaining about a 25% decrease in pain scores within three months of therapy with milnacipran, the 217 patients who stayed on open-label treatment maintained that relief level to at least 38 months. 96 Of the patients who remained on the study, 70% demonstrated clinically significant improvements in global status after three years of treatment. 96 The trial originally included 1,268 patients with 1,220 in an intention-to-treat status. The four-phase study included a two-week washout period, a two-week dose-scalation period, then eight weeks on a stable dose. That was followed by flexible dosing of 50 mg to 200 mg of milnacipran a day through the three-year run of the study. The relief achieved by the 820 patients treated for one year of the trial was similar to the pain relief achieved by the 462 patients treated for two years of therapy and by the 217 patients who were treated for three years. 96 1,212 patients evaluated from the original cohort achieved a mean decrease of 17.6 points in their Visual Analogue Scale (VAS) pain score and at the three-year visit, the VAS pain score among the 217 patients still on medication showed a 23.9-point decrease. Thus, throughout the three years of study in general, patients who initially benefited from Milnacipran in terms of pain relief, maintained consistent clinically meaningful analgesia. The responder rate to milnacipran remained about 70% of the population across all three years of the study. 96
Safety and tolerability of milnacipran
Tolerability data are available from a pooled analysis (n = 2209) of three double-blind, placebo controlled trials of ≤29 weeks’ duration in the manufacturer's prescribing information 80 as well as data in various studies.70,71,92,93 Milnacipran was generally well tolerated during 6 months of treatment in adults with FM, with most treatment-emergent adverse events being mild to moderate in severity.70,71,92,93
Nausea was the most common adverse event in milnacipran recipients in the pooled 80 and in the individual trials discussed in section 3.70,71,92,93 In one trial, nausea (reported in 36.6% of milnacipran 100 mg/day recipients and 20.8% of placebo recipients) resolved within 3 weeks of trial completion in approximately 70% (69.5% and 72.1%) of patients. 92
According to the pooled analysis, 23% of milnacipran 100 mg/day recipients, 26% of milnacipran 200 mg/day recipients and 12% of placebo recipients discontinued treatment prematurely because of adverse events. 80 Adverse events that occurred with an incidence of ≥4% in milnacipran 100 or 200 mg/day recipients and at least twice as frequently than with placebo were constipation, hot flushes, hyperhidrosis, palpitations, hypertension, vomiting, increased heart rate and dry mouth.
Milnacipran did not disrupt cognitive function or psychomotor performance when administered as single daily doses of up to 100 mg in young healthy volunteers, or as repeated daily 75 mg doses for 3 days in healthy elderly subjects (aged >65 years). 97 A placebo-controlled study also demonstrated the lack of effect of milnacipran (100 mg/day, in two divided doses, for 1 week) on cognitive functions of healthy volunteers. 98
Rates of serious adverse events were generally similar in the milnacipran 100 mg/day, milnacipran 200 mg/day and placebo groups across the US trials (1.3%-1.6%, 1.0%-2.5% and 1.2%-2.7%, respectively).70,71,92 Corresponding rates of discontinuation because of adverse events were 17.8%-19.6%, 23.7%-27.0% and 9.5%-13.9%, respectively.70,71,92
Milnacipran was generally well tolerated in the longer-term (12-month) study. 71 Nausea was the most commonly reported newly-emergent adverse event (occurring in 18.8% and 17.5% of milnacipran 100 and 200 mg/day recipients). 71 Branco and colleagues conducted a double-blind, 1-year extension study investigated the long-term efficacy and safety of milnacipran 100, 150, and 200 mg/day in the treatment of FM in completers of a 3-month European double-blind lead-in study of milnacipran 200 mg/day versus placebo. 28
The proportion of composite responders at the 1-year endpoint, ranged from 27.5% to 35.9%, and had increased from the extension study baseline by 15.2% to 20.7%. 28 At endpoint, an improvement from both baselines was shown in all groups with respect to pain, fatigue, sleep, and quality of life measures. Up to 1 year, all doses of milnacipran were safe and well tolerated. The most common drug-related adverse events were hyperhidrosis and nausea. Over a 1 year period Branco et al concluded that milnacipran 100, 150, and 200 mg/day exhibited sustained and safe therapeutic effects on predominant symptoms of FM. 28
Mease and colleagues identified 4452 milnacipran-venlafaxine and 3761 milnacipran-amitriptyline matched pairs with similar pre-existing characteristics. 99 The unadjusted incidence rate ratios (IRRs) of any cardiovascular (CV) events, comparing milnacipran with venlafaxine or amitriptyline, were 1.02 (95% CI 0.73 to 1.44) and 1.30 (95% CI 0.90 to 1.89), respectively. Adjusted IRRs confirmed the statistical similarity in the CV event risk between milnacipran and venlafaxine (adjusted IRR = 1.29, 95% CI 0.76 to 2.17) or amitriptyline (adjusted IRR = 1.06, 95% CI 0.59 to 1.89). Thus, this French population-based study found that the risk of CV events was not significantly different for patients receiving milnacipran versus those receiving venlafaxine or amitriptyline. 99
Statistical analysis
Data on specific adverse events were abstracted from eligible studies, and summarized as pooled odds ratios using both the Mantel-Haenszel (M-H) fixed-effects and the random-effects model of Der-Simonian and Laird (D + L). Trials consisted of milnacipran 100 mg, and/or 200 mg doses. Milnacipran groups were combined for studies with more than one treatment arm. In the absence of statistically significant heterogeneity (P < 0.05), results were reported according to the fixed-effects model. Heterogeneity was investigated using I2 analysis to detect the magnitude variation attributable to heterogeneity rather than chance. A value below 25% was arbitrarily chosen to represent low levels of heterogeneity. The absolute risk reduction was calculated as the difference in the probability of any treatment emergent adverse event between the treatment and placebo groups. The reciprocal of the absolute risk difference was calculated to represent the number needed to treat (NNT) for one additional treatment emergent adverse event.
Results
Four trials met inclusion criteria for assessment of adverse events.70,71,92 These studies involved 4,610 total subjects (2,407 treatment + 2,203 placebo patients). The findings from the analysis of individual and treatment emergent adverse events are shown in Table 3 and Figure 4. Meta-analysis of the four studies yielded 3,816 patients (2,089 milnacipran, 1,727 placebo) with any treatment emergent adverse event occurring in 87% of milnacipran patients and 78% of placebo patients, or an absolute risk increase of 9% (NNT = 11). The pooled data for any treatment emergent adverse event (See Fig. 4) revealed an odds ratio of 1.8 (95% CI = 1.5, 2.1). No significant between-study heterogeneity (d.f. = 3, P = 0.3) was found. Pooled odds ratios for individual adverse events (See Table 3) indicated that milnacipran was associated with a statistically higher likelihood of constipation (5.1, 95% CI = 4.0, 6.6), dizziness (1.9, 95% CI = 1.5, 2.4), headache (1.3, 95% CI = 1.1, 1.6), hot flash (5.6, 95% CI = 3.0, 10.2), increased heart rate (6.9, 95% CI = 3.0, 15.9), hyperhidrosis (6.9, 95% CI = 4.9, 9.6), insomnia (1.3, 95% CI = 1.1, 1.6), nausea (2.4, 95% CI = 2.0, 2.7), and palpitation (3.3, 95% CI = 2.7, 4.5).
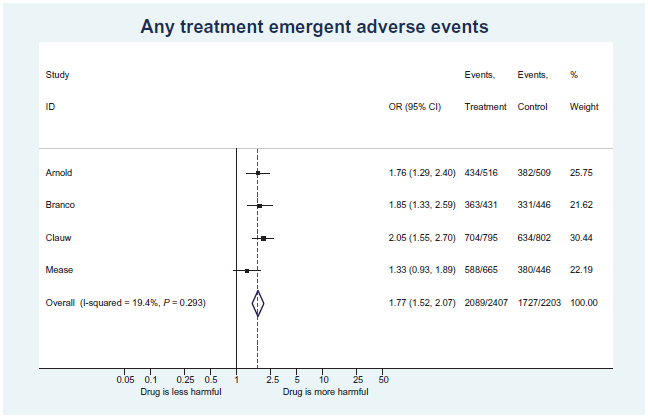
Forest plot of treatment emergent adverse events from placebo-controlled trials of milnacipran (n = 4,610).
Summary of adverse reactions showing pooled odds ratio from placebo controlled trials of milnacipran (n = 4,610).
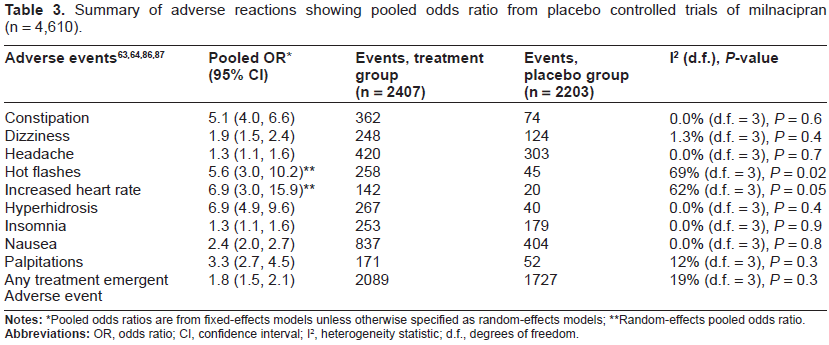
Pooled odds ratios are from fixed-effects models unless otherwise specified as random-effects models;
Random-effects pooled odds ratio.
Future Directions
In the future it is hoped that clinicians may be able to tailor therapy in efforts to target the primary patho/physiology present. Examining results from proton magnetic resonance spectroscopy of the brain, it appears that in a subpopulation of patients with FM, glutamate may be an especially relevant mediator in various molecular processes that may contribute to FM. 100 Conceivably, treatment strategies aimed at reducing glutamatergic activity in certain brain regions (eg, posterior cingulate cortex) may be beneficial in optimizing clinical outcomes.
Summary
Fibromyalgia is a central processing disorder associated with widespread pain, fatigue, sleep disturbances, cognitive difficulties, and somatic symptoms. The treatment of fibromyalgia involves patient education, cognitive behavioral therapy (CBT), and exercise/aerobic activities. The pharmacologic treatment of fibromyalgia may be extremely challenging. Despite having multiple agents to choose from, achieving significant and dramatic improvement in certain patients with fibromyalgia may not be possible. Milnacipran is an SNRI that inhibits the reuptake of norepinephrine more than inhibiting the reuptake of serotonin in a ratio of about 3 to 1 (and thus referred to by some as an NSRI). It is FDA approved in the US only for fibromyalgia. Multiple studies have demonstrated that both short-term and long-term milnacipran therapy are safe and efficacious for the treatment of fibromyalgia. It is beneficial not only for the pain component of fibromyalgia but also functionally and for a variety of other somatic symptoms/cognitive or sleep disturbances and fatigue. In part due to its preferential effects on inhibiting norepinephrine reuptake it is conceivable that milnacipran may be particularly useful for fibromyalgia patients who suffer from extreme fatigue as a predominant component of their fibromyalgia.
Author Contributions
Conceived and designed the experiments: HSS, PDM. Analysed the data: HSS, PDM. Wrote the first draft of the manuscript: HSS, PDM. Contributed to the writing of the manuscript: HSS, PDM. Agree with manuscript results and conclusions: HSS, PDM. Jointly developed the structure and arguments for the paper: HSS, PDM. Made critical revisions and approved final version: HSS, PDM. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.
Footnotes
Acknowledgements
The authors would like to acknowledge Pya Seidner for her great help in contributing to the preparation of this manuscript.