
Abstract
Oral mucositis (OM) is one of the most debilitating and common side effects of intensive anti-cancer treatment. OM is associated with adverse clinical and economic outcomes. In addition to its symptomatic impact, OM increases the likelihood of unplanned breaks or delays in anti-cancer treatment, reduction in dose of chemotherapy, use of feeding tube placement or total parenteral nutrition, the need for an intravenous line, opioid use and hospitalization. Palifermin is a N-truncated recombinant human keratinocyte growth factor (KGF), a member of the fibroblast growth factor (FGF) family, which binds specifically to the human KGF receptor and induces proliferation and differentiation of epithelial cells, including gastrointestinal epithelial cells, hepatocytes, type II pneumocytes, and transitional urothelial cells. It is the first agent approved by the U.S Food and Drug Administration and other regulatory authorities around the world for use in the prevention of oral mucositis caused by high-dose chemotherapy and stem cell transplantation. The following review aims to cover the recent peer-reviewed literature pertaining to the role of palifermin in the prevention of OM in different groups of patients treated with radiation therapy or chemotherapy against cancers.
Introduction
Oral mucositis [OM] is a frequent complication of the chemotherapy and radiotherapy regimens commonly used in oncological practice. It is an especially severe problem for patients who are undergoing hematopoietic stem-cell transplantation [HSCT] because of high-dose, myeloablative chemotherapy or radiotherapy, including total body irradiation [TBI], used for conditioning. In the HSCT setting OM may occur in up to 100% of patients. It results from the direct toxic effect of therapy on mucosa cells, but the mechanisms of mucositis seem to be more complex. 1 Many patients need nutritional support with total parenteral nutrition if oral intake is impossible. OM is usually managed by the application of topical and systemic pain medications. Many patients require narcotic pain medication and the length of time of intravenous narcotic need is one of the best indicators of the degree of mucositis. Morphine was recommended as the opioid of choice for patient controlled analgesia. 2 Bolwell et al investigated factors influencing mucositis after autologous progenitor cell transplantation. They treated patients suffering from non-Hodgkin's lymphoma [NHL], multiple myeloma and Hodgkin's disease. Patients were mobilized with G-CSF alone or the combination of etoposide and G-CSF. Univariable correlates of worse mucositis were prior radiation therapy, diagnosis of NHL, progenitor cell mobilizing regimen containing etoposide and HSCT regimen containing etoposide. Multivariable regression analysis revealed that NHL diagnosis, prior radiation therapy and etoposide in the mobilizing regimen were associated with worse post-transplant mucositis. 3 From the patients point of view, oral mucositis is often a debilitating complication of a transplant. 4 OM is associated with an increased risk of systemic infection resulting from bacteremia associated with the breakdown of mucosal barriers. The severity of mucositis and the associated infection risk is a significant cause of morbidity and mortality. 5 The recent data suggest that the inflammatory response after conditioning for HSCT is the result of the chemotherapy-induced mucositis and independent of neutropenia. Though primary inflammation appeared due to mucositis, infections resulting from mucosal barrier injury and neutropenia aggravated the inflammatory response. Hence, at least for some HSCT recipients, the inflammatory response and fever are the direct consequence of mucositis alone, and neutropenia plays a minor role or none at all.
The magnitude of the inflammatory response can, however, be aggravated by intercurrent infections arising from the loss of the mucosal barrier and simultaneous neutropenia. Consequently, the term febrile neutropenia might be better replaced by the term febrile mucositis. 6 Radiation therapy [RT] is commonly used to treat cancers. The incidence of mucositis among patients receiving RT varies depending on tumor location, radiation dose, schedule and use of concomitant chemotherapy. Oral mucositis is among the most frequent, symptomatic and regimen-limiting toxicities in patients suffering from head and neck cancers treated with RT and radiosensitizing concomitant chemo-therapy. 7 While oral mucosa can be easily inspected, we know little about small intestinal mucositis. Triantafyllou and Tsirigotis evaluated the severity of this early transplant-related complication using a video-capsule endoscopy. Their studies reveal for the first time that small intestinal mucositis in patients undergoing conditioning therapy for peripheral blood stem cell transplantations presents as small intestinal ulcerations. Severe intestinal mucositis was significantly associated with a higher incidence of documented infections.8,9 Whether intestinal barrier preservation [palifermin] protects from invasive infections, and in the allogeneic setting diminishes GVHD severity, remains to be investigated in randomized controlled trials. 10
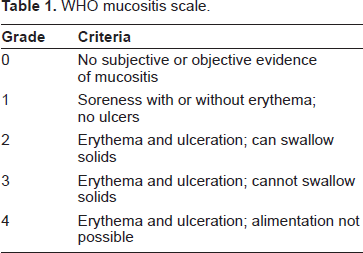
A number of scoring systems are available to grade the severity of oral mucositis, although none is universally accepted (Tables 1, 2, 3). Most scoring systems incorporate both subjective (e.g. pain) and objective (e.g. number and extent of ulcers) criteria to arrive at a final score.11–13 The National Cancer Institute Common Toxicity Criteria grading combines oral mucositis grade with grades of diarrhea, abdominal pain, nausea and use of narcotic analgesics representing a global index of mucositis. 14 The WHO scale, commonly used in clinical practice, 15 rates mucositis from 0 to 4 depending on the presence of oropharyngeal erythema and ulcers and the ability to tolerate solids and liquids. 11 WHO grades 3 and 4 mucositis are considered severe and are usually characterized by pain that requires intravenous narcotics. Patients with WHO grades 0 to 2 oral mucositis often require minimal or no intravenous narcotics and generally do not require extensive nutritional support. The negative impact of mucositis on patient outcomes has led to numerous attempts to decrease its incidence and severity in patients receiving radiotherapy or chemotherapy. Although methods such as cryotherapy, sucralfate, amifostine, granulocyte colony-stimulating factor, and granulocyte-macrophage colony-stimulating factor have been evaluated for a possible role in ameliorating mucositis, palifermin [Kepivance; Amgen Manufacturing Ltd, Thousand Oaks, CA], a recombinant human keratinocyte growth factor [rHuKGF], is the first drug to consistently demonstrate a benefit in clinical trials. 16
WHO mucositis scale.
Common terminology criteria for adverse events v3.0 (CTCAE).
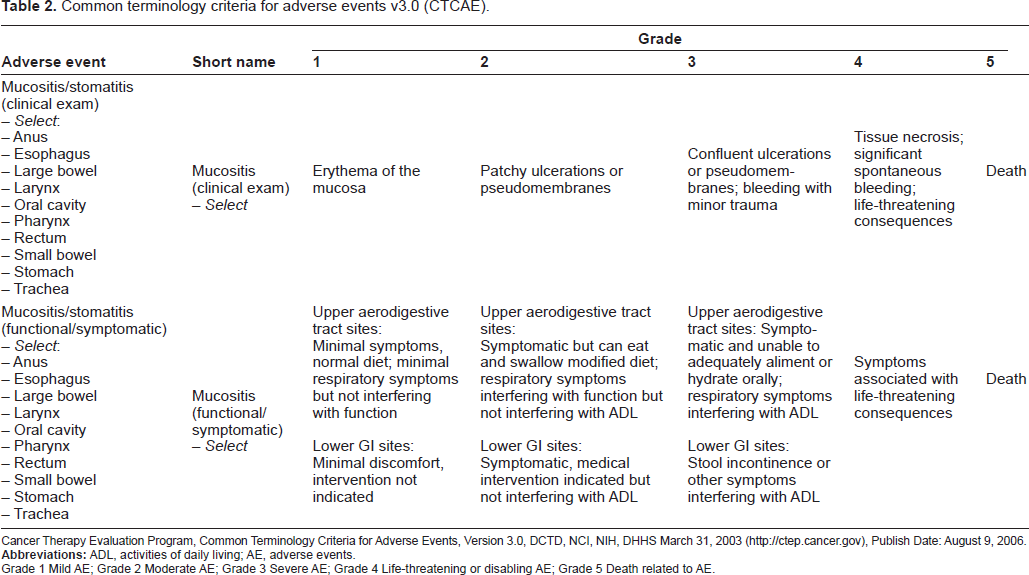
Cancer Therapy Evaluation Program, Common Terminology Criteria for Adverse Events, Version 3.0, DCTD, NCI, NIH, DHHS March 31, 2003 (http://ctep.cancer.gov), Publish Date: August 9, 2006.
Grade 1 Mild AE; Grade 2 Moderate AE; Grade 3 Severe AE; Grade 4 Life-threatening or disabling AE; Grade 5 Death related to AE.
OMAS mucositis scale.
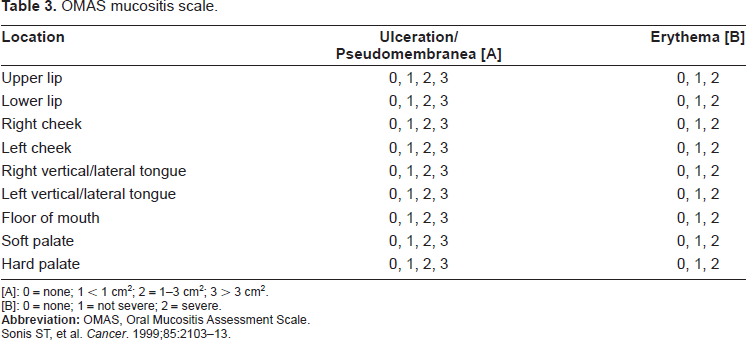
[A]: 0 = none; 1 < 1 cm2; 2 = 1-3 cm2; 3 > 3 cm2.
[B]: 0 = none; 1 = not severe; 2 = severe.
Sonis ST, et al. Cancer. 1999;85:2103-13.
Mechanism of Action
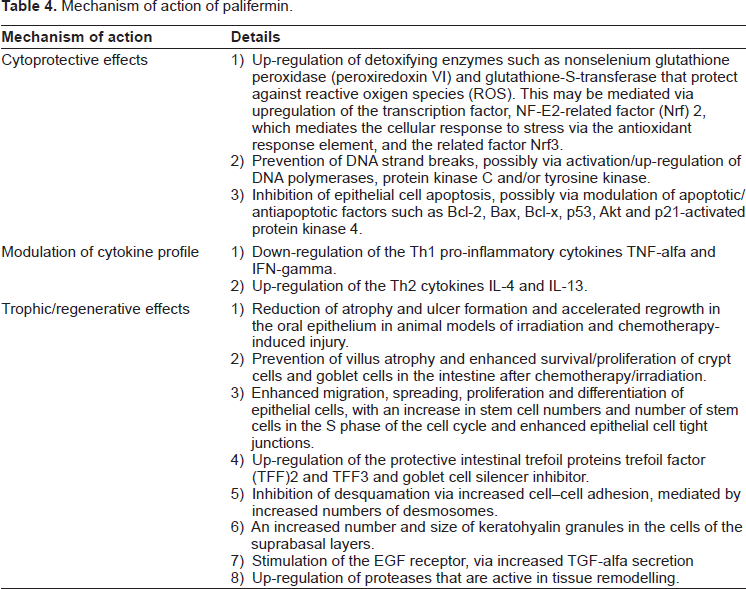
Palifermin is a humanized form of keratinocyte growth factor [KGF] that is produced by Escherichia coli through recombinant DNA technology. With a molecular weight of 16.3 kDa, it is smaller than endogenous KGF because it has been rendered more stable by removal of the first 23 N-terminal amino acids. Palifermin binds specifically to a tyrosine kinase receptor fibroblast growth factor receptor-2b [FGFR2b], which is uniquely expressed in epithelial cells in a variety of tissues. It has a number of biological effects (Table 4), which together limit cellular damage.17–19
Mechanism of action of palifermin.
Pharmacokinetics
The pharmacokinetics of palifermin were studied in healthy subjects and patients with hematologic malignancies. After single IV doses of 20 to 250 mcg/kg (healthy subjects) and 60 mcg/kg (cancer patients), Palifermin concentrations declined rapidly (over 95% decrease) in the first 30 minutes post-dose. A slight increase or plateau in concentration occurred at approximately 1 to 4 hours, followed by a terminal decline phase. Palifermin exhibited linear pharmacokinetics with extravascular distribution. On average, total body clearance (CL) appeared to be 2- to 4-fold higher, and volume of distribution at steady state (Vss) to be 2-fold higher in cancer patients compared with healthy subjects after a 60 mcg/kg single dose of Palifermin. The elimination half-life was similar between healthy subjects and cancer patients (average 4.5 hours with a range of 3.3 to 5.7 hours). No accumulation of Palifermin occurred after 3 consecutive daily doses of 20 and 40 mcg/kg in healthy volunteers or 60 mcg/kg in cancer patients. 20
Pharmacodynamics
Epithelial cell proliferation was assessed by Ki67 immunohistochemical staining in healthy subjects. A 3-fold or greater increase in Ki67 staining was observed in buccal biopsies from 3 of 6 healthy subjects given Palifermin at 40 mcg/kg/day IV for 3 days, when measured 24 hours after the third dose. Dose-dependent epithelial cell proliferation was observed in healthy subjects given single IV doses of 120 to 250 mcg/kg 48 hours post-dosing. 20
Indications and Dosing
Palifermin is indicated to decrease the frequency and duration of severe oral mucositis in patients with hematologic malignancies who are to receive myelotoxic therapy and require hematopoietic stem cell support.20,21 The recommended dosage of palifermin is 60 mcg/kg/day, administered as an IV bolus injection for 3 consecutive days before and 3 consecutive days after myelotoxic therapy for a total of 6 doses. Pre-myelotoxic therapy: The first 3 doses should be administered prior to myelotoxic therapy, with the third dose 24 to 48 hours before myelotoxic therapy. Post-myelotoxic therapy: The last 3 doses should be administered post-myelotoxic therapy, the first of these doses should be administered after, but on the same day of hematopoietic stem cell infusion and at least 4 days after the most recent administration of palifermin. We know little about modification of palifermin dosage in different myeloablative therapies. Future studies are needed to resolve this problem. 22 From a clinical point of view, administration of a single collapsed dose of palifermin once before and once more after myeloablative therapy is more convenient than the standard regimen. Zia-Amirhosseini, et al, assessed the pharmacokinetic profile of palifermin after intravenous dosing with either a collapsed dose of 180 mcg/kg/day for 1 day or a standard dose of 60 mcg/kg/day for 3 days, before and after myeloablative chemo-radiotherapy and peripheral blood progenitor cell transplantation. Both dosing regimens were well tolerated. Their results were consistent with approximately dose-linear pharmacokinetics for the two dosing regimens, with no observed accumulation. 23 A randomized, controlled study is warranted to assess the safety and efficacy of collapsed-dose palifermin, which may provide a more convenient administration schedule.24,25 Guidelines for palifermin dosing in patients with renal dysfunction are not available. However, the results of a recent study in 31 patients suggest that the pharmacokinetics of palifermin are not affected by renal function. 26
Clinical Studies
A multicenter double-blind, placebo-controlled, randomized study was conducted to evaluate the efficacy of palifermin to reduce the incidence of WHO grades 3 and 4 mucositis in patients with hematologic malignancies undergoing auto-HSCT with a total body irradiation-containing conditioning regimen. The conditioning regimen consisted of TBI (12 Gy administered in 6, 8, or 10 fractions), etoposide 60 mg/kg on the day after completing TBI, and cyclophosphamide 100 mg/kg 2 days after etoposide. Peripheral blood progenitor cells were infused 2 days after cyclophosphamide. Palifermin 60 mcg/kg or placebo was administered daily for the 3 days preceding TBI and for 3 days beginning on the day of stem-cell infusion. 212 patients who received at least one dose of palifermin (106 patients) or placebo (106 patients) were evaluated for efficacy and safety. Patients with non-Hodgkin's lymphoma (NHL) and Hodgkin's lymphoma comprised 87% of the patients. WHO grade 3 or 4 oral mucositis developed in 63% of the palifermin-treated patients and 98% of the placebo-treated patients (P < 0.001). Among patients who developed grade 3 or 4 oral mucositis, its median duration was 3 days in the palifermin group and 9 days in the placebo group (P < 0.001). Palifermin was also effective for reducing the incidence of grade 4 oral mucositis (20% vs. 62%; P < 0.001) and its duration (2 days vs. 6 days; P = 0.004). Patient-reported mouth and throat soreness was significantly lower in the palifermin-treated patients (P < 0.001), and palifermin was also associated with improved swallowing, drinking, eating, talking, and sleeping (P < 0.001 for all). On the basis of this study palifermin was approved for the reduction of mucositis following HSCT. 21 Elting et al, estimated the impact of palifermin prophylaxis on hospital costs of transplantation in Spielberger's trial. This was a retrospective, economic analysis of estimated costs for a previously published clinical trial. 21 Patients from Spilelberger's study completed a daily questionnaire (Oral Mucositis Daily Questionnaire-OMDQ) evaluating mouth and throat soreness (MTS) severity and its impact on daily functional activities. Patients, self-assessment data were compared with clinicians, assessments of oral mucositis using the objective scales. Patients receiving palifermin reported statistically significant improvements in daily functioning activities (swallowing, drinking, eating, talking and sleeping) and required significantly less narcotic opioids. Improvement in the patient's overall physical and functional well-being was also reported. Comparisons between patient and clinician assessments demonstrated that the average daily scores between mucositis grade and subjective (MTS) instruments were similar. These results support the clinical benefit of palifermin in the autologous HSCT setting. 27 Costs were not collected during this trial. The authors found, that in addition to its previously demonstrated clinical benefit, palifermin prophylaxis offers a favorable economic profile among patients with hematologic malignancies who receive TBI and autologous stem cell support. It was caused by reductions in adverse outcomes and their associated hospital stay (incidence of febrile neutropenia, bacteremia/fungemia, pneumonia or use of total parenteral nutrition) in palifermin group in spite of the high price of the drug. 28 Two non-randomized studies from Australia estimated the efficacy of palifermin in autologous HSCT setting without TBI. The conditioning regimens were: busulphan containing (Bu/CTX, Bu/CTX/etoposide) or high dose melphalan (200 mg/m2 or BEAM, R-BEAM). There was a significant reduction in the incidence of severe oral mucositis and swallowing problems. There was no significant difference in infection, dietary intake, time to engraftment or cumulative dose and duration of narcotic administration between groups (receiving or not receiving palifermin).29,30 In allogeneic HSCT setting the randomized, double-blind, placebo-controlled, dose-escalation study assessed the safety and tolerability of palifermin. Patients with hematological malignancies and myelodysplastic syndromes were conditioned with cyclophosphamide and fractionated total body irradiation (CTX/TBI) or busulphan and cyclophosphamide (Bu/CTX) and given methotrexate along with a calcineurin inhibitor (cyclosporine A, tacrolimus) for graft versus host disease (GVHD) prophylaxis. Patients had a 6 of 6 human leukocyte antigen-matched sibling donor. Investigators found, that palifermin was generally safe in allogeneic HSCTs but had no significant effect on engraftment, the incidence and severity of acute GVHD, or survival in this trial. Similar to its effects in patients receiving autologous HSCT, palifermin was associated with a reduced incidence and severity of oral mucositis in patients receiving a more substantial mucotoxic regimen of high dose chemotherapy with TBI/CTX but not the less mucotoxic regimen – Bu/CTX. 31 The results of the long follow up phase of the trial of Blazar et al 2006 are now avail-able. 32 The investigators found no differences in CMV or invasive fungal infections, chronic GVHD, or long-term survival between cohorts. They concluded that the benefits of palifermin appear primarily to be limited to ameliorating mucotoxicity when given to allogeneic HCT recipients.
Adverse events occurring with ≥5% higher incidence in palifermin vs. placebo.
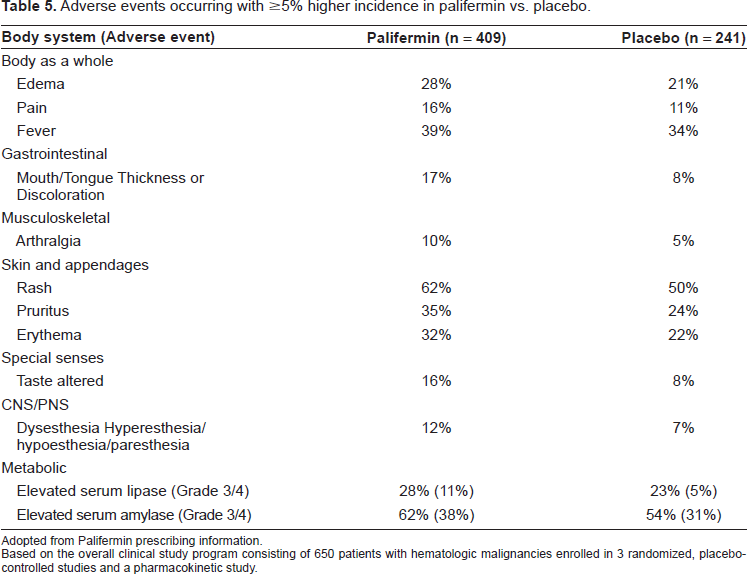
Adopted from Palifermin prescribing information.
Based on the overall clinical study program consisting of 650 patients with hematologic malignancies enrolled in 3 randomized, placebo-controlled studies and a pharmacokinetic study.
In two Polish studies (single and multicenter) investigators assessed the ability of palifermin to reduce the incidence, duration and severity of oral mucositis (OM) induced by high-dose chemo-/radiotherapy followed by HSCT in patients with hematological diseases. Both types of transplantations: autologous and allogeneic were evaluated. The requirement for analgesics and total parenteral nutrition (TPN) administered because of OM, incidence of febrile neutropenia and severe infections were also evaluated. The influence of palifermin on hematopoietic recovery, on the incidence of acute GvHD (aGvHD) and on the length of hospitalization after HSCT was assessed. The studies were planned as a single arm trial with a retrospective group of control patients selected by each center (in case of multicenter study). Each of the reporting centers submitted an equal number of patients to the palifermin and control groups. The data were collected and analyzed by the principal investigator. There was a significant reduction in the incidence of OM of World Health Organization (WHO) grades 1-4; 3-4 and the median duration of OM in the palifermin group compared to the control patients. The incidence of analgesics, opioid analgesics and TPN was also significantly reduced. The analysis of distribution of affected organs revealed that aGvHD was less prevalent in the palifermin group. There was no significant difference in the onset of any OM after HSCT, time to engraftment and length of hospitalization between groups also there was no significant difference in the incidence of febrile neutropenia and severe infections, the time to engraftment and length of hospitalization between groups in both types of transplants.1,33 In single center study the trend to reduce the number of days with antibiotics treatment and shorten time to platelet engraftment for allogeneic patients was also observed. 33
In a multicenter Austrian study 30 patients undergoing matched related or unrelated allogeneic stem-cell transplantation for leukemia were treated with palifermin and retrospectively compared to a matched control group. The results were similar to previously described studies. The administration of palifermin significantly reduced oral mucositis whereas, regardless of donor status, no effect on the incidence and severity of acute graft versus host disease was seen. Unfortunately, reduction of severity, incidence and duration of oral mucositis WHO grades 2-4 was mainly observed in palifermin recipients transplanted with a matched-unrelated donors. 34 The small phase I/II randomized multicenter trial examined palifermin in the setting of solid tumors. In this study, Rosen et al. randomly assigned 64 patients with metastatic colorectal cancer receiving fluorouracil/leucovorin to palifermin or placebo, given for 3 consecutive days before each of two consecutive chemotherapy cycles. They reported a lower incidence of grade 2 or worse oral mucositis in patients who received palifermin, compared with placebo (29% vs. 61% in cycle 1; 11% vs. 47% in cycle 2). There were no statistically significant differences in the incidence or severity of diarrhea or in overall survival between the groups. 35
Safety and Tolerability
Palifermin appears to be well tolerated at the dosages studied. Adverse events are generally consistent with the biological activities of this growth factor on skin and oral epithelium, generally mild to moderate in severity and reversible. In the phase III study, rash, pruritus, erythema, cough and edema were most common events reported by palifermin recipients, occuring in 55%, 50%, 44%, 32% and 27% of patients, respectively. However, these events were also relatively common in the placebo group, with corresponding incidences of 46%, 32%, 30%, 26% and 17%, respectively. All events were transient and mild to moderate and none led to discontinuation of palifermin treatment. Anti-palifermin antibodies were not detected. Adverse events occurring more frequently in palifermin-treated patients as compared to placebo-treated patients (a higher incidence of 5%) are listed in Table 5. The median time to onset of cutaneous toxicity was 6 days following the first of 3 consecutive daily doses of palifermin, with a median duration of 5 days. An interval of no less than 4 days must separate the last pre-dose (dose 3) and the first post-dose (dose 4) of palifermin because of the potential for increased skin and oral related adverse events when the cumulative dose exceeds 360 mcg/kg within 7 or 8 days. Palifermin should not be administered within 24 hours before or during infusion of cytotoxic chemotherapy. In clinical trial, administration of palifermin within 24 hours of chemotherapy resulted in an increased severity and duration of oral mucositis.20,21
Acanthosis nigricans, described with insulin resistance and with gastrointestinal or lung carcinomas, has been recently reported with palifermin use. In this case, an obese 45-year-old woman was treated for multiple myeloma with melphalan 200 mg/m2 followed by autologous stem cell transplantation. She had impaired glucose tolerance on an oral glucose tolerance test. She received palifermin, 60 mcg/kg per day for 3 days before chemotherapy and again for 3 days after stem cell reinfusion. Five days after graft infusion she developed a bilateral hyperpigmented hyperkeratotic axillary rash consistent with acanthosis nigricans. The rash spontaneously resolved over 3 days following completion of palifermin therapy. This pathogenesis is related to increased tyrosine kinase growth factor receptor signaling from transforming growth factor-alfa, insulin-like growth factor-1 or activating mutations of the fibroblast growth factor receptor. 36
A case of severe hand-foot syndrome with toxic epidermolysis has recently been reported. 37 Five patients who developed flexural hyperpigmentation after treatment with palifermin have been recently described. All patients showed ill-defined symmetrical hyperpigmented papillomatous plaques with slight erythema in the skin folds, especially affecting axillary and inguinal areas. The most striking histological finding was the thickened granular layer in all patients. The filaggrin, an essential component in the terminal differentiation of the epidermis, was upregulated in these cases. 38
The safety and efficacy of palifermin have not been established in patients with non-hematologic malignancies. The effects of palifermin on stimulation of KGF receptor-expressing, non-hematopoietic tumors in patients are not known. It has been shown to enhance the growth of human epithelial tumor cell lines in vitro and to increase the rate of tumor cell line growth in a human carcinoma xenograft model. Although KGF promoted proliferation in human endometrial carcinoma cells, via activation of the MAPK pathway, the effect was small. Hematological malignancies do not express the KGF receptor, so palifermin does not possess any adverse effects on their outcome. 19 Current trials investigate the use of palifermin in solid tumor settings. The objective of Brake's study was to determine whether combining palifermin with different chemotherapeutic or biological agents affected the antitumor activity of these agents in human head and neck (FaDu) and colorectal (HT29) carcinoma xenograft models. Nude CD1 mice were injected with 1 × 10(7) of either FaDu or HT29 cells, which express both KGF and epithelial growth factor receptors. Animals were treated with palifermin in various combinations with chemotherapeutic (5-fluorouracil and cisplatin) and/or biological (bevacizumab, cetuximab, and panitumumab) agents. Palifermin alone had no effect on either FaDu or HT29 tumor growth. Palifermin did not affect the therapeutic efficacy of 5-fluorouracil, cisplatin, cetuximab, bevacizumab, or panitumumab in any of the two- or three-way drug combinations tested in either model. The results of this study showed that palifermin did not promote the growth of two carcinoma cell lines that express functional KGF receptors and did not protect these tumor cells from the antitumor effects of several chemotherapeutic and biological agents. 39
Conclusions
Oral and intestinal mucositis are among the most significant dose-limiting toxic effects of intensive cancer treatment and are associated with adverse clinical and economic outcomes. Recombinant human KGF-1 (fibroblast growth factor 7 [FGF-7] or palifermin) is a member of the FGF super class. Initially, the tissue-protective capacity of palifermin was attributed to its mitogenic effect, which results in increased thickness of mucosal epithelium. However, palifermin also upregulates the expression of transcription factor Nrf2 in keratinocytes, which leads to the upregulation of genes that encode a series of reactive oxygen species-scavenging enzymes. It stimulates the generation of the anti-inflammatory cytokine interleukin-13 (IL-13), which reduces tumor necrosis factor, a proinflammatory cytokine that plays a key role in the pathogenesis of mucositis. In addition, palifermin exerts antiapoptotic effects and reduces angiogenesis. Palifermin, an N-truncated recombinant human keratinocyte growth factor-1, is the first agent to be approved for the prevention of oral mucositis. Palifermin reduces the incidence, severity and duration of oral mucositis in patients with hematological malignancies undergoing myelotoxic conditioning therapy and hematopoietic stem-cell transplantation. Clinical sequelae, including febrile neutropenia and resource use (opioid analgesia and parenteral feeding), are concomitantly reduced. Other potential applications being explored include use in the solid tumor setting. The side effects of the treatment are generally mild and transient, and are confined to skin rashes, pruritus, mouth and tongue disorders and altered taste. This led the Food and Drug Administration (FDA) to approve palifermin for the prevention of oral mucositis of patients with hematological malignancies and boosted the development of other mucosa-protective growth factors, such as repifermin (KGF-2) and velafermin (fibroblast growth factor-20).16,19,40 Preclinical studies show that KGF has several other properties besides protecting epithelial surfaces as it lessens apoptosis of several cell types and modulates the inflammatory and immune responses, which could be of benefit in the setting of allogeneic HSCT. Moreover, KGF has been shown to reduce the incidence of acute GVHD (aGVHD) in mouse models and to improve immune reconstitution by thymic preservation. The amelioration of aGVHD has been attributed to the preservation of gut integrity with decreased translocation of microbial products and reduced cytokine production, although other factors probably contribute such as the shift of cytokine profiles from helper T cell Th1 to Th2.16,19,40 KGF administration may offer a novel approach to the separation of graft-versus-leukemia (GVL) effects from GVHD. 41 Palifermin might also be effective as a treatment of severe, refractory hemorrhagic cystitis. 42 Thus, the development of palifermin and other potential new agents for preventing chemotherapy- and radiotherapy-induced mucositis represents an important breakthrough in oncological supportive care.
Disclosure
The authors report no conflicts of interest.