
Abstract
Angiotensin-converting enzyme (ACE) inhibitors have been FDA-approved for treating refractory hypertension since 1981. Since then, clinical investigations support the benefits of ACE inhibition (ACE-I) in pathologies like congestive heart failure, myocardial infarction, diabetes mellitus, chronic renal insufficiency, and atherosclerotic cardiovascular disease. Both, clinical trials and animal models of type I and type II diabetes have shown that hyperactivity of the angiotensin II signaling pathway contributes to the development of diabetes and its complications, and that blockade of the renin-angiotensin system prevents new onset diabetes and reduces the risk of diabetic complications. Furthermore, ACE inhibitors are generally well tolerated and have few contraindications. This article describes ACE as a target molecule and gives an overview on the clinical evidence that supports the use of ACE inhibitors in diabetes.
Role of the Renin-Angiotensin System in Diabetes
The Renin-Angiotensin System (RAS) is an important component for the homeostasis of blood flow. 1 The existence of the RAS was recognized more than 100 years ago, after the discovery of renin by Tigerstedt and Bergman. 2 Renin is released from juxtaglomerular cells of the kidney in response to reduced renal perfusion pressure, reduced salt transport to the distal tubule, or increased renal sympathetic tone. 3 The cascade of events that follows renin release is illustrated in Figure 1. The action of renin on its liver-generated substrate, angiotensinogen, generates the inactive decapeptide, angiotensin I (Ang I), which is hydrolyzed by angiotensin-converting enzyme (ACE) to the octapeptide, angiotensin II (Ang II). ACE conversion of Ang I occurs primarily in the lungs, producing changes in Ang II levels that vary in accordance to plasma renin levels. 4 There is growing evidence that local systems in various tissues and organs are capable of generating Ang II including the adrenal gland, brain, heart, kidney, vasculature, adipose, gonads, pancreas, prostate, retina, and liver.2,5–14
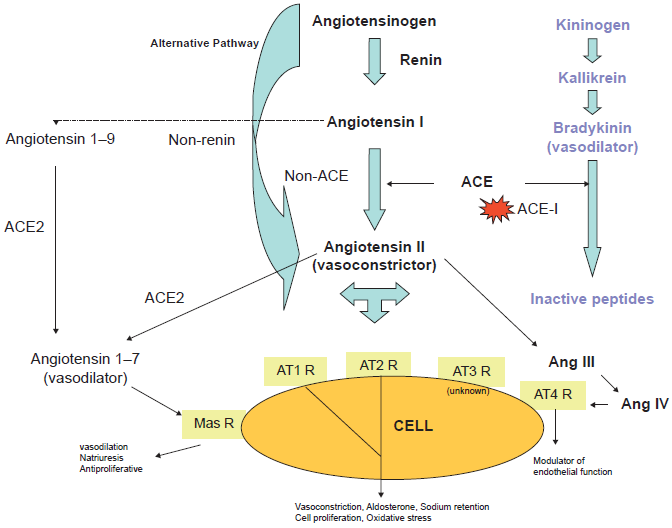
Schematic representation of the Renin-Angiotensin and Kinin-Kallikrein cascade.
Elements of the RAS act in concert to maintain exquisite balance of water homeostasis (Fig. 2). Deregulation or accumulation of any of these elements disrupts the balance, tilting the balance to one side and exacerbating or accelerating the onset of disease. Of the RAS elements shown in Figure 2, Ang II is perhaps the most biologically active, triggering elevation in blood pressure by direct vasoconstriction, the stimulation of thirst by causing vasopressin release, 15 and the induction of aldosterone production leading to water retention and facilitation of sympathetic activity. 16 Ang II has also been implicated in insulin resistance by inhibiting insulin receptor dependent PI3K signaling. 15 Additionally, Ang II and can act on the AT1 receptor, thereby decreasing insulin-induced nitric oxide production and at the same time activating NADPH oxidase leading to enhanced production of other reactive oxygen radicals and enhancing inflammation.16,17 That hypertension is a common characteristic of insulin-resistant diabetes, with observed increases in tissue Ang II seen 18 coupled with the inhibition of the vasodilator, nitric oxide, is not surprising. Further, it has been shown that in diabetic patients, therapeutic inhibition of the RAS increased nitric oxide activity in renal endothelium, having a positive influence on renal function, and possibly cardiovascular function as well. 19
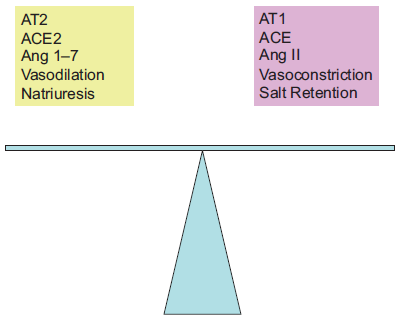
Balance activities in the RAS.
Therapeutic responses to RAS blocking agents indicate that maintenance of normal renin levels may contribute to blood pressure elevation, suggesting that renin-dependent mechanisms may be involved in more than 70% of patients with essential hypertension. On the other hand, 25%-30% of patients have evidence of low or suppressed renin levels, a finding that may reflect primary aldosteronism, sodium or volume excess. 17 Low-renin hypertension is more common among older people with hypertension, women, African Americans, patients with chronic renal parenchymal disease and patients with type 2 diabetes. 17 Although such patients often have lesser blood pressure-lowering benefit from RAS blocking agents, there is evidence that the circulating levels of plasma renin activity (PRA) might not reflect tissue activities of the system. One particular example is the involvement of intrarenal Ang II in progression of renal damage and therefore substantial benefit of RAS blockage despite low circulating levels of renin and Ang II. 17
The frequent association of diabetes mellitus with hypertension, retinopathy, nephropathy, and cardiovascular disease has implicated dysfunction of RAS in the initiation and progression of these disorders.2,18 Because the prevalence of diabetes is reaching epidemic levels, the potential importance of these agents in the prevention and control of diabetic complications is obvious.
Clinical trials have demonstrated the ability of RAS blockade to prevent new-onset diabetes and the development of diabetic complications.19–21 In the Heart Outcomes Prevention Evaluation study (HOPE), diabetes incidence was lower in the group treated with ramipril when compared with placebo. 20 In the Losartan Intervention For Endpoint Reduction in Hypertension study (LIFE), the use of losartan was associated with a reduction in the occurrence of new diabetes onset as compared with atenolol. 22 RAS components, mostly Ang II, have a potential role in endothelial cell dysfunction, insulin resistance, inflammation, and proliferative effects.23–25 Meta analysis of several trials demonstrated that ACE inhibitors or Ang II receptor blockers (ARB) reduce the risk of diabetes by 25%. 26 Clinical evidence supports the idea that aggressive ACE-I treatment is warranted in diabetic patients. A subgroup of the United Kingdom Prospective Diabetes Study (UKPDS) was analyzed for the effect of aggressive versus less aggressive treatment of hypertensive diabetic patients with the ACE-I, captopril, or the beta-blocker, atenolol. This study found that patients treated more aggressively with either antihypertensive agent had reduced risk of complications associated with diabetes when compared to those treated less aggressively.27,28
Targeting RAS
The Angiotensin-Converting Enzyme (ACE)
ACE is a zinc metallopeptidase expressed at the surface of many cells where it catalyzes the conversion of Ang I to Ang II and degrades bradykinin. Bradykinin is a potent vasodilator, acting through the release of prostacyclin, nitric oxide, and endothelial derived hyperpolarization factor (Fig. 1). Clinical and experimental evidence show that blockage of ACE improves endothelial dysfunction. 15
ACE inhibitors (ACE-I) are a family of drugs commonly prescribed to combat hypertension. The primary vasodilatory action of ACE-I is the blockage of ACE and thus the formation of Ang II. With long-term administration, ACE-I lower blood pressure, even in patients with low renin hypertension, suggesting that part of the effect is independent of a decrease in Ang II. 1 The contribution of bradykinin to the action of ACE-I has been debated. 1 Studies by Gainer et al 29 found that co-administration of the bradykinin receptor antagonist, icatibant acetate, significantly attenuated the hypotensive effect of the ACE-I captopril in normotensive and hypertensive subjects. Furthermore, Horning et al, showed that ACE-I increase flow-dependent, endothelial-mediated dilation in humans by bradykinin-dependent mechanisms. 30 In another study, bradykinin concentration in plasma was found to be increased or unchanged after ACE inhibition. 1 These studies suggest a potential contribution of bradykinin to the effect of ACE-I. Considering that the treatment with ACE-I also increases Angiotensin 1-7 levels,31,32 the beneficial action of ACE-I could also be in part due to Angiotensin 1-7 effects.33,34
Currently, there are at least 10 ACE-I that have been approved for use in the US (Table 1 and Fig. 3). 35 Most of these drugs, with the exception of captopril and enalaprilat, are considered to be pro-drugs. The use of ACE-I has risen over the years, with the sales in the U.S. for angiotensin-II antagonists increasing from $3.5 billion (US) in 2003, to $6.6 billion (US) in 2007, while global sales were $19.4 billion (US) in 2007. 36
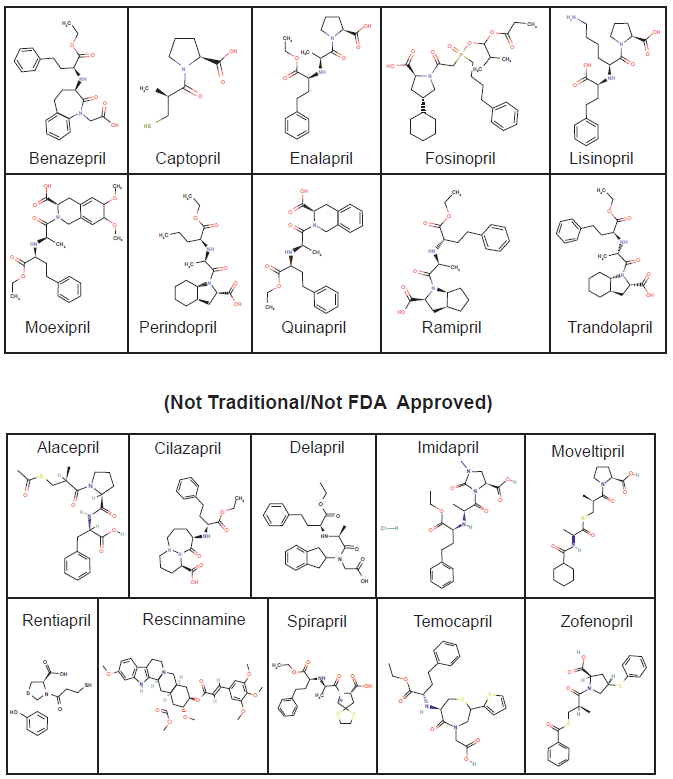
ACE inhibitor Chemical Structures (FDA Approved).
Angiotensin Receptor Blockers (ARBs)
ARBs bind to the angiotensin type-1 receptors (ATR1) (Fig. 1) and block the physiological effects that result from binding of Ang II to these receptors. Similar to ACE-I, these agents reduce blood pressure, inflammation, cytokine generation, and prothrombotic factors. 37 Available ARBs include Candesartan, Eprosartan, Irbesartan, Losartan, Olmesartan, Telmisartan and Valsartan.
Renin blockers
Aliskiren inhibits the capacity of renin to form Ang I, and therefore Ang II (Fig. 1). It produces more complete RAS inhibition than the ACE-I or ARBs. Six randomized, double blinded placebo-control trials in >2,700 patients with mild to moderate hypertension demonstrated the blood lowering potential of this agent. 37 Further trials are under way to assess cardiovascular events and diabetic complications with aliskiren.
ACE-I Blockage and Diabetic Complications
In addition to their antihypertensive properties, for which these compounds were originally designed, ACE-I are also indicated (and prescribed) in a number of clinical situations (Table 1).38–46 There is strong evidence that ACE-I are effective in preventing cardiovascular disease and reducing morbidity and mortality in patients at high risk of cardiovascular disease or renal complications.47–52 Evidence is also mounting for other potential uses for these drugs.
ACE inhibitors.
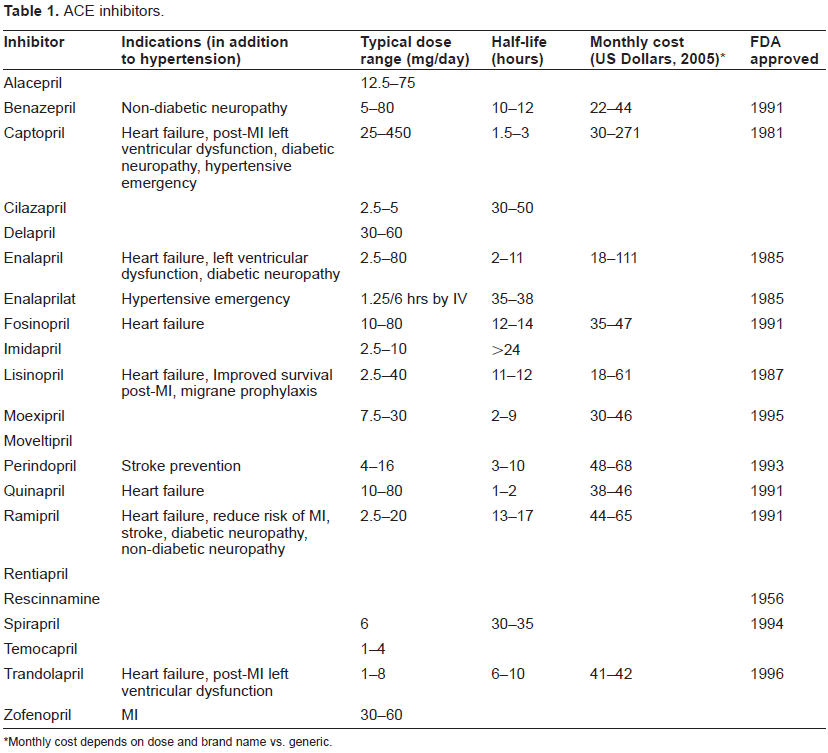
Monthly cost depends on dose and brand name vs. generic.
Hypertension and cardiovascular diseases
Insulin resistance is related to hypertension and frequently is a comorbidity. 53 Patients with diabetes are more likely to be hypertensive than nondiabetics, and hypertension is linked with cardiovascular disease, stroke, progression of renal disease, and other complications. 37 The cardiovascular morbidity and mortality related to diabetes are very high. 15 Clinical trials including the UKPDS, HOPE and MICRO-HOPE, Patients with Type 2 Diabetes and Microalbuminuria Study (IRMA2), and Reduction of Endpoints in Non-insulin-Dependent Diabetes Mellitus with the Angiotensin II Antagonist Losartan (RENAAL) have shown that prevention or reduction of proteinuria, blood pressure control, glycemic control, and particularly the blockade of RAS, are essential to prevent or delay the vascular diabetes complications in diabetics. 15
Studies comparing the effect of ACE-I to other antihypertensive agents have been performed. The Captopril Prevention Project (CAPP) assessed diabetic patients at risk for cardiovascular disease, and found that patients who were treated with captopril had a significantly reduced incidence of cardiac events, and the incidence of diabetes was lower in the captopril treated group compared to those treated with other agents. 54 When compared to diuretics and beta-blocker therapies, patients receiving ARB or ACE-I had a 25%-30% lower risk of developing new-onset diabetes despite similar reduction in blood pressure.55,56
Other studies have also shown that calcium antagonists (another antihypertensive drug class) are less effective than ACE-I in preventing cardiovascular events in diabetic hypertensive patients. 57 The Appropriate Blood Pressure Control in Diabetes Trial also found that diabetic patients treated with ACE-I had lower incidence of MI and overall cardiac events compared to patients treated with a calcium antagonist. 28 However, recent large prospective randomized studies showed an opposite effect. 57
Diuretics, the gold standard treatment in hypertension have been used singly and in combination with ACE-I. However, they have been shown to actually impair glucose tolerance and thereby accelerate the development of diabetes mellitus.58,59 The effect of treating diabetics with thiazide diuretics may be detrimental to their health by affecting the action of insulin. 58 Thiazide diuretics were also associated with increased cardiovascular mortality in diabetic patients except at low-medium dose. 57 When given in combination with ACE-I, it was shown that ACE-I alone provided better health benefit than when combined with thiazide diuretics. In the CAPP study, captopril reduced the relative risk of diabetes by 22% in previously untreated patients compared with diuretic and/or beta-blocker treatment. 54
The combination of ACE-I and ARB is controversial. Some experts believe there are advantages to the combination to further reduce blood pressure. 60 According to The Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET), combination therapy of ACE-I and ARB showed a modest effect of lowering blood pressure in diabetic patients, but the added risk of adverse events attributable to the combination therapy makes them not recommendable in the treatment of hypertension. 61 However, it was suggested that the ACE-I and ARB combination therapy maybe beneficial to patients having proteinuria or diabetic patients without concomitant diseases. 61 There also appears to be a substantial benefit in heart failure and renal disease.62,63 In the Candesartan and Lisinopril Microalbuminuria (CALM) study in hypertensive patients with type 2 diabetes and microalbuminuria, the combination was more effective in reducing blood pressure and the urinary albumin:creatinine ratio than either agent alone. 64 The combination of an ACE inhibitor and an ARB produced no significant clinical benefit in preventing vascular events in high-risk patients in ONTARGET. But, the risk of adverse events, including hypotension, syncope, renal dysfunction, and hyperkalemia, was increased with combination therapy.
The American Diabetes Association (ADA) recommends that all patients with diabetes and hypertension receive an ACE-I or ARB as part of their antihypertensive regime. 65 ACE-I is a strong first-line therapy for diabetic patients having hypertension, but it is recognized that hypertension may best be combated by multi-therapy.66,67
Renal complications
The relative risk of developing end-stage renal disease increases with higher systolic blood pressure.68,69 Ang II produces renal vasoconstriction and antinatriuresis, therefore, targeting the RAS is a logical approach to reducing renovascular risk. 37 National guidelines recommend ACE-I or ARB therapy in patients with diabetes who also have hypertensionand/orproteinuriatoretardtheprogressionof renal damage.65,70,71 One of the main characteristics of essential hypertension is nephrosclerosis, the first clinical sign of which is protein in the urine. Proteinuria is the main predictor of cardiovascular disease in patients with type 2 diabetes as well as progressive renal disease in type 1 diabetes and in patients with overt diabetic nephropathy. 1 Renoprotective effects of captopril are reported in diabetic neuropathy, 72 the ACE-I ramipril, exhibited vascular and renal protective effects in high risk diabetic patients with previous history of cardiovascular events, 73 and the ACE-I, benazepril was shown to inhibit the deterioration of renal function in patients with glomerular disease.1,74 Treatment with ACE-I has been shown to consistently reduce proteinuria in these patients, as compared to other antihypertensive agents.75,76
Other complications
ACE-I therapy is now commonly prescribed to diabetic patients and has been associated with a lower likelihood of other complications including a history of cancer and peptic ulcers. 77 Also, clinical studies have detected inhibition of diabetic retinopathy by ACE-I. The EURODIAB Control Trial of Lisinopril in Insulin-Dependent Diabetes Study Group investigated the effect of the ACE-I, lisinopril, on retinopathy in normotensive type I diabetic patients. They found a 50% reduction in the progression of retinopathy in lisinopril treated subjects compared to controls. 78 After 9 years follow-up, the UKPDS clinical trial similarly reported that the ACE-I captopril inhibited the two-step progression of retinopathy by 34%. 78 Despite the evidence that the use of ACE-I does not have long-term or irreversible effects in most cases, there is literature stating that ACE-I are still underprescribed.79,80 A recent study using 30,750 patients with diabetes (68.7% with hypertension and/or proteinuria) suggested a potential underuse of ACE-I and ARB in elderly patients with diabetes. Of the whole sample, only 50.7% of potential users were administered an ACE-I or ARB in the quarter studied. In multivariate analysis, failure to administer either agent was associated significantly with older age, male sex, chronic lung disease, depression, dementia and other mental illness. 70
Generally, this family of drugs has the effect of increasing plasma levels of renin, and decreasing aldosterone secretion. The effects of a single dose treatment with ACE-I, such as ramipril have been shown to be long-lasting, maintaining up to 80% inhibition 24 hours after administration.81,82 They are additionally thought to have effects separate from the ACE effects, as they have been shown to also increase kinins and N-acetyl-seryl-aspartyl-lysyl-proline, a tetrapeptide that has anti-fibrotic and anti-inflammatory effects.83,84
Overall, ACE-I are effective as antihypertensive agents, have utility in prevention of cardiac remodeling following myocardial infarct (MI), inhibition of heart and kidney disease, prevention of cancer and diabetes, and their use has even been associated with decreased mortality in patients hospitalized with community-acquired pneumonia.50,51,58,77,80,83,85–93
ACE-I Side Effects and Limitations
ACE inhibitors are generally well tolerated and have few contraindications. 94 However, the use of ACE-I does come with side effects and warnings. The most common side effects in adults are a dry, persistent cough attributed to accumulation of substance P (which is normally degraded by kininase II), 17 dizziness, fatigue and nausea. Other side effects include hypotension, hyperkalemia, hypoglycemia, renal failure and angioedema. 44 ACE inhibitors are not nephrotoxic, but an increase of up to 20 percent in the serum creatinine level is not uncommon. During the first four weeks of treatment, serum potassium and creatinine levels should be monitored closely. 95 Hypotension can occur in patients with hyponatremia or volume depletion, those taking vasodilators, those in acute heart failure or dialysis. Patients with high plasma renin level are vulnerable to first dose hypotension. 95 Cough occurs in 5-20 percent of patients, more frequently in women than men, and more frequent in blacks than whites. It develops within one week to six months and resolves within four days of cessation. 95 Hyperkalemia generally occurs in patients with renal insufficiency or diabetes. Patients taking potassium, salt substitutes, potassium-sparing diuretics, beta blockers, and NSAIDs are susceptible. 95
It has been shown that black people received less benefit from ACE-I than do white people. 71 Also, other RAS blockers like the ARBs are generally better tolerated than ACE-I across large populations, particularly in black people, cigarette smokers, and people who might be susceptible to the effects of bradykinin. 96 There is some evidence that with longterm ACE-I treatment, circulating Ang II levels may return to pretreatment levels, perhaps through activation of the so-called alternative pathway (Fig. 1), although the studies are controversial.17,37
The absolute contraindications for ACE-I are: 1) angioneurotic edema which occurs in approximately 0.1-0.2 percent patients, 2) ACE-I must be avoided by pregnant women, as major congenital malformations have been seen in fetus exposed to ACE-I following the first trimester,97–100 3) renal artery stenosis and 4) previous allergy to ACE inhibitors.
Conclusions
The RAS is involved in a wide range of adverse effects that contribute to metabolic diseases. ACE-I are effective as antihypertensive agents, have utility in prevention of cardiac remodeling following myocardial infarct (MI), inhibition of heart and kidney disease, prevention of diabetes, and their use has even been associated with decreased mortality in patients hospitalized with community-acquired pneumonia. Furthermore, evidence is starting to accumulate for further beneficial uses of these drugs in diabetic patients. In spite of the accumulating evidence on the benefits of ACE-I therapy, there is an underuse of ACE-I in patients with diabetes.80,101
Disclosures
The authors report no conflicts of interest.