
Abstract
Acute decompensated heart failure (ADHF) is a prominent condition whose frequency is increasing, especially in the context of an aging population. The ability to discern the cause of undifferentiated dyspnea in acute presentations is an increasing struggle. In this review, we seek to explore the various biomarkers that have been studied for the diagnosis of ADHF and their respective clinical utilities as the most recent data would suggest. Natriuretic peptides, galectin-3, soluble ST2, adrenomedullin, cardiac troponin-T, neutrophil gelatinase-associated lipocalin, and copeptin are reviewed. Of these biomarkers, natriuretic peptides are the most thoroughly evaluated and show the most promise for diagnosis or exclusion of acute heart failure, though other biomarkers can add significant utility in the form of prognostication.
Introduction
Clinical congestive heart failure (HF) is a massive and growing epidemic with an expected 25% growth in the next 15 years beyond the current prevalence of 10 per 1000 among patients more than 65 years of age. 1 Despite the prevalence and readily identifiable clinical signs, including peripheral edema, jugular venous distention, pulmonary rales, and an S3 gallop, the diagnosis of acute HF remains elusive in many settings as various comorbidities may contribute to acute respiratory events. Furthermore, conditions that mimic acute decompensated HF (ADHF) have similar risk factors, such as hypertension, diabetes, and tobacco use. As a result of this uncertainty, biomarker research in HF has increased dramatically to assist clinicians adjunctively with the diagnosis of ADHF.
Paramount to the discussion below is the realization that biomarkers can only be used to extend the evaluation and that history and physical exam continue to be the most important tools for the evaluation of HF and undifferentiated dyspnea in acute settings. Isolated elevations of the biomarkers discussed herein are of no inherent consequence and should always be taken in the clinical context.
In this article, we review the current literature and focus on the laboratory biomarkers that have been tested for the diagnosis of ADHF. We also describe the use of some of the biomarkers in the prognosis with respect to both ADHF and serial observations over time. Special focus in this article is placed on clinically studied biomarkers rather than promising preclinical markers of HF.
Natriuretic Peptides
Since the discovery of atrial natriuretic peptide (ANP) in 1981 and the subsequent discovery of brain natriuretic peptide in 1989,2,3 there has been considerable interest in natriuretic peptides for the assessment of ADHF. Originally termed brain natriuretic peptide due to the tissue type of initial isolation, now B-type natriuretic peptide (BNP) has been most fully evaluated for the diagnosis and risk stratification of HF. Derived from the 108-amino acid peptide pro-BNP, BNP (1–32 amino acids) is secreted by atrial and ventricular myocardium in response to wall stress, including volume overload. BNP has a circulating half-life of just 21 minutes, is metabolized by endopeptidases, and is relatively unstable in vitro. 4 Pro-BNP itself (1–108) has also been studied as a marker. 5 However, the amino-terminal portion of pro-BNP, NT-proBNP (33–108), has shown more stable in vitro characteristics and with a longer half-life (90 minutes) and has become a highly utilized biomarker in the diagnosis and management of HF. Natriuretic peptides have been validated in both systolic HF (HFREF) and HF with preserved ejection fraction (HFPEF). 6 Furthermore, natriuretic peptides may return to normal or decrease in patients’ systolic or diastolic dysfunction when clinical HF resolves,7,8 though a substantial response is required to alter prognosis. 9
B-type natriuretic peptide
The first large study examining the utility of BNP for the diagnosis of ADHF as a cause of dyspnea was the Breathing Not Properly Multinational Study. 10 An elevated BNP level of >100 pg/mL had a positive predictive value of 79%, and values below 50 pg/mL had a negative predictive value (NPV) of 96% [positive and negative likelihood ratios (LR) were 2.6 and 0.05,respectively]. 10 Many subsequent studies have attempted to stratify the utility of BNP and NT-proBNP. The test characteristics of these studies are summarized in Table 1. The first large NT-proBNP study was reported in 2005, called the N-Terminal Pro-BNP Investigation of Dyspnea in the Emergency Department (PRIDE) study, 11 which sought to determine optimal cut points for evaluating acute dyspnea. Cutoffs of 450 and 900 pg/mL were utilized for patients less than and greater than 50 years of age, respectively, and achieved good sensitivity. A threshold of <300 pg/mL virtually excluded HF. 11 Studies attempting to stratify by renal function found an acceptable ability to exclude HF with a threshold of 1200 pg/mL [glomerular filtration rate (GFR) <60 mL/min/body surface area (BSA)]. 12 Another study utilized tertiles of age to establish thresholds, with 90% sensitivity achieved in each of patients <50, 50–75, and >75 years of age when 450, 900, and 1800 pg/mL were utilized, respectively. 13 These values are reflected in the current European Society of Cardiology Guidelines 14 as well as the guideline recommendations of AHA (American Heart Association), HFSA (Heart Failure Society of America), and the ISHLT (International Society for Heart and Lung Transplantation).15–17
Summary of test characteristics of BNP or NT-proBNP for the diagnosis of HF from selected studies.
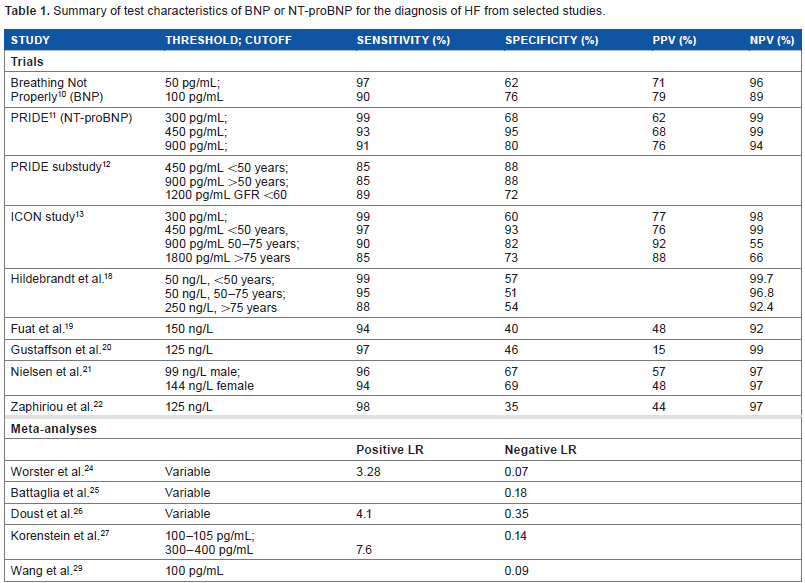
Additional studies have attempted to analyze the role of NT-proBNP in the exclusion of HF in specific clinical settings. In the primary care realm, thresholds of 50, 75, and 260 ng/L achieved excellent NPV for excluding HF for tertiles of age (<50, 50–75, and >75 years of age, respectively). 18 A universal cutoff near 125 ng/L achieved reasonable NPV, similar to other analyses.19–22 As noted previously, 23 positive predictive values for NT-proBNP are poor, generally in the range of 50%–60% when the cutpoints above are chosen for excluding HF.
Emergency department laboratory values have been evaluated separately, resulting in several important meta-analyses. One study showed a positive LR in the Emergency Department (ED) of 3.28 and negative LR of 0.07 for NT-proBNP, with variable thresholds, 24 while others have similar results with a negative LR of 0.18. 25 For HFREF only, BNP performed well with a positive LR of 4.1 and a negative LR of 0.35. 26 Similar results have been seen in other studies.27–29 Although less common, a higher threshold of 300–400 pg/mL had a stronger positive LR at 7.6 in one study. 27 These suggest that there is good utility for NT-proBNP for the stratification of nonspecific dyspnea in the acute care settings, although the highest utility is when age-specific thresholds are utilized. Utilization of NT-proBNP as a screening tool is uncertain at best, though studies indicate that, especially in an elderly population, there is likely little benefit given the added cost.28,30
Although only adjunctively useful in the diagnosis of HF, the presence of pleural effusions in patients with possible HF is common, and there appears to be utility in the measurement of NT-proBNP in pleural fluid. A meta-analysis performed by Janda and colleagues 31 showed a positive LR of 15.2 and a negative LR of 0.06 with a threshold of roughly 1500 pg/mL. Similarly, another meta-analysis by Zhou and colleagues 32 revealed a sensitivity of pleural fluid NT-proBNP of 95% and specificity of 94%.
Forms of B-type natriuretic peptide have shown benefit in the prognosis of HF events, mortality, and other outcomes. 33 Several systematic reviews have been published showing that NT-proBNP is a useful marker for predicting all-cause mortality and cardiac-specific mortality.4,26 Not only has N T-proBNP been shown to be useful in prognosis in ADHF but it can potentially be used to monitor response to therapy in the acute setting 8 as well as chronic therapy. Serial monitoring of NT-proBNP has shown utility for decreasing all-cause mortality as well as HF hospitalizations in patients treated for chronic HF compared to symptom-driven therapy alone. This has been elucidated in multiple studies, driven mostly by intensification of HF therapy.4,34–40 Interestingly, only large reductions (>80% decrement) in NT-proBNP or BNP values reflect an improve prognosis, whereas more modest changes are not associated with benefit. 9
Results of years of analysis of B-type natriuretic peptide clearly define its usefulness in several areas: 1) adjunctive laboratory testing for the exclusion of HF in breathless individuals, 2) prognostic information at the time of diagnosis of ADHF, and 3) prognostication and response to therapy in the chronic HF outpatient setting.
Atrial natriuretic peptide
Another natriuretic peptide that has been explored is the atrial natriuretic peptide (ANP). ANP has theoretical pathophysiologic advantages over the BNP and NT-proBNP, as the former is more prevalent in serum and released by the atria under volume overload conditions whereas the latter are related to increased wall stress in the ventricles and released by cardiomyocytes. Therefore, BNP-derived biomarkers are theoretically less specific, instead reflecting general myocardial dysfunction including cardiomyopathies. 41 However, analysis of ANP has been fraught with difficulty because of the short half-life of plasma ANP and the relative instability of NT-proANP. 41 As a result, analysis of the more stable mid-regional pro-atrial natriuretic peptide (MR-proANP) has been undertaken. In general, increased stability is found with prohormones.
In a meta-analysis by Hu and colleagues 42 of five previous trials of MR-proANP as a diagnostic marker of HF,43–47 a 90% sensitivity and a 68% specificity for the diagnosis of HF in dyspneic patients was found. However, there were notable differences between these trials. Nevertheless, MR-proANP performed similarly to BNP diagnostically,44,46,48 yet it may yield additional benefit to equivocal BNP-based values.43,45,47
Additional considerations include the various confounders. Some authors have suggested that MR-proANP may be able to provide diagnostic certainty in cases of impaired renal function or obesity, 47 though other studies could not confirm such an effect.43,44 Unfortunately, it seems that atrial arrhythmias may disproportionately affect MR-proANP due to its secretion from atria. 43
MR-proANP has been assessed for utility in prognostication for patients presenting with ADHF, and performed similarly to NT-proBNP. 43 In this study, its prognostic performance was enhanced by addition of midregional proadrenomedullin to the model (discussed below). MR-proANP was also shown to be of prognostic value in chronic, compensated HF and outperformed NT-proBNP. 49 MR-proANP has not been assessed in the longitudinal management of chronic HF patients.
At present, the role of MR-proANP is primarily restricted to “uncertain” BNP values, prognostication in combination with other peptides, and prognostication in chronic HF patients, the latter finding requiring more study.
Galectin-3
Another potential marker of HF is galectin-3 (Gal-3), a β-galactosidase binding protein first discovered in 2004 by Sharma and colleagues. 50 It was found that this protein was uniformly overexpressed in rat cardiomyopathy models and predicted progression to HF in these experimental studies. Interestingly, infusion of Gal-3 resulted in expression of markers of myocardial fibrosis and clinical left ventricular dysfunction in the model. Furthermore, studies have subsequently shown that Gal-3 was necessary for the development of fibrosis, 51 prompting further interest in Gal-3 as a predicator of response to antifibrotic medications 52 and as a therapeutic target. 53
The first study to evaluate the ability of Gal-3 to diagnose HF as the cause in breathless individuals was by van Kimmenade et al. 54 , who evaluated patients in the emergency department both with NT-proBNP and Gal-3 as part of the PRIDE study. Although it fared satisfactorily with an area under the curve (AUC) of 0.72, with a cutoff of 6.88 ng/mL best stratifying the etiology of symptoms, the sensitivity was 80% and specificity was 52%, which were worse than those in the NT-proBNP evaluation of dyspnea. Notably, correlations between Gal-3 and age, blood urea nitrogen (BUN), and creatinine may explain some of the issues with its utility as a diagnostic biomarker. 55 Other cohorts have suggested Gal-3 may be affected by gender, diabetes, hypertension, hypercholesterolemia, body mass index (BMI), and tobacco use. 56
However, other studies of Gal-3 for the diagnosis of HF suggested more positive results. In a study by Yin and colleagues, 57 AUC values for Gal-3 and BNP were very similar at 0.891 and 0.896, respectively, yielding a sensitivity and specificity for the former of 94% and 65%, respectively. Another study found that Gal-3 correlated significantly with several echocardiographic markers of cardiac dysfunction, including indices of right-sided failure, suggesting a potential role for the biomarker. 55 Gal-3 has also effectively predicted HF in patients after recent myocardial infarction (MI). 58
Overall, the additive benefit of Gal-3 beyond NT-proBNP is debated,54,59 though its prognostic utility has been suggested in numerous clinical trial cohorts, including CORONA and COACH, 60 PRIDE, 54 Val-HeFT, 61 PROTECT, 62 CARE-HF, 63 and DEAL-HF. 64 It is validated in the Framingham cohort as well. 56 Gal-3 has been added to the most recent 2013 ACC/AHA guidelines in the management of HF. 65 It is the prognostic realm in which Gal-3 appears to be most useful, both during ADHF and in the outpatient setting.
Soluble ST2
The ST2 receptor is a member of the interleukin-1 (IL-1) family, which is expressed on cardiac myocytes, but expresses a soluble portion (sST2) that is readily measurable in peripheral blood. 66 In preclinical studies, sST2 had been shown to be increased after cardiac myocytes stress events, including MI and myocyte mechanical strain, 66 the latter finding prompting interest in the use of sST2 for evaluation of clinical HF. 67 In the first clinical study of sST2, significant correlation was noted between sST2 and ANP, BNP, and NT-proBNP. Additionally, sST2 provided prognostic value independent of natriuretic peptides. 67
The first study to rigorously examine the diagnostic utility of sST2 in the ADHF setting failed to show significant predictive ability to stratify patients presenting with HF, with AUC of 0.62 and a nonsignificant odds ratio for HF. 68 Additionally, an analysis of the PRIDE study with ST2 69 showed an AUC for ST2 of 0.74, which was noted to be worse than previously reported for NT-proBNP. Interestingly, stratification of NT-proBNP by ST2 levels revealed that ST2 levels were more likely to not be elevated in acute HF, which may reflect a timing delay, preventing its utility as a biomarker useful in the diagnosis of acute HF.
Soluble ST2 has been more extensively studied in the context of prognosis at this point – both in the value at presentation69,70 and as a serial marker, 71 in various settings. 72 However, sST2 has shown prognostic value independent of left ventricular ejection fraction (LVEF). 73 ST2 has also been added to the most recent ACC/AHA guidelines in the management of HF as a biomarker with potential additive prognostic value. 65 As a result, utility of sST2 is in prognosis for ADHF, especially in the context of diastolic failure, where there are relatively fewer biomarkers of utility.
Mid-regional Proadrenomedullin
Adrenomedullin is an endogenous vasodilatory peptide, isolated initially from pheochromocytoma extracts. 74 Subsequent studies localized this peptide to the myocardium, 75 both atrial and ventricular, suggesting a possible role in volume homeostasis. This was studied initially in the HF model, where it was found that circulating levels were statistically higher in HF patients than controls 76 and other dyspneic patients. 77 Immunohistochemical staining was greater in the failing ventricle than the control ventricles. 75 In contrast to Gal-3, adrenomedullin has been shown to have beneficial effects, most notably on volume status, and has been studied as a therapeutic agent. Indeed, infusion of adrenomedullin resulted in a decrease in pulmonary capillary wedge pressure via increase in urine volume and urine sodium excretion. 78
For the diagnosis of acute HF in dyspneic individuals, mid-regional proadrenomedullin (MR-proADM) performed worse than NT-proBNP in one study (PRIDE) with an AUC of 0.8 compared to 0.94 for NT-proBNP. 43 However, others have argued that the addition of MR-proADM to NT-proBNP can improve diagnostic accuracy via an increase in AUC from 0.81 (NT-proBNP alone) to 0.84 (combined biomarkers). 79 Various comorbidities correlate with MR-proADM, and therefore may harm the diagnostic accuracy of MR-proADM, including age, hypertension, renal failure, coronary artery disease, and diabetes mellitus. 77 As a result, MR-proADM has fallen out of favor as a diagnostic tool.
It must be noted that MR-proADM has performed well as an assay for the prediction of adverse events after myocardial infarction80,81 or HF 81 and a biomarker with better prognostic capacity than the natriuretic peptides.47,77,82 It has been studied with MR-proANP and can perform well as an adjunctive biomarker in this setting.43,82 Therefore, the current role for MR-proADM is a secondary one as an adjunctive prognostic marker in the setting of ADHF.
Copeptin
Derived from preprovasopressin, copeptin is a carrier protein of serum vasopressin (AVP). 83 As with other vasoactive hormones, AVP is rapidly degraded both in vivo and ex vivo, limiting its utility for direct analysis, 84 whereas copeptin, secreted in equal amounts with AVP, is stable for a sufficient period for laboratory assay. 85 In addition to the well-known stimuli for secretion of AVP, decreased effective circulatory pressures and hyperosmolarity, increased cardiac filling pressures have been cited as a stimulus for AVP release.86,87 As a result of these data and the pathophysiology relating to downstream effectors of V1a and V2 receptors, it has been argued that AVP may have a yet-untapped potential for neurohormonal blockade in HF, and trials have assessed AVP antagonism for this purpose.88,89
Results regarding the utility of copeptin in the diagnosis of HF are mixed. 90 Copeptin has been shown to be associated with several echocardiographic parameters of left ventricular dysfunction, including LVEF, left ventricular end-diastolic volume (LVEDV), and wall motion index score (WMIS), and predictive of future HF events. 91 Likewise, it has been used to exclude MI. 92 However, in clinical HF, while prospective studies have found a reasonable negative predictive value of 95%, sensitivity and specificity were low at 68% and 51%, respectively. 93 Other studies have suggested a limited utility of copeptin in addition to traditional biomarkers, 94 and in one study, copeptin was unable to increase the discriminatory capacity of NT-proBNP for unspecified dyspnea in the ED. 79
However, copeptin has shown to be useful in prognostication in ADHF, both in the short and long term,95,96 and may be complementary97–99 or may perform superiorly to NT-proBNP in this regard.100–104 Specifically, elevated copeptin level was associated with elevated short-term mortality and need for transplantation, particularly when combined with the presence of hyponatremia. 104 Its prognostic capacity holds independently of renal function. 105
Copeptin should be used in the prognostication in ADHF and chronic HF and may provide additional data to that of NT-proBNP in this regard. There is likely no benefit for utilization in the diagnosis of exclusion of ADHF as a cause of dyspnea in acute settings.
Troponin-T
Although typically thought of as a biomarker for the diagnosis of acute coronary syndromes, troponin-T has also been investigated in the setting of HF. Cardiac troponin-T (cTnT) is a breakdown product of the cardiac troponin–tropomyosin complex, which is structurally distinct from skeletal muscle troponin-T, 106 and, therefore, has broad utility for ischemic cardiac conditions. More recently, advanced assays have been developed that allow detection of cTnT more precisely at lower thresholds, referred to as high-sensitivity troponin-T (hs-cTnT). 107
Troponin-T has less frequently been utilized as an adjunctive biomarker in the diagnosis of HF, though several factors favor its utilization in the context of HF. cTnT is associated with not only LV end diastolic pressure, diastolic parameters, ejection fraction, pulmonary pressures108–111 but also physical exam findings in acute HF, including an S3 gallop and pulmonary rales, 112 and clinical decongestion is associated with clearance of elevated troponins.111,113
There are several limitations to cTnT in this context. Although troponin elevations are seen in ADHF,79,114 the differential diagnosis for elevations in troponin levels is broad and includes, primarily, acute coronary syndromes, pulmonary embolism, stroke, tachyarrhythmias, sepsis, or shock, among several others, which limits the specificity of the biomarker for any particular diagnosis. 115 Additionally, age alone may be associated with elevated troponins in ill patients with non-cardiopulmonary disease, 116 and HF comprises a small proportion of non-ACS diagnoses in the acute setting. 117 Even within HF populations, patients with ischemic cardiomyopathy have greater elevations in troponins than do non-ischemic cardiomyopathies, 118 and there may be gender-related differences in troponin values. 119 Nevertheless, troponin values should be obtained in the work-up of new HF to exclude Type I MI as an etiology in addition to risk stratification.120,121
More importantly, cTnT, and to a lesser extent troponin-I, 122 has been associated with prognosis.123,124 Worsening inhospital troponin levels in ADHF is also associated with a worse prognosis. 125 Serial elevated troponins in the out patient setting have been shown to be independently associated with mortality, cardiac transplant, and HF hospitalization, especially in combination with elevated NT-proBNP.126,127 Increased troponin-T levels are associated with increased risk of development of HF,97,128,129 and elevated troponins are a strong, independent prognostic marker in the hospitalized population for future HF98,107,125 and mortality,114,125,130–134 often independently of NT-proBNP levels or with additive benefit.70,97
As a result of these data, it would be reasonable to obtain cTnT level at 1) presentation with ADHF, as it is a useful prognostic marker and a marker for evaluating the potential for a type 1 myocardial infarction, and 2) in the outpatient setting as a strong indicator of prognosis both for mortality and re-hospitalization.
Neutrophil Gelatinase-Associated Lipocalin
Neutrophil gelatinase-associated lipocalin (NGAL), is a 25-kDa glycoprotein expressed by neutrophils and some epithelial cells as well as renal tubular cells and hepatocytes, which was first detected as a urinary biomarker in acute tubular injury.135,136 However, there are data supporting the utility for NGAL in the assessment of ADHF and chronic HF. One early study described a significant correlation between NGAL and NT-proBNP and significant association between higher NGAL levels and NYHA class as well as cardiovascular events. 135 Although a significant correlation with renal function is observed, there were elevated levels found in patients with normal GFR, suggesting a separate inflammatory pathway, and experimental models suggest within-myocardium expression of NGAL. 135
Prognostically, increased levels of NGAL were initially shown to predict mortality and cardiovascular events in ST-elevation MI (STEMI) patients treated with percutaneous coronary intervention (PCI), 137 but have subsequently shown to predict not only HF after STEMI 138 but also increased mortality and HF readmissions from ADHF when measured at admission.139,140 In the GALLANT study, plasma NGAL at discharge was also predictive of 30-day outcomes, including mortality and readmissions, more so than BNP alone, but greatest in combination with BNP. 141 In a substudy of COACH, NGAL was predictive of mortality when measured just before discharge, even after adjusting for chronic kidney disease. 142 These observations were not able to be replicated in the CORONA cohort. 143
In contrast to ADHF, in chronic HF, serum and urinary levels of NGAL are elevated compared to controls, but NGAL does not correlate with echocardiographic data.136,144 Prognostically, in chronic HF, elevated NGAL levels were correlated with mortality, though not after adjustment for renal function. 145 Additionally, NGAL levels have also been shown to be independently associated with indices of anemia. 146 Together, these variables decrease the utility of NGAL in the outpatient setting. A notable finding with regard to NGAL has been the ability to predict acute kidney injury in patients admitted with ADHF,140,147–150 though a few studies have failed to duplicate this result.151,152
There is little role for NGAL in the diagnosis of ADHF. Nevertheless, the optimal role for NGAL is utilization upon admission for ADHF to predict acute kidney injury during the hospitalization, and upon discharge as a reliable predictor of short-term events and rehospitalization. There appears to be little utility in chronic, compensated HF.
A summary of the biomarkers listed here is displayed in Table 2 with an analysis of their relative abilities to adjunctively diagnose, prognosticate, and inform outpatient management.
Utility of biomarkers in various clinical settings.
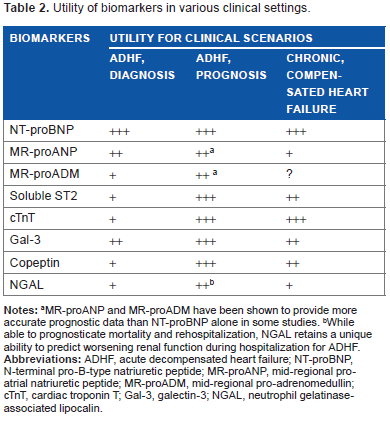
MR-proANP and MR-proADM have been shown to provide more accurate prognostic data than NT-proBNP alone in some studies.
While able to prognosticate mortality and rehospitalization, NGAL retains a unique ability to predict worsening renal function during hospitalization for ADHF.
Novel Clinically Relevant Biomarkers
Several additional biomarkers deserve discussion. These biomarkers are being evaluated for their ability to diagnose or prognose in acute or chronic HF, but their current clinical data is sparse. These markers show promise but require further study before being routinely used. The first group of biomarkers is urinary or renal-derived proteins. Similar to NGAL, both β-trace protein and cystatin C, measures of impaired renal function, have been tested in the setting of ADHF, and showed superiority to markers of renal function in predicting death or rehospitalization. 153 Additionally, two urinary markers, KIM-1 and IL-18, were evaluated in the context of ADHF; however, only the latter was associated with mortality in follow-up, and neither biomarker predicted renal insufficiency during hospitalization. 151 The second biomarker relates to the observation that the parathyroid–calcium axis has been implicated in the pathogenesis of HF. Parathyroid hormone (PTH) not only correlates with BNP levels in ADHF patients, but PTH was superior to BNP in predicting the presence of HFPEF and advanced HFREF, and predicting HF hospitalization in one study. 154 As ADHF is a pro-inflammatory state, likely due in part to poor tissue perfusion, inflammatory markers have been evaluated in ADHF. For example, CXCL16 has been identified and used to predict mortality in myocarditis patients. 155 A target of CXCL12, stromal cell-derived factor one (SDF-1), has been shown to predict episodes of ADHF and mortality after adjusting for cardiovascular disease (CVD) risk factors. 156 Large proteomic analyses have been undertaken to evaluate for potentially useful biomarkers. One of these yielded a novel biomarker, angiogenin, which was able to distinguish individuals with HF (HFREF or HFPEF) from controls with AUC of 0.88 as well as predict short-term mortality. 157 The most contemporary field of biomarker study is microRNAs, which are small nucleotide fragments that serve as modulators of gene expression and reflect CVD states. Several circulating miRNAs have been tested and have the potential to diagnose ADHF and may even be able distinguish differences in HF states, including HFREF from HFPEF, though a thorough discussion is outside the scope of this review.158–160
Conclusions
The above biomarkers represent the majority of the spectrum that has shown any significant ability to stratify breathless patients by etiology. While MR-proADM, soluble ST2, copeptin, cTnT, and Gal-3 showed some promise for the ability to provide diagnostic utility, the mainstay of diagnostic biomarkers continue to be the natriuretic peptides, as these novel biomarkers have not performed superiorly to NT-proBNP. Other biomarkers can be adjunctively utilized for risk stratification and prognostication. ANP fragments as biomarkers have been shown to be superior in some studies, though assays for ANP are not as common as those for NT-proBNP. Thus, NT-proBNP as a biomarker will continue to be the primary laboratory adjunct to the history and physical exam for evaluating the diagnosis of ADHF in the setting of undifferentiated dyspnea.
Author Contributions
Wrote the first draft of the manuscript: ANR. Contributed to the writing of the manuscript: ANR, WLM. Agreed with manuscript results and conclusions: ANR, WLM. Jointly developed the structure and arguments for the paper: ANR, WLM. Made critical revisions and approved final version: ANR, WLM. Both authors reviewed and approved of the final manuscript.