
Abstract
Recurrent upper respiratory infections caused by respiratory syncytial virus (RSV) and other respiratory viruses occur throughout life. During the first 2 years of life, RSV infected children have up to a 40% risk of a lower respiratory tract infection (LRTI). In turn LRTI, including bronchiolitis, due to RSV is the most common cause of hospitalization among infants less than one year of age. While mortality from RSV infection has fallen over the last 2 decades, approximately 400-500 deaths occur annually in the United States again primarily in infants less than 1 year of age. Palivizumab, a humanized monoclonal antibody, has been shown to reduce the risk of hospitalization in high risk infants if given monthly during RSV season. Post marketing safety surveillance originating from a variety of sources, mostly active surveillance, has confirmed the prelicensure safety profile of palivizumab. Other than very rare anaphylactic reactions (<1/100000), no significant adverse reactions have been noted.
Introduction
Epidemiology
Recurrent upper respiratory infections caused by respiratory syncytial virus (RSV) and other respiratory viruses occur throughout life. During the first 2 years of life, 90% of children are infected with RSV and up to 40% will have a lower respiratory tract infection (LRTI). 1 LRTI, including bronchiolitis due to RSV, is the most common cause of hospitalization among infants less than one year of age, more than 100,000 per year.2,3 While mortality from RSV infection has fallen over the last 2 decades, approximately 400-500 deaths occur annually in the United States3,4 primarily in infants less than 1 year of age. 5
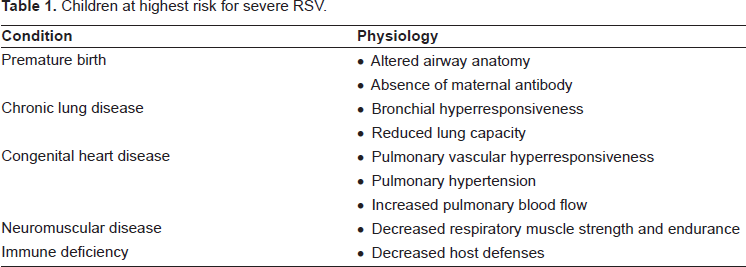
In the Northern hemisphere, RSV infection occurs most often in the winter months but there is considerable variability in seasonal onset and duration, particularly in the Southeastern United States and Puerto Rico.6–8 In the latter locations significant RSV activity exists in the summer months. Further, in the Southern regions of the country, RSV season begins earlier and may extend into April. There even can be substantial variation in seasonality within the same community from one year to the next. 6 The adult population and day care facilities serve as reservoirs of infectivity.9,10 The most vulnerable population, those infants from birth to one year of age with chronic lung disease, neuromuscular disease or airway anomalies, or hemodynamically significant congenital heart disease are at highest risk for severe disease and hospitalization.11,12
Virology
RSV is a single stranded RNA pneumovirus of the Paramyxoviridae family. All pneumoviruses encode two major surface glycoproteins (G and F), which are incorporated in the virus particle. 13 The attachment G protein binds the virus to the cell receptor and the F protein mediates fusion of cell and viral membranes essential for viral penetration into the cell. The G protein is the most variable gene product among human RSV isolates, and antigenic differences detected with monoclonal antibodies specific for the G protein have been used to classify human RSV isolates into two groups, A and B. Sequence identity at the amino acid level is only 53% between the G proteins of the prototype strains of groups A and B, and up to 20% sequence variation has been observed among the G proteins of human RSV isolates of the same antigenic group. However, the F protein is conserved across all isolates.13,14 Antibodies to the F protein may either directly neutralize virus or block entry into the cell.
Transmission
RSV is transmitted by droplets, large particles, and contact with fomites. It can survive for as long as 6 hours on stethoscopes, and up to 12 hours on hard, nonporous surfaces.15,16 More than 50% of medical personnel are infected when RSV is prevalent in the community.16,17
Pathophysiology
During a 5-day incubation period, the virus replicates in the nasal mucosa, reaching titers of 10 6 in young infants, and then spreads to the bronchial epithelium. In both vitro and in vivo models of LRTI, RSV causes an exaggerated nuclear factor (NF)-kappaB activation and subsequent elevated cytokine and chemokine production18–22 resulting in acute inflammation, edema and epithelial cell necrosis. Symptoms are related primarily to the increased mucus production and bronchospasm. NF-kappaB dimmers exist as inactive complexes in the cytoplasm of unstimulated cells by virtue of their interaction with inhibitory proteins (IκBs). These inhibitory proteins are phosphoralated by cellular kinase complexes. This appears to be regulated through activation of the IkappaB kinase alpha (IKK-α) in lung tissue. RSV infection activates IKK-α and IKK-β. 20 Respiratory viruses also can cause induction of inflammatory cytokines in human bronchial cells by activation of the p38 MAPK pathway. 23 RSV infection inhibits granulocyte apoptosis via kinase and NF-kappaB dependent mechanisms. 24 In the mouse model, RSV infection causes increased expression of inducible nitric oxide synthase and nitric oxide production adding to the inflammatory burden. 25 This inflammatory cascade results in long term airway obstruction, and chronic inflammatory infiltrates associated with long-term airway hyper-responsiveness (up to 154 days). 26
Prevention
Both prevention and treatment options for RSV disease were limited until studies demonstrated that passive administration of high-titer RSV IGIV reduced both the incidence and severity of RSV LRTI in high risk infants. 27 While RSV-IGIV proved effective, its use was accompanied by several limitations related to the time required for intravenous administration and the relatively large volume of fluid required for each dose. During the same period that RSV-IGIV was being studied, several investigators worked to develop an effective monoclonal antibody (MAb) against RSV. Tempest et al. developed a humanized MAb to a linear epitope of RSV 28 and Barbas and co-workers reported the isolation of a RSV specific human Fab fragment from an Escherichia coli phage display library. 29 Both of these compounds demonstrated neutralizing properties against RSV. Johnson et al. in a series of experiments, demonstrated that MEDI-493 (palivizumab), a humanized monoclonal antibody composite of human (95%) and murine (5%) antibody sequences (IgG1 k) had potent neutralizing and fusion inhibition capacity and reacted with a majority of clinical isolates of both A and B serotypes studied. 30 In the murine model, palivizumab, when given 24 hours prior to RSV inoculation, has been shown to reduce RSV replication in the lung and decrease pulmonary histopathologic scores, airway obstruction measured by plethysmography, and airway hyper-responsiveness after methacholine challenge, as well as reducing the inciting inflammatory markers, compared to untreated controls. 31
Palivizumab Mechanism of Action, Metabolism and Pharmacokinetic Profile
Mechanism of action
The effectiveness of MAbs depend upon their being human or humanized to retain appropriate pharmokinetics and to avoid generating a human anti-mouse antibody response, given the need to administer repetitive doses throughout the RSV season. The murine sequences in palivizumab were derived from a murine monoclonal antibody, Mab 1129 32 in a process that involved the grafting of the murine complementarity determining regions into a human antibody frameworks. The human heavy chain sequence was derived from the constant domains of human IgG1 and the variable framework regions of the V H genes Cor 33 and Cess. 34 The human light chain sequence was derived from the constant domain of C k and the variable framework regions of the V L gene K104 with J k -4. 35 Palivizumab is composed of two heavy chains and two light chains and has a molecular weight of approximately 148,000 Daltons. It acts by binding to the A antigenic site of the F protein thus preventing viral replication without enhancement of virus infectivity. 30
Metabolism
Proteins, such as IgG, continuously circulate from the vascular system to the extravascular fluids and tissue and then return to the vascular system through the lymphatic system. As the pharmakinetics of palivizumab resemble those of IgG1, 36 its metabolism should follow. IgG1 moves in and out of cells via transcytosis mediated by the Fc receptor, FcRn, found primarily in endothelial cells.37,38 FcRn binds to Ch2-Ch3 hinge region of IgG only at an acidic pH; it releases at a neutral pH.37–39 Following fluid phase uptake into acidic endocytic vesicles, the IgG-FcRn complex can be transported across the cell and the IgG can be released upon fusion of the vesicle with the basolateral cell surface at near neutral pH. If IgG is not bound to FcRn, it is subject to intracellular catabolism via lysosomal degradation. Thus, the intracellular binding by FcRn acts to prolonged IgG serum half life.
Pharmacokinetic profile
Palivizumab serum concentrations of ≥40 μg/mL reduce pulmonary RSV replication in the cotton rat model of RSV infection by 100-fold.
30
The
Clinical Studies: Safety
In the phase I/II multicenter, randomized, double blind, placebo controlled dose escalation trial by Subramanian et al. safety and tolerance of intravenous MEDI-493 were assessed. They demonstrated that up to 15 milligrams per kilogram was well tolerated and safe in the population studied (premature infants born 35 weeks gestation or less who were 6 months or younger and infants with bronchopulmonary dysplasia who were 24 months or younger). 41 A comparable phase I/II multicenter, open label, escalating dose clinical trial that involved a similar patient population also found that intramuscular administration of dosages up to 15 milligrams per kilogram given were also safe and well tolerated. 36 Saez-Llorens and colleagues, in another multicenter, randomized, double-blind, placebo-controlled, escalating dose clinical phase I/II trial, further examined the safety, tolerance, pharmacokinetics and clinical outcome of a single intravenous dose of palivizumab in previously healthy children equal to or less than 2 years of age hospitalized with acute RSV infection. No significant adverse events were found due to the study drug. 44
The safety of palivizumab was more extensively evaluated in the large cohort that comprised The Impact-RSV study. 45 Once again, palivizumab was felt to be safe and well tolerated with no significant differences between reported adverse events between the palivizumab (11%) and placebo (10%) groups. The most common adverse events of fever, nervousness, and injection site reactions were not statistically significant between the two groups. Injection site reactions occurred 2.7% in the palivizumab group and 1.8% in the placebo group. These types of reactions were overall mild and short in duration, none being serious. Mild to moderate elevations of transaminases occurred in both groups; however, hepatic and renal adverse events were similar in both groups when evaluated by blinded investigators. The discontinuation rate secondary to related adverse events was 0.3%. Five (1.0%) children in the placebo group and 4 (0.4%) in the palivizumab group died during the trial; no death was judged related to palivizumab. 45
A follow-up study involving 56 high-risk infants who participated in the Impact-RSV study evaluated the safety of palivizumab in a second RSV season. 46 These infants received a 5-dose course, 15 mg/kg/dose, over a five month period. No local or systemic immune mediated responses were found. One child had an anti-palivizumab titer of >1/40 after the start of dosing with no associated serious adverse effects and appropriate trough palivizumab levels. Prior to completion of the 5 does course the titer had fallen to 1/10 by study day 120. 46
Palivizumab safety also has been specifically examined in infants equal to or less than 30 weeks’ gestation. No serious adverse reactions or significant hepatic and renal functions were associated with palivizumab injections. Local reactions such as indurations, erythema, and bruising at the site of injection were observed in 28%; resolving within 24 to 48 hours. 42
In patients with congenital heart disease, adverse events were similar in the treatment groups with no child discontinuing the study secondary to a drug related event. Serious adverse events were statistically decreased in the palivizumab recipients with 55.4% occurrence versus 63.1% in the placebo group. No differences in rates of earlier-than-planned or urgent cardiac surgeries were seen between the 2 groups. Mortality rates were 3.3% for the palivizumab group and 4.2% in the placebo group (p 0.463) with no deaths attributed to palivizumab. 43
Romero estimated in 2003, that >250,000 infants have received >1 million doses of palivizumab prophylaxis in the 4 years subsequent to the Food and Drug Administration approval of palivizumab. 47 Post marketing safety surveillance originating from a variety of sources, mostly active surveillance, has confirmed the prelicensure safety profile of palivizumab. Other than very rare anaphylactic reactions (< 1/100 000), no new serious adverse events and no evidence of increased rates of severe adverse events or death were observed in the post marketing data.47–49
Unlike RSV immunoglobulin intravenous (RSV-IGIV) which required a 9 month delay of live vaccines after dosing, palivizumab, when administered concurrently, has shown no crossre-activity with measles-mumps-rubella and varicella vaccines. 50
Clinical Studies: Efficacy
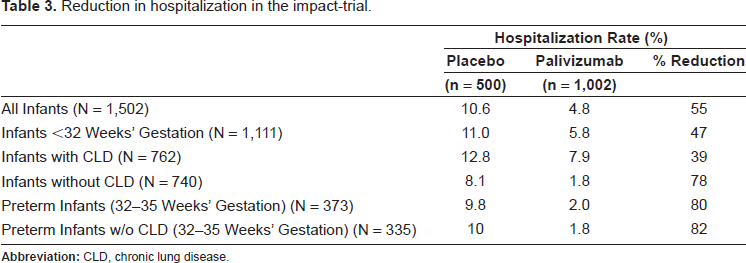
The Impact-RSV Study Group study, performed during the 1996 to 1997 RSV season, is the largest randomized (2 treatment to 1 control) double-blind, placebo-controlled, phase 3 trial to evaluate both safety and efficacy of palivizumab prophylaxis. 45 It involved 139 centers in the United States, the United Kingdom, and Canada and enrolled 1,502 children ≤35 weeks’ gestation with prematurity (6 months of age or younger) or bronchopulmonary dysplasia (24 months old or younger) who were randomized to monthly intramuscular injections for 5 months of either palivizumab (15 mg/kg) or placebo. Patients were subsequently followed until one month after last injection. All five scheduled injections were given to 93% of the children. The results demonstrated a 55% RSV related reduction in RSV hospitalization (10.6% placebo vs. 4.8% palivizumab.) Infants with prematurity plus BPD had a 39% reduction (12.8% vs. 7.9%) and those with only prematurity as a risk factor had a 78% reduction (8.1% vs. 1.8%). In the palivizumab group, the hospitalized children were also noted to have fewer hospital days, fewer hospital days with oxygen administration, fewer days with moderate/severe lower respiratory tract infection, and a lower incidence of intensive care admission. There was no statistically significant reduction in the number of deaths, those requiring mechanical ventilation or total days of mechanical ventilation, non RSV related respiratory hospitalizations or otitis media. The efficacy of the prophylaxis remained statistically significant after logistic regression was performed analyzing gender, entry age, entry weight, BPD, and gestational age or when comparing different countries. 45
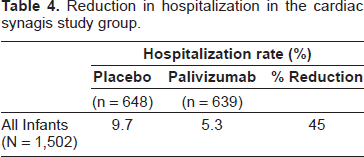
The efficacy of palivizumab prophylaxis has also been evaluated in hemodynamically significant congenital heart disease children, less than 2 years of age. In a randomized, double- blind, placebo-controlled trial of 1,287 randomly assigned children, a 45% relative reduction in RSV hospitalization (9.7% in the placebo group vs. 5.3% n the palivizumab group) was found. 43 The reduction was evident in both cyanotic and acyanotic patient groups when examined as a whole. Although when cyanotic infants were compared to acyanotic ones, the reduction was only statistically significant in the acyanotic stratum, the study was not powered to detect differences between these two groups. Reduction in RSV hospitalization days and days with an increased oxygen requirement were also statistically lower in the palivizumab group. Incidence and days of RSV-associated intensive care and mechanical ventilation were not statistically different. 43
Multiple long term observational studies also have confirmed the continued low rate of RSV hospitalization following passive immunization with palivizumab.47,49,51,52
Long term respiratory benefits may also occur in preterm infants without chronic lung disease receiving palivizumab. A cohort of preterm infants who were not hospitalized for RSV but had received palivizumab (191) compared with a group of infants who had never received palivizumab (76 who had had RSV hospitalizations and 154 who had not) were prospectively followed over a 2 year period. Even with adjustment for potential confounding variables, the incidence of recurrent wheezing and physician diagnosed recurrent wheezing were significantly lower in the palivizumab-treated infants (13% and 8% respectively) versus all 230 untreated infants of 26% and 16% respectively and when only looking at those 154 without RSV hospitalization (23% and 16% respectively). 53 Paradoxically, high maternal RSV neutralizing antibodies have been associated with an increased risk of recurrent wheeze. 54
Place in Therapy
As there are no effective treatment options except supportive care, prevention is critically important in a vulnerable population. Hand washing is the most important factor to limit the spread of RSV in healthcare, school, and daycare settings.55,56 Careful handling of contaminated items and cohorting of infected individuals can be helpful in the hospital setting. Hospital visitors, especially young children, should be screened for the presence of an URI and, if found, prevented from visiting.57,58
Immunoprophylaxis
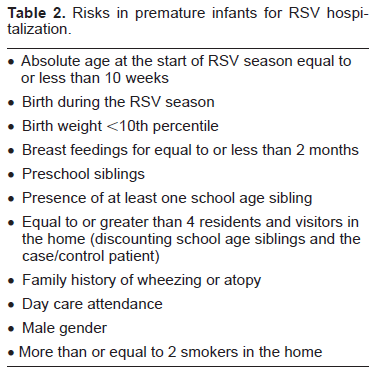
Certain factors are associated with the development of more severe disease (Table 1),59,60 and risk of hospitalization (Table 2).53,61–63 In these high risk groups, the use of immunoprohylaxis has been advocated as a means of decreasing disease burden. 64 While palivizumab does not prevent RSV infection, randomized controlled trials examining certain high risk infants have shown that palivizumab significantly reduces the risk of hospitalization due to RSV: those infants with bronchopulmonary dysplasia (BPD), infants with a history of premature birth (≤35 weeks gestational age), and children with hemodynamically significant congenital heart disease (CHD).43,45 (Tables 3 and 4). This is particularly true in premature infants between 32 and 35 weeks’ gestation where the reduction in hospitalization may approach 80 per cent (Table 3). 45 Palivizumab is not effective in ameliorating or preventing illness due to other respiratory viruses.
Children at highest risk for severe RSV.
Risks in premature infants for RSV hospitalization.
Reduction in hospitalization in the impact-trial.
Reduction in hospitalization in the cardiac synagis study group.
Current American Academy of Pediatrics’ recommendations suggest that prophylaxis be considered in infants with chronic lung disease (CLD) or hemodynamically significant congenital heart disease (CHD) for up to 2 years following birth as well as others born prematurely. 1 (Table 5) Prophylaxis should be started before the RSV season and continued throughout the season, including those infants who develop an RSV infection as different strains may be present.
2003 American academy of pediatrics palivizumab administration guidelines.
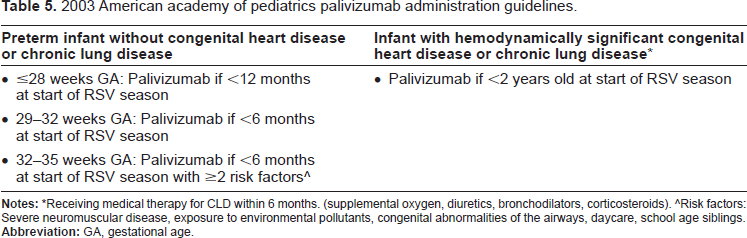
Receiving medical therapy for CLD within 6 months. (supplemental oxygen, diuretics, bronchodilators, corticosteroids).
Risk factors: Severe neuromuscular disease, exposure to environmental pollutants, congenital abnormalities of the airways, daycare, school age siblings.
Palivizumab requires monthly injections to be given during the RSV season and high parental compliance. Cost is also a consideration. If a direct cost analyses are performed, most suggest that there are no direct cost savings related to hospitalization or ambulatory care in preterm infants, or in those infants with congenital heart disease.65–67 This has led to recommendations to limit the use of palivizumab to those infants at highest risk (e.g. less than or equal to 32 weeks’ gestation)68–72 or who have specific risk factors.61–63,73 However, if an analysis of prematurely born infants (≤35 weeks’ gestational age), those with bronchopulmonary dysplasia (BPD), and children with congenital heart disease (CHD) is undertaken using a decision tree model developed employing multiple data sources (published literature, palivizumab clinical trials, and national population statistics) with the comparator being no prophylaxis, a different result is found. Two recent studies, one using United Kingdom NHS funding data and the other Austrian Health Insurance Fund information found benefit from palivizumab prophylaxis. In these societal perspective scenario analyses, the future lost productivity of a child resulting from RSV-related mortality (indirect costs) were also included as well as the cost of administration of palivizumab, hospital care for RSV infections and the cost of asthma treatment. The analyses were based on a lifetime follow-up period in order to capture the impact of palivizumab on long-term morbidity and mortality resulting from an RSV infection. Both studies suggest that palivizumab prophylaxis against severe RSV infection in high risk infants may be cost effective (vs. no prophylaxis), and that the positive clinical and economic benefits may persist beyond one RSV season.74,75
There are only anecdotal reports regarding the use of palivizumab to modify or prevent nosocomial RSV infection in high risk patients;76–78 no controlled trials using this approach have been published. Therefore, present recommendations do not include the administration of palivizumab for those situations. 1
In virtually all term infants, palivizumab is not usually an option and the importance of good hand washing, avoidance of day care, tobacco smoke, and school age siblings are the most important concepts to communicate to the child's primary and secondary caregivers.
Palivizumab use in other populations
Infants with cystic fibrosis (CF) are at high risk to develop serious RSV lower respiratory tract infection (LRTI). Hospitalization rates have been reported to be between 8.75% to 14.6%79,80 and long term pulmonary sequelae are common. 79 These rates are comparable to those for children with bronchopulmonary dysplasia.81,82 RSV LRTI also may play a role in the initial Pseudomonas colonization and the decline in pulmonary function in these patients. 83 Two retrospective studies have been conducted, one large and one small. Both suggest that palivizumab may reduce hospitalization due to RSV infection.84,85 The larger study involved 91 CF infants who were enrolled in a prospective, observational registry 52 designed to collect data on the demographics, risk factors, clinical characteristics, and outcomes of infants and young children who received palivizumab from 2000-2004. None of the CF infants were hospitalized due to RSV infection. This finding was significant when compared to historical controls. 85 There is little research available regarding the use of palvizumab in other populations aside from two phase 1 safety studies that have been performed in hematopoietic stem cell transplant recipients. 86
Vaccines
The first vaccine to prevent RSV disease was produced in the mid 1960s. It had the unfortunate adverse outcomes of not protecting against RSV infection and caused vaccine enhanced disease during the next RSV infection. 87 This was shown to be secondary to immune potentiation. A number of live attenuated vaccines have been produced since including host range mutants, cold-passaged mutants, and temperature-sensitive mutants; none have been totally successful. 64 Subunit vaccines based upon a purified F protein have shown the greatest promise and have been evaluated in phase I–II clinical trails with demonstrated immunogenicity and safety.88,97 However, the immunogenicity has been shown to be only modestly better that RSV infection itself. In a trial in children with cystic fibrosis, immunogenicity and safety were shown, but LRTIs were not prevented. 88 G subunit vaccines also have been examined, but do not appear to provide lasting immunity to any degree. 89 Other subunit vaccines have been considered, but likewise do not protect adequately. 64 A recently developed Sendai virus (SV) based vaccine has demonstrated in preclinical studies that intranasal vaccinations with recombinant SV expressing an RSV antigen are sufficient to activate high-magnitude RSV-specific neutralizing B- and T-cell activities in a cotton rat system. Furthermore, vaccinated animals are completely protected against RSV challenges. 90
Treatment
Treatment is primarily supportive and includes hydration, clearance of secretions, careful monitoring of oxygen saturation, supplemental oxygen as required, and if necessary, mechanical ventilation. In considering antiviral treatment of acute RSV infection, familiarity with typical viral load dynamics during the course of a lower respiratory tract infection is vital in the therapeutic decision process. For example, in a patient who has had airway obstruction and other respiratory symptoms for >3 days the viral load has already peaked and any currently available antiviral therapy will be ineffective.
Currently there is only one licensed antiviral agent, ribavirin. Ribavirin is a broad spectrum antiviral agent that inhibits viral multiplication through a number of mechanisms. 64 A recent review of 11 randomized controlled trials of ribavirin treatment for RSV infection yielded decidedly mixed results as to ribavirin's effectiveness. 91 Even in those studies that reported benefit, the benefit was marginal for most patients. However, in certain high-risk patients (e.g. patients who are immunocompromised or have significant cardiopulmonary disease) who have severe documented RSV bronchiolitis, ribavirin may be indicated. 10 Other antiviral agents are under investigation in cell culture and animal models, but have not been used in humans and are still considered experimental. 64 Corticosteroids 92 or anticholinergic agents (e.g. ipratopium) 64 are not indicated in the treatment of RSV bronchiolitis as neither have shown any benefit. Bronchodilators, including epinephrine, albuterol, and salbutamol, in certain select populations, may have a beneficial short-term effect on wheezing. 10 Recent recommendations have suggested that epinephrine may be the preferred agent in the outpatient setting, 10 but documented improvement must be demonstrated to justify continued bronchodilator use. In the absence of a clinical response, this mode of therapy should not be continued. One study has shown benefit of a leukotriene antagonist in children with bronchiolitis in preventing subsequent wheezing when treated during the acute episode. 93 This small randomized controlled trial (N = 130) demonstrated on follow-up that those patients treated with montelukast were free of symptoms 22% of the days and nights compared to 4% of the days and nights treated with the placebo. However, in a larger multi-center, double-blind study of 3- to 24-month-old children who had been hospitalized for a first or second episode of physician-diagnosed RSV bronchiolitis and who tested positive for RSV, [N = 979], leukotriene at a similar dose did not provide any improvement in their respiratory symptoms post-RSV illness. 94 No treatment studies showing efficacy have been reported using palivizumab, except a retrospective chart review series reported by Chávez-Bueno and colleagues. 95
Conclusions
Palivizumab immunoprophylaxis, when given monthly throughout the RSV season, reduces the severity of RSV LRTI in certain categories of infants and decreases the risk of hospitalization for that population. Palivizumab administration may also decrease subsequent recurrent wheezing. Cost-benefit analyses have provided mixed results; thus, national organizations have adopted a number a strategies for its use, focusing on infants at most risk for severe disease.
Disclosure
The authors report no conflicts of interest in this paper.