
Abstract
Strategies for preventing vision loss in patients with neovascular age-related macular degeneration (ARMD) have evolved over the past decade. Whereas earlier treatments were based on thermal destruction of choroidal neovascularization (CNV), new therapies rely on targeted pharmacologic approaches to reduce the harmful effects of CNV treatment. For the first time in the history of neovascular ARMD treatment, anti-VEGF therapies have consistently improved visual acuity in a subset of patients. Clinical trials continue to investigate the optimal dosing strategies and combination therapies to better refine the treatment of this chronic and debilitating disease.
Pathophysiology of ARMD
Age-related macular degeneration (ARMD) is the leading cause of visual impairment in patients over the age 60 in Europe and North America and is the third leading cause of blindness worldwide.1,2 The number of patients with macular degeneration will dramatically increase over the next few decades due to the aging population. ARMD is classified by two forms: “dry” (nonexudative) and “wet” (neovascular, exudative). In most cases of dry ARMD, patients do not experience significant visual loss. A small percentage of dry ARMD patients (7%-10%) will progress to the “wet” form, which is characterized by significant visual loss. The hallmark of ARMD pathology is drusen formation, which is an insoluble lipid deposit that accumulates between Bruch's membrane and retinal pigment epithelium (RPE). 3 Whereas dry ARMD is characterized by atrophy of the macular RPE and degeneration of photoreceptors, wet ARMD is characterized by choroidal neovascularization (CNV) and loss of photoreceptors and the RPE. Vascular endothelial growth factor (VEGF) has been proven to be a key potent stimulator in CNV formation 4 and is targeted in ARMD therapies. The risk factors for ARMD include: increased age, genetic markers and environmental factors (particularly smoking) with age being the strongest factor.5–7
The precise molecular mechanisms of AMD remains unknown, however, accumulated data from pathobiological, biochemical and genetic studies have prompted an integrated model. 8 This model states that aging is the primary factor with specific genetic variants exacerbating the pathogenesis along with environmental factors (smoking, etc). The initial step in ARMD pathogenesis is the natural aging process which causes oxidative stress and accumulation of drusen. Drusenoid material includes toxic substances that can trigger chronic inflammation and activate complement pathways. Chronic inflammation causes localized ischemia which stimulates VEGF production and resulting formation of choroidal neovascular membranes. Treatments to target pathogenic molecules (VEGF and inflammatory factors) are currently available and in the process of being developed.
Inflammation as a pathologic process in ARMD is well documented by the discovery of complement factor H polymorphisms as a risk factor for ARMD.9,10 Also, genome studies have identified a mitochondrial protein (ARMS2) which increases the susceptibility to ARMD.11,12 These studies support the role of genetic susceptibility and the variation of clinical presentation in different individuals and ethnic groups. In addition, environmental factors such as smoking, lack of an antioxidant-rich diet, hypertension and diminished immune system by chronic infection or inflammation, add another of layer of complexity to the pathogenesis of AMD.
With the advances in the understanding of the pathogenesis of AMD on the molecular level, progress in ARMD treatment has evolved from laser therapy and surgical procedures to verteporfin photodynamic therapy and anti-VEGF based molecular therapies. This review will focus on anti-VEGF therapies with a brief introduction to upcoming innovative therapeutics.
State of ARMD Therapy
Significant progress in the treatment of neovascular ARMD has occurred since the introduction of thermal laser photocoagulation for subfoveal CNVM. Although a select number of non-subfoveal lesions can be successfully destroyed by thermal laser photocoagulation, recurrences and symptomatic scotomas can occur. 13 Surgical removal of CNVM was investigated in the Submacular Surgery Trial (SST) and the findings showed poor visual and structural outcomes for subfoveal lesions. 14 Fortunately, since the introduction of photodynamic therapy (PDT), therapeutic approaches have shifted from ablative to more pharmacotherapeutic.13,15 Targeted pharmacologic therapy began with the first anti-VEGF molecule, an RNA aptamer, Pegaptanib (Macugen, OSI Eyetech), which specifically inactivates the pathologic VEGF165 isoform. Treatment with Pegaptanib allowed maintenance of vision without damage to the neurosensory retina. 16 Clinical trials and retrospective reviews have revealed that treatment of CNV with ranibizumab (Lucentis, Genentech) and bevacizumab (Avastin, Genentech) not only maintains visual acuity, but improves visual acuity in a significant number of patients. 17 The following sections summarize the pertinent data from ongoing clinical trials and review previous studies related to ARMD therapy.
Photodynamic Therapy
The efficacy of verteporfin (photoexitable dye) for the treatment of CNV was established in several studies including the Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) and the Verteporfin in Photodynamic Therapy (VIP) trials.15,18,19 In the TAP study, patients with some component of classic subfoveal CNV were treated with verteporfin or placebo. At one year, fewer eyes in the verteporfin group (39%) lost greater than 3 lines of vision (15 letters) than the placebo group (54%), (p < 0.001, the primary endpoint of the study). At 2 years this beneficial effect was maintained. 18 When the data was subdivided into predominantly classic lesions, the beneficial effect was greater in the treated group (38% lost greater than 3 lines of vision) than the placebo group (61%). No beneficial effect was seen in patients with minimally classic (<50% classic) CNV.
In the VIP study, patients with occult subfoveal CNV were treated with verteporfin or placebo. For the primary endpoint of loss of at least 15 letters, no difference was see between the verteporfin and placebo groups at 1 year. At two years, a beneficial effect was seen with 54% of verteporfin-treated patients losing 15 letters compared to 67% in the placebo group (p = 0.023). 19 Further analysis of the TAP and VIP data revealed that smaller lesions (<4 disc areas) lost less vision than larger CVN lesions. These studies concluded that small lesions size was a better predictor of visual acuity than lesion composition. 15 The most common adverse events associated with verteporfin therapy included back pain, injection site reaction, photosensitivity reaction and visual disturbance. Acute decreases in visual acuity (losing greater than 20 letters within 7 days of treatment) were reported in 0.7% of patients in the TAP trial and 4.4% of patients in the VIP trial. 20
Pegaptanib
Pegaptanib was introduced in 2004 as the first intravitreally administered anti-VEGF agent. 3 Pegaptanib is an anti-VEGF RNA aptamer that primarily targets the VEGF165 isoform to reduce vascular permeability and retinal neovascularization. 21 The VEGF Inhibition Study in Ocular Neovascularization (VISION) determined the efficacy and tolerability of pegaptanib. Patients were randomized to receive 0.3 mg, 1 mg or 3 mg of pegaptanib or sham injection every 6 weeks for 48 weeks. The results showed that all 3 doses of pegaptanib were significantly more effective than sham in achieving the primary endpoint (loss of fewer than 15 letters). Loss of less than 15 letters occurred in 70% of eyes treated with ranibizumab (0.3 mg) compared to 55% of sham eyes. Pegaptanib was found to be effective in maintaining vision, but only 6% of eyes gained 15 or more letters. This pivotal study showed that repeated intravitreal injections could be performed to maintain visual acuity in neovascular ARMD. Injection related adverse events were rare with endophthalmitis occurring in 1.3% of patients and traumatic injuries to lens or retina occurring in 0.6% of patients.
Bevacizumab (Avastin) and Ranibizumab (Lucentis)
To date, bevacizumab and ranibizumab are the most affective treatments for ARMD. These anti-VEGF antibodies provide pan- VEGF blockage rather than binding a single isoform of VEGF. In recent studies, the full-length monoclonal anti-VEGF antibody (bevacizumab) and antigen binding fragment (Fab) active site fragment (ranibizumab) have been shown to be highly effective at reducing vision loss. Results of the phase III clinical trials (ANCHOR, MARINA) for ranibizumab (Lucentis, Genentech) have shown stabilization or improvement of vision in 95% of patients, and improvement of ≥3 lines of vision in 40% of patients. 22 Off-label use of intravitreal bevacizumab (Avastin, Genentech) has been shown to significantly improve vision in several studies.23–25 A recent survey of practicing retinal specialist by the American Society of Retinal Specialists (ASRS) (Preferences and Trends, 2007) show that 50% of retinal specialist use ranibizumab as first line therapy and 50% use bevacizumab as first line therapy for treatment of CNV lesions (ASRS 2007 Preferences and Trends, Membership Survey, R. Mittra).
Ranibizumab and Pivotal Clinical Trials
Marina
Ranibizumab is a humanized antigen binding fragment (Fab) designed to block all active forms of VEGF. 26 In 2006, ranibizumab was approved for the treatment of subfoveal CNVM. MARINA (Minimally Classic/Occult Trial of the Anti-VEGF Antibody Ranibizumab in the Treatment of Neovascular AMD) enrolled patients with minimally classic or occult (lesions with presumed recent disease progression. 17 Patients were randomized to sham or ranibizumab intravitreal injection (0.3 mg or 0.5 mg) every 4 weeks for 24 months. The primary outcome was loss of less than 15 letters. At one year, the results showed that 95% of eyes treated with ranibizumab (0.3 mg and 0.5 mg) lost less than 15 letters compared to 63% of sham eyes (Fig. 1). In addition to maintenance of visual acuity, treatment with ranibizumab showed significant gains in visual acuity with 25%-34% of eyes (0.3 mg and 0.5 mg doses) gaining 15 letters at 12 months. The mean gain in visual acuity at 12 months was 7.2 letters compared to a loss of 10 letters in the sham group. At 24 months, this effect was maintained in the ranibizumab group with an average gain of 6 letters compared to a 15 letters loss in the sham group (difference of 21.5 letters) 17 (Fig. 1). Adverse events including endophthalmitis and retinal detachment were rare. Systemic adverse events were no different in ranibizumab and sham groups including hypertension, death, myocardial infarction and cerebrovascular events.
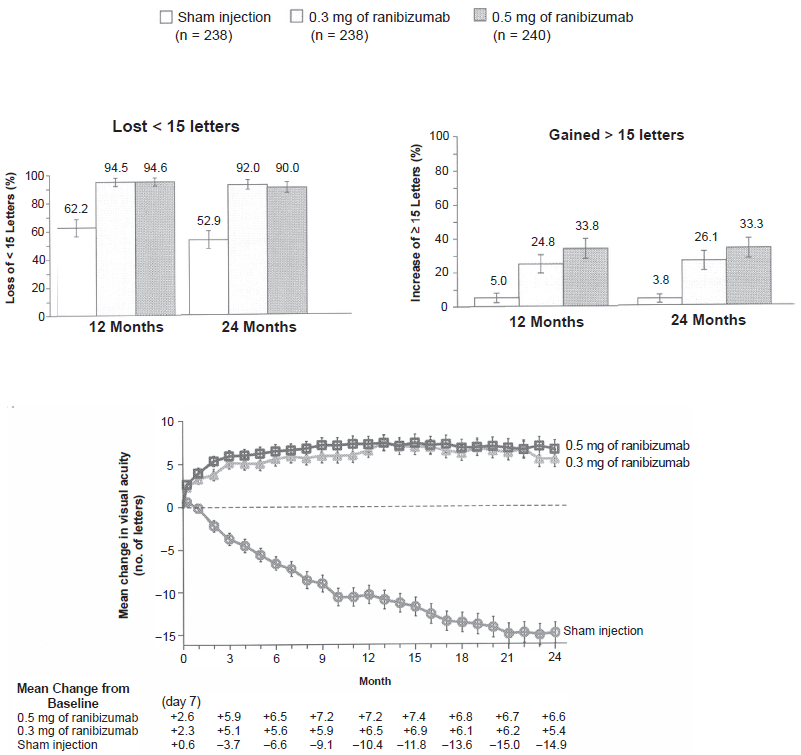
Data from MARINA trial. Top: Percentage of patients in each group who lost less than 15 letters (left) or gained 15 or more letters (right). Bottom: Mean change from baseline visual acuity during a 24 month period. Comparison between the ranibizumab groups (0.3 mg and 0.5 mg) and sham is shown below chart.
Anchor
ANCHOR (Anti-VEGF Antibody for the Treatment of Predominantly Classis Choroidal Neovascularization in AMD) enrolled patients with predominantly classic CNV for randomization into 3 groups: PDT with sham injection of ranibizumab, sham PDT with ranibizumab 0.3 mg or sham PDT with ranibuzumab 0.5 mg. The primary outcome was loss of less than 15 letters at 12 months. The study found that 94%-96% of ranibizumab injected eyes (0.3 mg and 0.5 mg, respectively) lost less than 15 letter compared to 64% of eyes treated with PDT alone (p < 0.0001). 27 A gain of > 15 letters was present in 40.3% of eyes receiving ranibizumab and 5.6% of eyes receiving PDT (Fig. 2). The mean change in visual acuity was an 11 letters gain with ranibizumab compared to a 9.5 letter loss with PDT treatment at 12 months (20.8 letter difference). Subgroup analyses showed that the benefit of ranibizumab over PDT for predominately classic lesion was present regardless of patients’ age, visual acuity or lesion size. 28
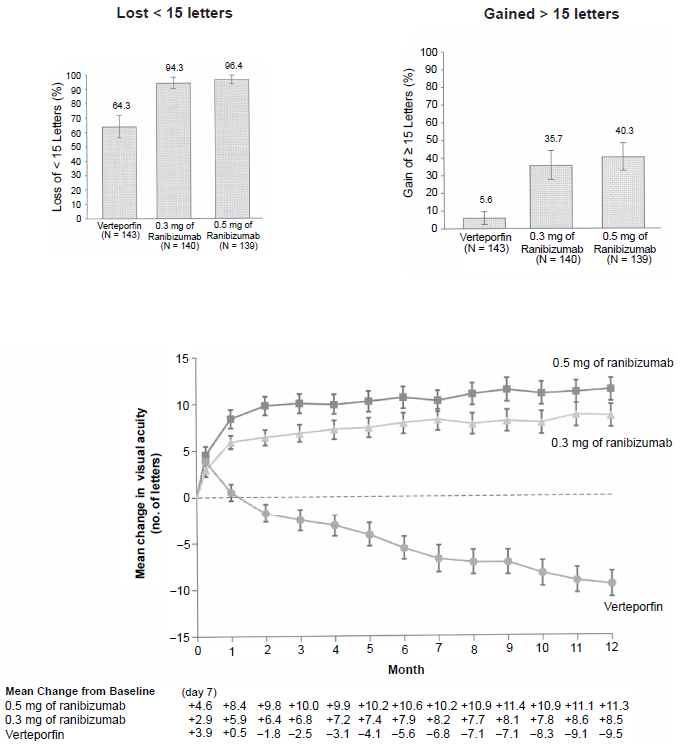
Data from ANCHOR trial. Top: Percentage of patients in each group who lost less than 15 letters (left) or gained 15 or more letters (right). Bottom: Mean change from baseline visual acuity during a 12 month period. Comparison between the ranibizumab groups (0.3 mg and 0.5 mg) and sham is shown below chart.
Alterante Dosing Strategy: prONTO Study
The PrONTO study (Prospective OCT Imaging of Patients with Neovascular AMD Treated with Intraocular Ranibizumab) is a 2-year, open-label, prospective study to evaluate an OCT guided dosing regimen. 29 The study enrolled patients to receive 0.5 mg of ranibizumab monthly for 3 months with additional reinjection if: loss of >5 letters, OCT evidence of fluid defined as subretinal fluid or retinal cysts, increase in OCT thickness of >100 microns, new macular hemorrhage, or new CVN. Reinjection also occurred if fluid persisted following a previous injection. Major endpoints examined were changes in visual acuity and OCT thickness from baseline after treatment and the number of injections required over 12 months. Other endpoints included the number of consecutive monthly injections to achieve a fluid free macula and the time to next injection due to fluid recurrence.
The most common criteria for reinjection was vision loss, a fluid increase of > 100 microns on OCT and persistent fluid following the last injection. Of the 40 eyes enrolled, 7 eyes did not require another injection after the initial 3 injections and 8 eyes required only 4 injections. The mean number of injections was 5.6 in 12 months. Visual outcomes were similar to those seen in the MARINA and ANCHOR trials (Fig. 3). Of the 40 patients, 95% lost <15 letters and 35% gained 15 or more letters (mean 9.3 letters). OCT outcomes resulted in a mean reduction in thickness of 178 microns. The authors found that development of any of the retreatment criteria was preceded by OCT changes suggestive of early fluid. Although these results are comparable to MARINA and ANCHOR, this study was smaller, nonrandomized, open-label, and unmasked.
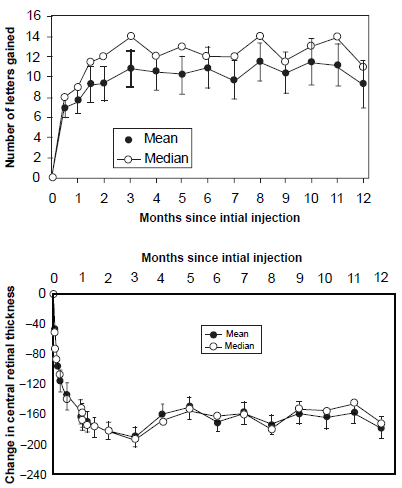
Data from PrONTO trial. Top: Mean and median change in visual acuity through 12 months. Bottom: Mean and median change in the optical coherence tomography (OCT) central thickness through 12 months.
Clinical Trial Data Provides “Guidelines”
Dosing strategies
Two dosing strategies have been proposed using clinical trial data and ancillary testing data to monitoring efficacy and guide decision-making. “Strategy A” adheres to the clinical trial protocol with “automatic” monthly injections for 24 months without the use of FA or OCT to guide retreatment decisions. FA and OCT are only obtained to evaluate adverse events if unexplained vision loss occurs. Pitfalls of this approach include the potential for overtreament considering the known risks of intravitreal injection, patient discomfort and inconvenience, possible toxicity by blocking the neurotrophic effects of VEGF with prolonged VEGF blockade and societal costs. “Strategy B” is a tailored, more labor intense approach that requires synthesis of all available data (exam, FA and OCT). Monthly injections are performed for 3 months (similar to MARINA, ANCHOR, PrONTO), followed by monthly imaging studies which are used to guide the need for retreatment until the lesion is considered inactive. Once considered inactive, patients are then closely monitored with clinical exams, FA and OCT imaging. Pitfalls include possible undertreatment, the difficulty of determining when a lesion is completely inactive, and the “off label” use of the prescribed medication.
CATT Trial
Bevacizumab (Avastin) and Ranibizumab (Lucentis) appear to be similarly effective, and currently the CATT clinical trial (Comparison of AMD Treatment Trial) is a multicenter trial sponsored by the National Eye Institute which directly compares the effectiveness of Avastin and FDA approved Lucentis. Monthly dosing and “as needed” dosing will be compared in this 2-year study. We are currently awaiting the results of the study.
Future Treatments
Because of the need for repeated intravitreal injection in the above treatments, newer therapeutic agents with longer half-life, high potency, minimal systemic side effects, and less invasive administration are being investigated. The following is a brief introduction to a few promising new agents.
VEGF Trap (Regeneron pharmaceuticals, inc)
VEGF Trap-Eye is a recombinant fusion protein of the Fc domain of human IgG1combined with a VEGF binding domain of human VEGF receptors 1 and 2. 30 Similar to bevacizumab and ranibizumab, it binds to all isoforms of VEGF. The key feature is a very high binding constant for VEGF, which is even higher than native VEGF receptors. This property leads to high potency and longer duration of action, suggested to last for 10 weeks. 31 Although repeated intravitreal injections are required for administration, the longer duration of action is favorable. Systemic administration has been show to cause multiple side effects, 32 which have not been observed following intravitreal injection. In a recent phase I trial, 5 patients with diabetic macular edema received one-time intravitreal injection. Results showed improvements in excess foveal thickness and median improvement of three letters. 33 Patients tolerated the injection and the results demonstrated bioactivities of VEGF Trap-Eye. Testing with repeated injections for longer-term will be the next step in evaluating its potential as a therapeutic agent for ARMD.
NT-501 (Neurotech pharmaceuticals, inc.)
NT-501 is an intraocular polymeric implantable device containing modified human retinal pigment epithelium cells transfected with modified ciliary neurotrophic factor (CNTF) gene. 34 The semipermeable membrane of the transplant allows diffusion of the CNTF protein to the intraocular space, while allowing the exchange of nutrients and waste products to sustain the viability of the cells. This delivery device circumvents the blood-retina barrier and the immune attack on implanted cells. The phase II clinical trial in 51 subjects with progressive geographic atrophy revealed stabilization of visual acuity of 97% of patients compared to 70% of controls at 12 months.
Fenretidine
Fenretidine inhibits of vitamin A delivery to the eye by displacing retinal-binding protein in the blood. 35 It has been undergoing phase II clinical trials for dry ARMD. This trial is based on an original study that fenretinide can block the formation of lipofusion pigments in the retinal pigment epithelium in recessive retinitis pigmentosa knockout mice model.36,37 Fenretidine is an oral agent that is used for the treatment of certain cancers and its role as a treatment for macular degeneration is being investigated.
Other investigational therapies
Sirolimus (rapamycin) is an immunosuppressive agent that inhibits the response of IL-2. The efficacy of this molecule in the treatment of exudative ARMD is being investigated in a Phase II study of ocular Sirolimus in combination with Ranibizumab (EMERALD study). “Double” and “triple” therapies using a combination of anti-VEGF agents, low fluence photodynamic therapy, intravitreal dexamethasone and external beam radiation have shown promise.39,40
Conclusion
Age-related macular degeneration is a chronic, vision threatening and increasingly prevalent disease. Although current therapies have dramatically changed visual outcomes of patients with this disease, future clinical trials and new therapies are necessary to address prevention and better refine early treatment of this chronic and debilitating disease.
Disclosure
The authors report no conflicts of interest.