
Abstract
This article reviews the pharmacology and clinical evidence of the use of dabigatran etexilate (DE) in the prevention and treatment of venous thromboembolism (VTE). Published data in English language were identified from MEDLINE and Current Content database (1966 to January 30, 2011) using the search terms dabigatran, VTE, deep vein thrombosis, and pulmonary embolism. Citations from available articles were reviewed for additional references. DE is an oral direct thrombin inhibitor that has a rapid onset of action, achieving peak anticoagulation effect in 0.5–2 hours. In clinical studies, DE has demonstrated superiority and non-inferiority to enoxaparin for VTE prophylaxis and non-inferiority to warfarin for VTE treatment. A common side effect of DE is gastrointestinal complaints. The overall rates of major bleeding were low, and minor bleeding was commonly noted but similar in incidence to other anticoagulant (enoxaparin and warfarin). Future studies should focus on long-term efficacy and safety compared to other anticoagulants, and for other clinical indications.
Introduction
Venous thromboembolism (VTE) is the third most common cause of cardiovascular mortality after coronary heart disease and stroke in the United States (US). 1 The annual incidence of VTE is reported to be 100 to 192 per 100,000 person-years.1,2 Because only 1 in every 3 cases of VTE is diagnosed, the actual incidence of VTE in the United States may be substantially higher. 3 Incidence of VTE among in-patients is 10% to 20% and rises to approximately 80% in patients with spinal cord injury, major trauma, and who are critically ill. 2 Venous thromboembolism is idiopathic 25% to 50% of the time. 4 VTE is reported to be the second most common medical complication, the second most common cause of excess hospital length of stay, and the third most common cause of excess hospital mortality and charges. 5
Anticoagulants remain the main state of therapy for prevention and treatment of VTE. Until recently, warfarin remained the only oral anticoagulant option available in the US. However, it's narrow therapeutic index, large inter-patient variability in dose response and numerous drug and food interactions continue to remain a concern regarding its use.6,7 Other options for anticoagulation include unfractionated heparin, low molecular heparin, factor Xa inhibitors, all of which are only available in parenteral forms in the US.8,9 Currently, the 8th edition of the American College of Chest Physicians Guidelines on Anti-thrombotic and Thrombolytic Therapy recommend all these anticoagulants as therapeutic options for both prevention and treatment of VTE.1,2
Direct thrombin inhibitors (DTI) represent another newer class of anticoagulants. The three intravenous agents in the US market are primarily used in the treatment of heparin induced thrombocytopenia (lepirudin, argatroban) and during percutaneous coronary interventions (bivalirudin).10,11 Ximelagatran was a previously developed oral DTI that was approved and available for use in VTE treatment and prevention in selected European countries for a brief period in 2005. The manufacturer subsequently withdraw the medication from the market and further applications for marketing the drug in other countries including the US, due to the risk of hepato-toxicity and acute coronary syndrome (ACS) events. 13 Dabigatran etexilate is another oral DTI that has recently been approved by the US Food and Drug Administration (October 19, 2010) and in Canada for prevention of thromboembolic events in patients with atrial fibrillation. 12 Prior to this, dabigatran etexilate has gained approval in Europe and Canada in 2008 for the treatment and prevention of VTE. 13 This article will focus on the discussion of the use of dabigatran etexilate as a therapeutic alternative, for prevention and treatment of VTE.
Pharmacology of Dabigatran
Mechanism of action
Thrombin generation begins initially with either vessel injury, resulting in exposure of tissue factor and activation of the extrinsic pathway of coagulation, or slow blood flow, which activates the intrinsic pathway of coagulation. 14 Thombin converts fibrinogen to fibrin and activates factor V, VIII and XI, which stimulate production of more thrombin. 14 Fibrin cross link the thrombin and form a hemostatic plug. Thrombin also plays an important role in platelet activation. 14 Thrombin has three structural domains, one active site and two exosites. Exosite 1 acts as a dock for substrates such as fibrin in order to promote orientation for active site binding. Exosite 2 is the heparin binding domain. The bivalent DTI, such as lepirudin and bivalirudin, bind to both the active site and exosite 1. The univalent DTI, argatroban and dabigatran, bind only to the active site.10,11 Thus, DTI are able to inactivate both fibrin-bound and unbound thrombin, unlike unfractionated heparin and low molecular weight heparin, which inactivate non-fibrin bound thrombin only.
Dabigatran is a polar, permanently charged molecule and therefore has minimal oral bioavailability itself. Thus, a pro-drug, dabigatran etexilate was generated. Dabigatran etexilate undergoes hydrolysis in vivo to the active molecule, dabigatran. 15 Dabigatran is a competitive DTI. 15 It has high affinity for the active site of thrombin.
Pharmacokinetics
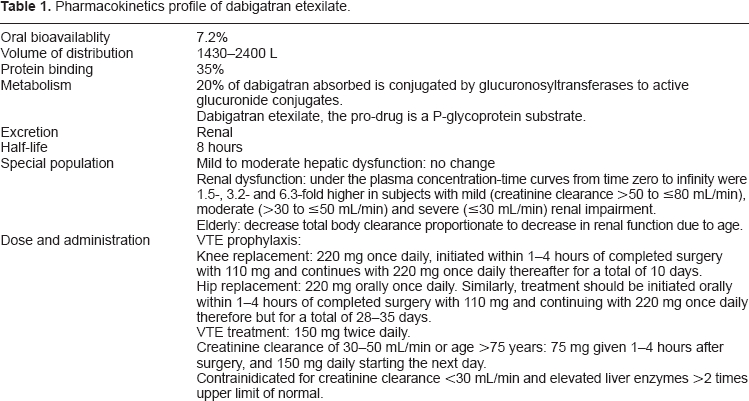
Table 1 summarizes the pharmacokinetics parameters in dabigatran.
Pharmacokinetics profile of dabigatran etexilate.
Healthy volunteers
The pharmacokinetics profile of dabigatran etexilate has been evaluated in health volunteers.16,17 In an open-label, 3-way crossover study, dabigatran etexilate 150 mg as a single oral dose, was administered to 18 male volunteers in the fasted state, after administration of food and with coadministration of pantoprazole. Food had no effect on the extent of absorption of dabigatran etexilate. A decrease in the mean dabigatran area under the concentration curve (AUC0-∞) (from 904 to 705 ng · h/mL) occurred with coadministration of pantoprazole. 16 Whether this interaction is clinically significant is not known.
In another study, dabigatran etexilate or placebo was administered orally at single doses of 10–400 mg to 40 healthy volunteers or at multiple doses of 50–400 mg three times daily for 6 days to a different group of 40 healthy individuals. 17 Absorption of dabigatran etexilate was rapid with peak plasma concentrations achieved within two hours of administration. The elimination half-life was reported to be 8–10 hours and 14–17 hours with single and multiple dose administrations, respectively. Dabigatran etexilate exhibited linear pharmacokinetics characteristics with dose-proportional increases in maximum plasma concentration and area under the curve. Steady-state was reached within three days with continuous twice daily dosing. The mean apparent volume of distribution during the terminal phase was 1860 L (range 1430–2400 L) and the apparent total body clearance after oral administration was 2031 mL/min (range 1480–2430).
Blech et al evaluated the oral bioavailability of dabigatran etexilate. 18 Ten healthy volunteers were randomized to receive one dose of oral dabigatran etexilate 200 mg or an IV infusion of dabigatran 5 mg. Dabigatran etexilate was rapidly converted to dabigatran, with peak plasma dabigatran concentrations being attained after approximately 1.5 hour. The bioavailability of dabigatran after oral administration was 7.2%. Dabigatran etexilate and dabigatran are both not metabolized by the cytochrome P450 system. Additionally, dibagatran does not inhibit or induce cytochrome activity. Approximately 20% of dabigatran is conjugated by glucuronosyltransferases to active glucuronide conjugates. Unabsorbed dabigatran is eliminated in the feces after oral administration. Drug absorbed into the blood stream is eliminated by the kidney. The mean terminal half-life of dabigatran was approximately eight hours. 18
Protein binding studies with radiolabelled dabigatran showed that 35% of dabigatran was bound to plasma protein. 19 Because of the low percentage of protein binding, displacement interactions appear to be unlikely. Dabigatran etexilate but not dabigatran, is a substrate of P-glycoprotein. 20
Patient undergoing hip replacement
In a multicenter, open-label study, 59 patients underwent total hip replacement received a single dose of oral dabigatran etexilate 150 mg, administered one to three hours following the surgical procedure. 16 Immediate onset of absorption was seen with the maximum plasma concentration of dabigatran observed after 6 hours. Compared with healthy volunteers, the pharmacokinetics postoperative profile demonstrated a delay peak concentrations.
Elderly
An open-label, parallel-group, single-centre study, was designed to evaluate the pharmacokinetic profile of dabigatran etexilate in 36, otherwise healthy elderly subjects. (aged ≥ 65 years). 21 Subjects were randomized to receive dabigatran etexilate 150 mg twice daily for seven days with or without coadministration of pantoprazole. Pantoprazole was administered at 40 mg twice daily, starting two days prior to dabigatran etexilate administration and ending on the morning of day seven. With twice-daily administration of dabigatran etexilate, plasma concentrations of dabigatran reached steady state within 2–3 days. The peak plasma concentrations were reached after a median of three hours. Coadministration with pantoprazole decreased the AUC(ss) by 24%. Half-life of dabigatran etexilate in this patient population was found to be 12–14 hours, which reflected the age related decrease in renal function leading to reduction clearance of dabigatran etexilate.
Hepatic dysfunction
The impact of moderate hepatic impairment on the pharmacokinetics of dabigatran etexilate was evaluated in an open-label, parallel-group study. 22 Twelve healthy volunteers and 12 patients with hepatic impairment (Child-Pugh classification B) received a single oral dose of dabigatran etexilate 150 mg. The mean values for area under the concentration-time curve, terminal half-life, and renal clearance of dabigatran were comparable between patients with hepatic impairment and healthy volunteers. Conversion of the dabigatran etexilate to active dabigatran was slower in patients with hepatic impairment, indicating that the liver was partly involved in bioconversion of dabigatran etexilate. However, total drug exposure was comparable between groups. The extent of dabigatran glucuronidation as well as protein binding was unchanged by liver disease; glucuronidation capacity was maintained in moderate liver disease.
Renal impairment
The pharmacokinetics profile of dabigatran etexilate in patients with renal impairment has been evaluated in an open-label, parallel-group, single center study. 23 Six healthy volunteers and 23 subjects with mid, moderate or severe renal impairment (creatinine clearance >50 to ≤80, >30 to ≤50 and ≤30 mL/min, respectively) was given a single oral dose of dabigatran etexilate 150 mg. Six subjects with end stage renal disease (ESRD) were given an oral dose of 50 mg. Compared with the pharmacokinetic profile in healthy subjects, the area under the plasma concentration-time curves from time zero to infinity were 1.5-, 3.2- and 6.3fold higher in subjects with mild, moderate and severe renal impairment. Changes in the maximum plasma concentration were modest, and the time to reach the C(max) was unchanged. In subjects with severe renal impairment, the mean terminal elimination half-life was doubled (28 hours vs. 14 hours in healthy volunteers). In patients with ESRD, the dose-normalized AUC was approximately twice the value in the control group. Haemodialysis removed 62%–68% of the dose. Exposure to dabigatran is increased by renal impairment and correlates with the severity of renal dysfunction. In patients with ESRD, dabigatran can be partly removed from the plasma by hemodialysis.
In conclusion, in healthy adults, oral dabigatran etexilate (DE) is approximately 7.2% absorbed and achieves its maximum plasma concentrations at approximately two hours after administration. Its half-life is approximately 12 hours. Steady state is attained in two to three days of treatment with twice daily dosing. The total and peak exposure have been shown to increase linearly and are dose proportional after single and multiple oral dosing of dabigatran etexilate in a dose range between 10–400 mg single dose and 50 to 400 mg three times daily dosing, respectively. Dabigatran is mainly (80%–85%) eliminated in the unchanged form via glomerular filtration. There are effects of age and creatinine clearance on dabigatran plasma concentrations. Dabigatran and dabigatran etexilate are neither substrates nor inhibitors or inducers of cytochrome P450 enzymes. Dabigatran is not a substrate, inducer or inhibitor of the efflux transporter P-glycoprotein. However, dabigatran etexilate, the pro-drug is a substrate but not an inducer or inhibitor of P-glycoprotein.
Pharmacodynamics
The pharmacodynamics of dabigatran has been evaluated in 80 healthy volunteers in doses varied from 10–400 mg as single dose and 50–400 mg three times daily. 17 Pharmacodynamic activity was assessed by blood coagulation parameters including activated partial thromboplastin time (aPTT), international normalized ratio (INR), thrombin time (TT), and ecarin clotting time (ECT). Time curves for aPTT, INR, TT and ECT paralleled plasma concentration-time curves in a dose-dependent manner. At the highest dose of 400 mg administered three times daily, maximum prolongations over baseline for aPTT, INR, TT and ECT were 3.1 times, 3.5 times, 29 times and 9.5-fold times, respectively. Of the four assays, TT and ECT exhibited the greatest sensitivity and precision within the anticipated therapeutic dose range. 17
Pharmacodynamics of dabigatran has also been evaluated in elderly subjects. Thirty-six healthy elderly subjects (aged ≥ 65 years) were randomized to receive dabigatran etexilate 150 mg twice daily for seven days either with or without coadministration of pantoprazole. Pantoprazole was administered at 40 mg twice daily, starting two days prior to dabigatran etexilate administration and ending on the morning of day seven. 21 Prolongation of the ECT and aPTT correlated with, and paralleled to the plasma concentration-time profile of dabigatran. The ECT increased in direct proportion to the plasma concentration, and the aPTT displayed a linear relationship with the square root of the plasma concentration. Pharmacodynamic effect was not affected by pantoprazole. The authors concluded that age did not affect the pharmacodynamic profile of dabigatran.
The impact of moderate hepatic impairment on the pharmacodynamics of dabigatran etexilate has also been evaluated in an open, parallel-group study. 22 Healthy volunteers (n = 12) and patients with hepatic impairment (Child-Pugh classification B; n = 12) received a single oral dose of 150 mg dabigatran etexilate. The aPTT, ECP, and TT relationships were essentially identical in both groups.
Similarly, the pharmacodynamic profile of dabigatran etexilate has been evaluated in an open-label, parallel-group, single center study. 23 Six healthy volunteers and 23 subjects with mid, moderate or severe renal impairment (creatinine clearance >50 to ≤80, >30 to ≤50 and ≤ 30 mL/min, respectively) was given a single oral dose of dabigatran etexilate 150 mg. Six subjects with end stage renal disease (ESRD) were given an oral dose of 50 mg. The AUC for prolongation of pharmacodynamic parameters (the aPTT and ECT) increased in line with the pharmacokinetic changes.
Overall, prolongation of the ECT, aPTT, INR and TT correlated with, and paralleled to the plasma concentration-time profile of dabigatran. Age, hepatic and renal dysfunction did not appear to affect the pharmacodynamic response of dabigatran.
Drug Interactions
No drug-drug interaction studies of dabigatran etexilate are published to-date. The following information is based on briefing materials submitted to the US Food and Drug Administration by the manufacturer. 20 The manufacturer has performed 13 pharmacokinetic or pharmacodynamic drug interaction studies with dabigatran (with atorvastatin, diclofenac, clopidogrel, proton pump inhibitors, H-2 antagonist, digoxin, P-glycoprotein inhibitors including verapamil, quinidine, clarithromycin, ketoconazole and amiodarone and P-glycoprotein inducer rifampin respectively). There was no significant influence of dabigatran etexilate on the pharmacokinetics of either atorvastatin or diclofenac, and the exposure of dabigatran was not significantly altered by these drugs. The bioavailability of dabigatran was modestly reduced (about 30%) in a Phase I study by the concomitant administration of the proton pump inhibitor pantoprazole while the H2-receptor antagonist ranitidine did not reduce the bioavailability of dabigatran etexilate. In a Phase I study, steady state coadministration of dabigatran and clopidogrel had no effect on the pharmacokinetics or pharmacodynamics of either compound. In this Phase I study, when a loading dose of clopidogrel (300 or 600 mg) was given, dabigatran AUC at steady state and Cmax at steady state increased by about 30% to 40%. As clopidogrel is a substrate of P-glycoprotein, a high loading dose may have competitively inhibited the ability of intestinal P-glycoprotein to bind to dabigatran. The steady state pharmacokinetics of digoxin (P-glycoprotein substrate) and dabigatran were not altered upon co-administration.
For drug interactions with P-glycoprotein inducers and inhibitors, the maximum increase in dabigatran bioavailability of about 150% was observed with ketoconazole, a potent inhibitor of P-glycoprotein. A similar effect was observed when a single dose of immediate-release verapamil was co-administered. After multiple dosing of verapamil (120 mg twice daily or four times daily), there was a 50%–60% increase in dabigatran bioavailability. Amiodarone and quinidine exerted similar effects (50%–60% increased bioavailability of dabigatran) as steady state verapamil. Clarithromycin did not significantly affect the pharmacokinetics of dabigatran. Consistent with all P-glycoprotein interactions between dabigatran etexilate and P-glycoprotein inhibitors, which should only occur in the gut, when verapamil was administered 2 hours before dabigatran etexilate intake, there was only a marginal (<20%) impact on dabigatran bioavailability.
After seven days pre-treatment with rifampin (600 mg daily), dabigatran AUC and Cmax were reduced by 66% and 67%, respectively. Seven days after cessation of rifampin treatment, dabigatran exposure was similar to when dabigatran etexilate was administered alone.
Clinical Trials
Prophylaxis of venous thromboembolism
Five large scale clinical trials of dabigatran etexilate for the prevention of VTE have been published (Table 2).24–28 The Boehringer Ingelheim Study in Thrombosis I (BISTRO 1) was designed to determine a therapeutic dosage range for dabigatran etexilate in patients after total hip replacement. 24 This was a multicenter, open-label, dose escalation study with treatment continued for 6–10 days, and patients were followed for 4–6 weeks after surgery. The first dose was administered 4–8 hours after surgery, or held until the following morning if the patient has vomiting or active in bleeding immediately after surgery. Multiple oral doses were assessed: 12.5, 25, 50, 100, 150, 200, and 300 mg twice daily, and 150 and 300 mg once daily. The study included 314 patients who were at least 18 years of age and weighed more than 40 kg. Patients were excluded if they had undergone other surgery or trauma within three months, had known cardiovascular disease or uncontrolled hypertension at the time of the study enrollment, had history of myocardial infarction within 6 months, history of intracranial hemorrhage or VTE, gastrointestinal bleeding, or pulmonary bleeding within one year, current bleeding diathesis, undefined renal or hepatic dysfunction, contrast media allergy, anticoagulant used within seven days, had histamine-2 receptor blocker or proton pump inhibitor treatment, thrombocytopenia, known alcohol or drug use, childbearing potential or pregnancy or leg amputation. The primary efficacy outcome was the occurrence of venographically confirmed deep vein thrombosis (DVT), symptomatic DVT or pulmonary embolism (PE). The study was not powered to detect efficacy differences among different doses. The overall DVT rate was 12.4%, with a highest rates occurring in the 12.5 mg group. The lowest rates were observed within the highest dosing groups (300 mg once or twice daily), but a dose-response relationship was not determined. There were no major bleeding events reported in this trial. Patients in the 300 mg twice daily group were discontinued from the study prematurely due to observed bleeding episodes from multiple sites within a few days of treatment. Results from this study suggest that a dosage of 12.5–300 mg twice daily will be effective at preventing VTE in high risk patients undergoing total hip replacement but 300 mg twice daily may cause more bleeding. Lower doses may be necessary in patients with renal dysfunction.
Pertinent clinical studies on the use of dabigatran in prevention and treatment of venous thromboembolism.
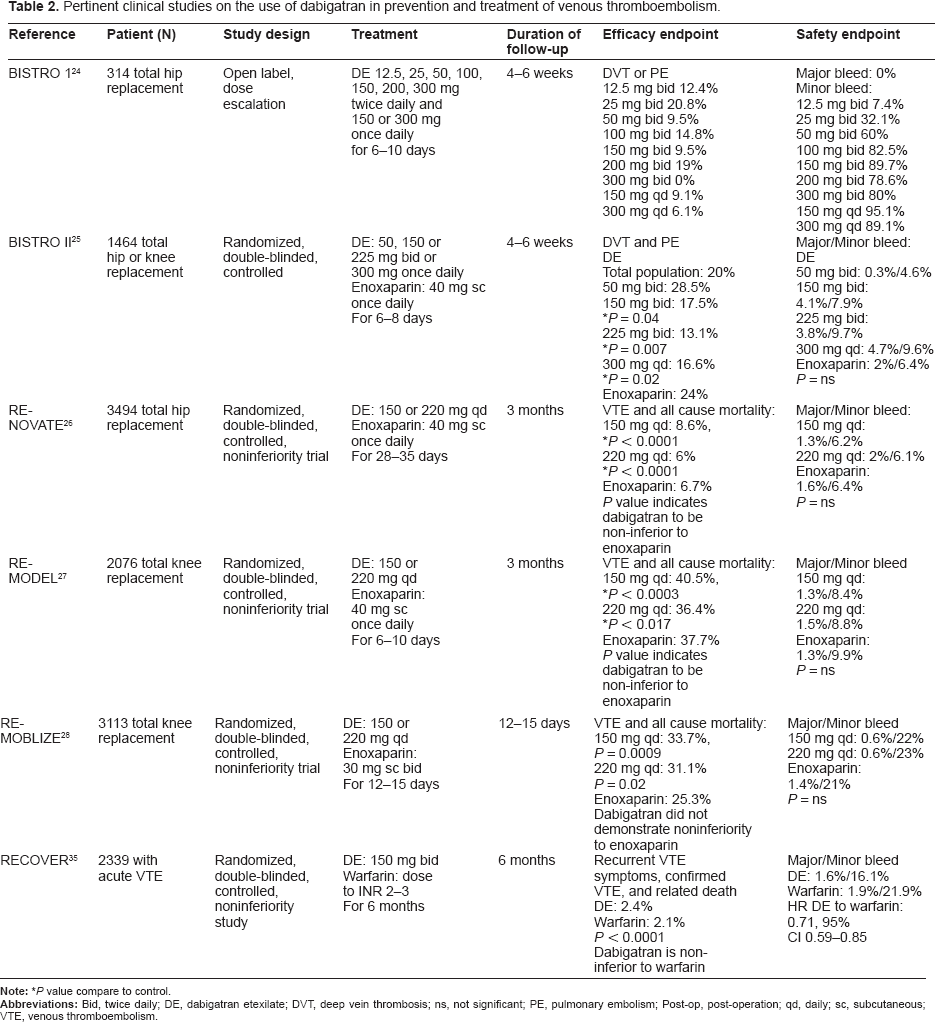
The BISTRO II trial was a randomized, double-blinded, parallel, active-control multicenter study designed to determine the dose-response relationship of dabigatran etexilate (both safety and efficacy) for prevention of VTE after total hip and total knee replacement. 25 Dabigatran etexilate dosing regimens: 50, 150 and 225 mg twice daily, as well as 300 mg once daily, were compared with enoxaparin 40 mg subcutaneously once daily. Dabigatran etexilate was administered one to four hours after surgery, and enoxaparin was given subcutaneously the evening before surgery according to product labeling. Treatment was continued for 6–10 days, and patients were followed for 4–6 weeks after surgery. Patient inclusion criteria and exclusion criteria were similar to those in BISTRO I. A total of 1464 patients were included in the efficacy analysis (total hip replacement (68%) or total knee replacement (32%)). The primary efficacy outcome was the occurrence of VTE during the treatment period. A significant dose-dependent decrease in VTE frequency was observed with increasing doses of dabigatran etexilate. Administration of dabigatran etexilate 150 mg twice daily, 300 mg once daily and 225 mg twice daily resulted in significantly fewer VTE compared with enoxaparin (17.4% (150 mg twice daily) vs. 16.6% (300 mg twice daily) vs. 13.1% (225 mg twice daily) vs. 24% (enoxaparin), P < 0.05 for comparison of each dose to enoxaparin); disregard of the type of surgery (knee or hip). However, no significant difference was noted in the frequency of VTE in patients receiving dabigatran etexilate 50 mg twice daily versus those receiving enoxaparin. Regarding the timing of initial dose, the frequency of VTE was significantly lower in patients receiving their first dose of dabigatran etexilate within two hours after surgery (P = 0.0005). The primary safety outcome was a frequency of major bleeding. Compared with enoxaparin, there was a higher, although non-significant, rate of major bleeding with dabigatran 150 mg twice daily and higher doses. There was no correlation noted between the timing of the first dose and bleeding event. This study was able to demonstrate a dose-response relationship for safety and efficacy. Larger studies are needed to further assess the risk of bleeding.
This Prevention of venous thromboembolism after Total Hip Replacement (RE-NOVATE) trial is a randomized, double-blinded, multicenter, non-inferiority study designed to compare the safety and efficacy of dabigatran etexilate with enoxaparin when given for VTE prevention in 3113 patients after total hip replacement. 26 Treatment groups were administered either dabigatran etexilate 220 or 150 mg orally once daily, with the first dose given as one half of the dose 1–4 hours after surgery, or enoxaparin 40 mg subcutaneously once daily starting the evening before surgery. If the patient was hemodynamically unstable after surgery, the first dose of dabigatran etexilate was administered the day after surgery as a full dose, followed by a second dose 12 hours later. Treatment was continued for 28–35 days in accordance with current VTE prevention recommendations. Bilateral venography was obtained within 24 hours of the last dose of treatment. Exclusion criteria was similar to those of BISTRO I and II, with more explicit definitions of hepatic and renal dysfunction (ALT or aspirate aminotransferase levels greater than twice the upper limit of normal, creatinine clearance <30 mL/min. The non-inferiority margin was set at 7.7% based on an enoxaparin VTE absolute reduction of 32.8% compared to no treatment. The primary efficacy outcome of total VTE and all-cause mortality was dabigatran etexilate 220 mg: 6%, dabigatran etexilate 150 mg: 8.6%, and enoxaparin 6.7%. It was concluded that dabigatran etexilate administered as either 150 or 220 mg orally once/day for 28–35 days after total hip replacement was non-inferior to enoxaparin. Major bleeding events occurred in 2%, 1.3% and 1.6% of patients receiving dabigatran etexilate 220 mg, dabigatran etexilate 150 mg, and enoxaparin, respectively. These observed differences were not statistically significant. The most frequent type of adverse event in each group was largely gastrointestinal related which included nausea, vomiting, and constipation. Alanine aminotransferase level increases greater than three times upper limit of normal were more common in the enoxaparin group (5%) than in either of the dabigatran etexilate dose group (3%) (P = 0.0081 for dabigatran 220 mg and P = 0.0061 for dabigatran 150 mg). Incidence of ACS events (confirmed unstable angina, myocardial infarction and cardiac death) were low (dabigatran etexilate 220 mg: five events; 150 mg: eight events; enoxaparin: nine events, P values not reported). Oral dabigatran etexilate 220 and 150 mg once daily each were demonstrated to be noninferior to enoxaparin subcutaneous 40 mg once daily in reducing the frequency of VTE and all-cause mortality when given for VTE prophylaxis in patients undergoing total hip replacement surgery. Extending the administration period did not appear to be related to increasing frequency of hepatic dysfunction and ACS events.
The Thromboembolism Prevention After Knee Surgery (RE-MODEL) study was a randomized, double-blinded, multicenter, active-control, non-inferiority trial designed to compare dabigatran etexilate 150 mg and 220 mg orally once daily versus enoxaparin 40 mg subcutaneously once daily in patients who underwent total knee replacement. 27 The study had similar inclusion and exclusion criteria as BISTRO II. 25 The primary endpoint was the same as that used in the RENOVATE study. 26 First dose of dabigatran etexilate was administered 1–4 hours after surgery as one half of the dose. If not clinically stable, a full dose was then given the following day followed by a second full dose 12 hours later. Enoxaparin was started after surgery as determined by local practice. Treatment period was 6–10 days. 2 Continuation after this time period was permitted at the discretion of the investigators. Patients were assessed up to three months after surgery. The median active treatment duration was similar among the treatment groups (7–8 days). The primary efficacy outcome with dabigatran etexilate, using either 220 mg or 150 mg once daily, was non-inferior compared with enoxaparin but did not show superiority (36.4%, 95% CI, 32.3%–40.6%, P = 0.0003; 40.5%, 95% CI, 36.3%–44.7%, P = 0.017; vs. 37.7%, 95% CI, 33.5%–41.9%) respectively. The absolute difference in total VTE and all cause mortality compared with enoxaparin was dabigatran etexilate 220 mg: −1.3% (95% CI, 7.3%–4.6%) and 150 mg 2.8% (95% CI, 4.1%–8.7%). The rate of major bleeding was not significantly different among the groups (dabigatran etexilate 220 mg 1.5% 0, 150 mg 1.3% and enoxaparin 1.3%). The frequency of ALT level elevations greater than 3 times the upper limit normal was similar between enoxaparin (4%), dabigatran etexilate 220 mg (2.8%) and 150 mg (3.7%), although P value was not reported. All abnormalities returned to baseline values during follow-up after the study conclusion. Incidence of ACS events were low (dabigatran etexilate 220 mg (0.44%); 150 mg (1%); enoxaparin (0.58%), P value not reported). This study demonstrated that dabigatran etexilate 220 gm and 150 mg taken orally once daily were each non-inferior to enoxaparin 40 mg subcutaneously once daily for prevention of VTE in patients undergoing total knee replacement. There was no significant difference in the frequency of major bleeding or overall rate of adverse events between either dose of dabigatran etexilate and enoxaparin. It is important to note that the dosing of enoxaparin (40 mg once daily) is different from what is typically employed in practice for this type of surgery (30 mg twice daily). Enoxaparin has not been approved for once daily dosing in patients undergoing total knee replacement surgery in the US. Use of lower dose of enoxaparin may lead to higher VTE events and a lower frequency of bleeding.
The Dabigatran versus Enoxaparin in Preventing Venous Thromboembolism Following Total Knee Arthroplasty (RE-MOBILIZE) study was a randomized, double-blinded, non-inferiority trial designed to assess oral dabigatran etexilate versus subcutaneous enoxaparin. 28 A total of 2615 patients were randomly assigned to dabigatran etexilate 150 mg or 220 mg once daily, or enoxaparin 30 mg twice daily for 12–15 days of treatment. The first dose of dabigatran etexilate was administered as a half-dose 6–12 hours after surgery. Enoxaparin was started 12–24 hours after surgery. The study had similar inclusion and exclusion criteria as BISTRO II. 25 Enoxaparin demonstrated superiority over dabigatran for the primary efficacy outcome of proximal DVT, distal DVT, PE and all-cause mortality (Dabigatran etexilate 220 mg 31.1%, P = 0.02; dabigatran etexilate 150 mg 33.7%, P = 0.0009; vs. enoxaparin 25.3%). Both doses of dabigatran etexilate failed to demonstrate non-inferiority to enoxaparin. The frequency of major bleeding events was higher in the enoxaparin group (dabigatran etexilate 220 mg 0.6%, 150 mg 0.6%, and enoxaparin 1.4% (P values were not reported)). Elevated ALT levels greater than 3 times the upper limit of normal occurred infrequently and similarly within each group (dabigatran etexilate 220 mg 0.7%, 150 mg 1% and enoxaparin 0.9% (P values were not report). Pulmonary embolism was confirmed in the dabigatran etexilate 220 mg group (0.7%) and in the enoxaparin group (0.57%). Cardiac adverse events (exact event not specified) were reported in nine patients in the dabigatran 220 mg group, ten patients in the 110 mg group and nine patients in the enoxaparin group. Findings from RE-MOBILIZE demonstrate that dabigatran etexilate was not as effective as enoxaparin in preventing total VTE and mortality. Differences in the study design and dosing regimen have been postulated to contribute to these findings. The dose of enoxaparin used was higher than previous studies (30 mg sc twice daily versus 40 mg sc daily) and the starting dose of enoxaparin was given at a mean of 20 hours after surgery. The mean duration of 13 days also varied from previous studies.
Friedman et al performed a pooled analysis of the RE-MOBLIZE, RE-MODEL and RE-NOVATE studies. 29 In total, 8,135 were included in this pooled analysis because they had available data evaluable for safety. These patients were randomized to receive dabigatran etexilate 220 mg or 150 mg once-daily, or subcutaneous enoxaparin (40 mg once-daily or 30 mg twice-daily). Efficacy analyses were based on the modified intention-to-treat population of 6,200 patients with an evaluable outcome. The composite outcome of major VTE and VTE-related mortality occurred in 3.3% of the enoxaparin group versus 3.0% of the dabigatran 220 mg group (−0.2%, 95% CI, −1.3% to 0.9%) and 3.8% in the dabigatran etexilate 150 mg group (0.5%, 95% CI, −0.6% to 1.6%). Major bleeding occurred in 1.4% of the enoxaparin group versus 1.4% of the dabigatran 220 mg group (−0.2%, 95% CI, −0.8% to 0.5%) and 1.1% of the 150 mg group (−0.4%, 95% CI, −1.0% to 0.2%). The authors concluded that oral dabigatran etexilate in dosages of 150 or 220 mg daily was as effective as subcutaneous enoxaparin 40 mg daily or 30 mg twice daily in reducing the risk of major VTE and VTE-related mortality after hip or knee arthroplasty and had a similar bleeding profile.
A similar pooled analysis performed by a group of Canadian investigators of the RE-MOBILIZE, REMODEL and RE-NOVATE studies also demonstrated similar results. 30 Compared with dabigatran, enoxaparin had a similar risk of symptomatic VTE plus all-cause mortality (0.9% versus 1.1%; OR, 0.76; 95% CI, 0.44 to 1.31) and bleeding (5.0% versus 5.6%; OR, 0.90; 95% CI, 0.71 to 1.15).
A meta-analysis was also performed with data from REMODEL, REMOBILIZE and RENOVATE studies. 31 No significant differences were detected between dabigatran etexilate and enoxaparin in any of the end-points analyzed although heterogeneity between the trials cannot be ruled out.
Trkulja et al attempted to perform an indirect comparison of the efficacy and safety of the use of dabigatran versus rivaroxaban in the prevention of VTE by performing separate meta-analysis of each of these agents and comparing the results. 32 The risk differences for symptomatic VTE were reported to be: rivaroxaban - enoxaparin = −0.4% (95% CI, −0.9 to 0.05%); dabigatran - enoxaparin = −0.09% (95% CI, −1.0 to 0.8%); rivaroxaban - dabigatran = −0.3% (95% CI, −1.3 to 0.7). Risk differences for clinically relevant bleeding were reported to be: rivaroxaban - enoxaparin = −0.99% (95% CI, 0.29%–1.69%); dabigatran – enoxaparin = 0.02% (95% CI, −1.0 to 1.0%); rivaroxaban - dabigatran = 0.97% (95% CI, −0.43 to 2.37). This demonstrated that both dabigatran and rivaroxaban appeared to not differ in efficacy/safety outcomes in the prevention of VTE. However, it is important to note that methodological differences did not allow direct comparison of the two agents and future study designed to compare these two new oral anticoagulants are needed.
The Cochrane Collaboration performed a systemic review of the use of direct thrombin inhibitor (including ximelagatran, dabigatran and desirudin) in the prophylaxis of VTE. 33 Four studies including 10183 patients were included (BISTRO II, REMOBILIZE, RENOVATE and REMODEL). Results were reported in combination with all other direct thrombin inhibitors. Overall, considering all direct thrombin inhibitors, there was no difference in major VTE compared to the use of low molecular weight heparin in both hip or knee replacement (Odds ratio 0.91, 95% CI, 0.69 to 1.19). No difference was observed with warfarin (Odds ratio 0.85, 95% CI, 0.63–1.15). More total bleeding were observed in the direct thrombin inhibitor group (for ximelagatran and dabigatran but not desirudin) in patients who underwent total hip replacement (odds ratio 1.40, 95% CI, 1.06 to 1.85) compared with low molecular weight heparin, but no difference was observed with warfarin in total knee replacement (odds ratio 1.76, 95% CI, 0.91–3.38).
Fuji et al assessed the efficacy, safety, and dose-response of dabigatran etexilate in prevention of VTE in 407 Japanese patients undergoing total knee arthroplasty. 34 Patients were randomly assigned to receive 110, 150, or 220 mg of dabigatran etexilate or placebo once daily for 11 to 14 days, starting the day after surgery (at least two hours after removing the indwelling catheter and confirming the absence of abnormal bleeding from the drainage sites). The primary efficacy end point was the incidence of total VTE and all-cause mortality; the primary safety end point was incidence of major, clinically relevant, and minor bleeding events. Total VTE and all-cause mortality were lower in patients receiving dabigatran etexilate 110, 150 or 220 mg daily (39.6%, 32.7%, and 24.0%) than placebo (56.4%) (P < 0.05 for all comparisons). There was no difference in the incidence of major bleeding among all groups (1 vs. 0 vs. 3 vs. 0.8% for dabigatran etexilate 110, 150, 220 mg and placebo respectively). The investigators concluded that the dabigatran etexilate reduced incidence of VTE in Japanese patients undergoing total knee replacement, with comparable safety profile to placebo.
For the prophylaxis of VTE, initially dabigatran etexilate 12.5–300 mg orally twice daily was proposed for patients undergoing total hip replacement. 24 This was narrowed to a total daily dabigatran etexilate dose of 100–300 mg orally, which demonstrated significantly fewer VTE in patients who had undergone total hip or total knee replacement, compared with enoxaparin. 25 Studies of larger populations demonstrated non-inferiority of dabigatran etexilate 220 and 150 mg once daily compared with enoxaparin 40 mg daily subcutaneously in patients undergoing total hip or total knee replacement, without significant increases in major or minor bleeding event.26,27 In contrary, dabigatran etexilate has failed to achieve non-inferiority in patients undergoing total knee replacement when enoxaparin was administered as 30 mg subcutaneously twice daily. 28 The authors attributed them to an increased frequency of asymptomatic distal DVT and perhaps the use of higher total daily doses of enoxparin.
Treatment of venous thromboembolism
The dabigatran versus warfarin in the treatment of acute VTE (RECOVER) study is the only randomized, double-blinded, non-inferiority trial evaluating dabigatran etexilate for VTE treatment published to-date. Two thousand three hundred and thirty-nine patients with acute VTE who have been treated with parenteral anticoagulation therapy for a median of nine days were randomized to receive either dabigatran etexilate 150 mg orally twice daily or warfarin that was dose-adjusted to achieve an INR of 2 to 3. 35 The primary outcome was the 6-month incidence of recurrent symptomatic, objectively confirmed VTE and related deaths. Safety end points included bleeding events, acute coronary syndromes, other adverse events, and abnormal results of liver-function tests. The primary outcome occurred in 30 of the 1274 patients receiving dabigatran (2.4%), as compared with 27 of the 1265 patients randomly assigned to warfarin (2.1%). The difference in risk was 0.4% (95% confidence interval [CI], −0.8 to 1.5; P < 0.001 for the pre-specified non-inferiority margin). Major bleeding episodes occurred in 20 patients assigned to dabigatran (1.6%) and in 24 patients assigned to warfarin (1.9%) (Hazard ratio with dabigatran, 0.82; 95% CI, 0.45 to 1.48), and episodes of any bleeding were observed in 205 patients assigned to dabigatran (16.1%) and 277 patients assigned to warfarin (21.9%; hazard ratio with dabigatran, 0.71; 95% CI, 0.59 to 0.85). The numbers of, acute coronary syndromes (dabigatran 0.4%, warfarin 0.2%, P = 0.73), and abnormal liver-function tests (AST elevation: dabigatran 3.1%, warfarin 2.1%, P = 0.14) were similar in the two groups. Adverse events leading to discontinuation of the study drug occurred in 9.0% of patients assigned to dabigatran and in 6.8% of patients assigned to warfarin (P = 0.05). The investigators concluded that fixed dose of dabigatran is as effective as warfarin, has a safety profile that is similar to that of warfarin for VTE treatment.
Dosage and Administration
Dabigatran etexilate is currently approved in Europe and Canada for prevention of VTE. The drug has not yet been officially approved for treatment of VTE. The recommended dosage of dabigatran etexilate for prevention of VTE in patients following knee replacement surgery is 220 mg once daily (taken as two capsules of 110 mg). Treatment should be initiated within 1–4 hours of completed surgery with 110 mg and continues with 220 mg once daily thereafter for a total of ten days. 36 For prevention of VTE in patients following elective hip replacement surgery, the recommended dose of dabigatran etexilate is also 220 mg taken orally once daily. Similarly, treatment should be initiated orally within 1–4 hours of completed surgery with 110 mg and continuing with 220 mg once daily therefore but for a total of 28–35 days. 36 For both types of surgery, if hemostasis cannot be secured within the first day after surgery, then treatment with dabigatran etexilate should be delayed. If treatment is initiated beyond the first day of surgery, then the starting dose should be 220 mg orally once daily. Based on the results of RECOVER, 35 the treatment doses for VTE would be dabigatran 150 mg twice daily.
According to the European dabigatran etexilate prescribing information, treatment with dabigatran etexilate in patients with creatinine clearance <30 mL/min for VTE treatment or prevention is contraindicated given there is no data to support its use in that population. And for patients with creatinine clearance of 30–50 mL/min, the recommended dose is 75 mg given 1–4 hours after surgery, and 150 mg daily starting the next day. 36 Although, according to the US prescribing information, where dabigatran etexilate is approved for use in preventing stroke from atrial fibrillation only, the dosage of dabigatran etexilate in patients with creatinine clearance 15–30 mL/min is 75 mg twice daily (not recommended for patients with creatinine clearance <15 mL/min) and no dosage adjustment is necessary for creatinine clearance of 30–50 mL/min (150 mg twice daily). 37 According to the European dabigatran etexilate prescribing information, in patients >75 years of age, the recommended dose is similar to those with creatinine clearance of 30–50 mL/min (ie, 75 mg given 1–4 hours after surgery, and 150 mg daily starting the next day). 36 Dabigatran etexilate is not recommended for patients with elevated liver enzymes >2 times upper limit of normal.
Based on drug interaction data discussed previously, the use of dabigatran etexilate with P-glycoprotein inducer such as rifampin should be avoided. Dosage adjustment is not required when dabigatran etexilate is used with P-glycoprotein inhibitors ketoconazole, verapamil, amiodarone, quinidine and clarithromycin.
In patients undergoing major orthopedic surgery, the use of dabigatran etexilate is not recommended in patients undergoing anesthesia with post-operative indwelling epidural catheters. Administration of the first dose of dabigatran etexilate should occur at a minimum of two hours after the catheter is removed.
If patients are to be converted from warfarin to dabigatran etexilate (in the case of VTE treatment), the US prescribing information recommended discontinuation of warfarin and initiate dabigatran etexilate when the INR is <2. 37 When converting dabigatran etexilate to warfarin, the starting time of warfarin should be based on patients’ creatinine clearance. For patients whose creatinine clearance is >50 mL/min, warfarin should be used for three days before discontinuing dabigatran etexilate. For those with creatinine 31–50 mL/mine, warfarin should be used for two days before discontinuing dabigatran etexilate. For those with creatinine clearance 14–30 mL/min, warfarin should be used for one day before discontinuing dabigatran etexilate. No recommendation was made for patients with creatinine clearance <15 mL/min because dabigatran etexilate is contraindicated in this situation. 37
Pharmacoeconomics
Dabigatran etexilate offers a new oral anticoagulant alternative to warfarin, which offers the convenience of no regular laboratory monitoring for dosage adjustment and minimal drug and food interaction. With the increase in economic burden of VTE, pharmacoeconomic analysis may aid to determine if newer anticoagulants promise more convenient and safe antithrombotic therapy with increased compliance.
Woloacz et al evaluated the cost-effectiveness of oral dabigatran etexilate compared with subcutaneous enoxaparin for the prevention of VTE after total knee replacement and total hip replacement from the perspective of the United Kingdom (UK) National Health Service. 38 Dabigatran etexilate (220 mg orally once daily) was compared with enoxaparin (40 mg once daily) in patients undergoing total knee replacement (duration of prophylaxis, 6–10 days) and total hip replacement (duration of prophylaxis, 28–35 days). The 10-week acute postsurgical phase was modeled using a decision tree. A Markov process (1-year cycle length) was used to model long-term events (recurrent VTE, post-thrombotic syndrome, and consequences of intracranial hemorrhage) for patients’ remaining lifetimes. The probabilities of long-term events were estimated using data from published longitudinal studies. Rates of VTE and bleeding events did not differ significantly between dabigatran etexilate and enoxaparin. Dabigatran etexilate was less costly than enoxaparin in total knee replacement and substantially less costly in total hip replacement, primarily due to differences in administration costs. The cost of prophylaxis for total hip replacement patients, including drugs and administration costs, was estimated at 137 pounds for dabigatran etexilate and 237 pounds for enoxaparin for the duration of treatment. At a willingness-to-pay threshold of 20,000 pounds per quality-adjusted life-year (QALY), the probability of cost-effectiveness for dabigatran etexilate was 75% in total knee replacement and 97% in total hip replacement. These results were robust across a range of sensitivity analyses. The authors concluded that from the perspective of the UK National Health Service, thromboprophylaxis with dabigatran etexilate was cost-saving compared with enoxaparin 40 mg once daily, with comparable efficacy and safety profiles.
The same group of investigators (Wolowacz et al) performed another similar pharmacoeconomics analyses of oral dabigatran etexilate 150 mg once daily, used in patients over the age of 75 years, 39 from a UK National Health Service perspective. Dabigatran etexilate was compared with subcutaneous enoxaparin 40 mg daily, using a decision model. Dabigatran etexilate was demonstrated to be less costly than enoxaparin; cost savings varied from 62 pound to 274 pound (base-case analyses) and were primarily due to differences in administration costs. Results were robust across a range of sensitivity analyses.
McCullagh et al evaluated the cost effectiveness of both rivaroxaban, an oral anti-Xa inhibitor and dabigatran etexilate compared with enoxaparin for the prophylaxis of VTE in patients undergoing elective total hip and total knee replacement in the Irish healthcare setting. 40 The evaluation was conducted from the Irish health-payer perspective. A static decision-tree model was developed with a 180-day post-surgery time horizon. Outcome measures were QALYs and life-years gained (LYG). Costs were valued in euro, year 2008 values. One-way sensitivity analysis of all probabilities in the model was performed. A probabilistic sensitivity analysis using second-order Monte Carlo simulation was performed to determine the probability of cost effectiveness at euro 45,000 per QALY threshold. In the total hip replacement base-case model, rivaroxaban dominated both dabigatran etexilate and enoxaparin sodium. The incremental cost-effectiveness ratios for dabigatran etexilate relative to enoxaparin were euro 23,934 per LYG and euro 17,835 per QALY. In the total knee replacement base-case model, rivaroxaban dominated both dabigatran etexilate and enoxaparin sodium. Dabigatran etexilate also dominated enoxaparin sodium. At a cost-effectiveness threshold of euro 45,000 per QALY, the probability that rivaroxaban was the most cost-effective strategy after total hip replacement was 39%, followed by dabigatran etexilate at 32% and enoxaparin sodium at 29%. The probability that rivaroxaban was the most cost-effective strategy after total knee replacement was 46%, followed by dabigatran etexilate at 30% and enoxaparin sodium at 24%. Base-case analysis indicates that when both rivaroxaban and dabigatran etexilate are compared with enoxaparin, rivaroxaban is the less costly and more effective option after total hip replacement and total knee replacement. Probabilistic sensitivity analysis indicates that rivaroxaban is the most cost-effective strategy at a cost-effectiveness threshold of euro 45,000 per QALY; however, there is uncertainty regarding this strategy being more cost effective than dabigatran etexilate when both are compared with enoxaparin sodium.
Pharmacoeconomics analysis of dabigatran etexilate in the US Healthcare setting has not been performed to-date.
Reversibility of Anticoagulant Effect of Dabigatran
There is currently no-antidote for direct thrombin inhibitors including dabigatran. In certain clinical situations such as serious bleeding into critical organs, potential overdose and emergency surgery, clinicians will need to make an assessment of the anticoagulant status of a patient receiving dabigatran before deciding on future management strategies. Measurements of TT or ECT are recommended to evaluate the anticoagulant effect of dabigatran. 41 The activated partial thomboplastin time can provide useful qualitative assessment of anticoagulant activity but is less sensitive at supratherapeutic dabigatran serumconcentrations. 41 However, aPTT may be the most accessible test to determine the presence or absence of anticoagulant effect.
In patients who require temporary discontinuation of dabigatran due to surgery, the manufacturer has recommended that in patients with creatinine clearance of >50 mL/min, dabigatran etexilate be stopped at least 24 hours prior to surgery, for those with creatinine clearance between 30–50 mL/min, the drug be stopped at least 48 hours prior to surgery and for those with creatinine clearance <30 mL/min, the drug be stopped 2–5 days prior to surgery. 41
In case of overdose, since dabigatran etexilate is a lipophilic molecule, adsorption by activated charcoal is expected and has been demonstrated in in vitro but not in vivo study. 41 In the event of bleeding complication, management should be individualized according to the severity and location of the hemorrhage. Treatment should be discontinued and the source of bleeding investigated. As dabigatran predominantly undergoes renal excretion, maintenance of adequate diuresis is essential. Delaying administration of the next dose or discontinuation of dabigatran etexilate therapy, mechanical compression, surgical hemostasis and transfusion of blood products should be performed as needed. In patients with normal renal function, plasma concentration levels should decline relatively quickly following discontinuation of the drug (~12 hours). 41 If all of the above measures fail to control bleeding, the use of hemodialysis to increase rate of dabigatran elimination can be considered. 39
Discussion and Future Perspectives
Prior to dabigatran, vitamin K antagonist warfarin remained the only available oral anticoagulant. Dabigatran appears to offer benefits over warfarin in terms of having less inter-patient variability in dose response, not requiring routine anticoagulation monitoring, less drug-food and drug-drug interactions, and faster dose titration process. Completed trials offer insight into the efficacy and safety of dabigatran etexilate for VTE prophylaxis in high-risk patients undergoing total knee or hip replacement, as well as treatment for patients who developed DVT and PE. For VTE prophylaxis, dabigatran etexilate has demonstrated either superiority or non-inferiority to enoxaparin in most studies.24–27 However, the REMOBILIZE study failed to demonstrate non-inferiority to enoxaparin dosed twice daily in the composite end point of proximal DVT, distal DVT, PE, and all cause mortality. 28 The two non-inferiority studies have different non-inferiority margin were used in RENOVATE and REMODEL (7.7% and 9.2% respectively).26.27 This may introduce disparity when analyzing the results. Both of these studies also have relatively low occurrence of primary events compared to historical studies of VTE prophylaxis in this patient population, which may also have affected outcomes.26,27 The dosage and timing of initiation of enoxaparin in the REMODEL trial is also a question. 27 In that study, enoxaparin 40 mg once daily was permitted to be started after surgery, which is not an FDA-approved regimen in the US. This regimen may have reduced the efficacy of enoxaparin and also the frequency of bleeding events. Also in the REMODEL study, a 40 mg dose of enoxaparin was studied in patients undergoing total knee replacement, whereas the US enoxaparin dose at 30 mg twice daily is preferred in these high-risk patients. Additional data comparing dabigatran etexilate with the recommended dose of enoxaparin 30 mg twice daily in patients undergoing total knee replacement surgery is needed.
The generalizability of the completed trials must also be addressed. All of the VTE prophylaxis trials used enoxaparin as the comparator. Fondaparinux is another anticoagulant that is indicated for VTE prophylaxis. When compared with enoxaparin, fondaparinux has demonstrated a 55.2% relative risk reduction (P < 0.001) in symptomatic and venographic VTE in patients undergoing total hip and knee replacement. 42 Therefore, additional data comparing dabigatran etexilate with fondaparinux is warranted.
Due to past experience with ximelagatran, there should be more monitoring for liver injury and ACS in long-term studies. 43 The REMEDY (Secondary Prevention of venous thromboembolism) study currently recruiting will focus on the efficacy of dabigatran etexilate compared with warfarin in patients with recurrent VTE who had received previous treatment with warfarin. 44
Finally when considering clinical application of new agents, pharmacoeceonomics must be addressed. There is no pharmacoeconomic analysis of dabigatran etexilate from a US societal perspective. Pharmacoeconomic analysis performed in the UK and Ireland demonstrated that dabigatran etexilate can be cost saving as compared to enoxaparin. Dabigatran etexilate has been recently approved by the US and the average wholesale price of the 150 mg capsule is $6.75 (as compared to warfarin at a cost of ~$0.40 daily). 45 The 220 mg formulation (dose used for VTE in patients with normal renal function) is not available in the US.
Conclusions
Dabigatran etexilate is an oral direct thrombin inhibitor that has demonstrated comparable safety and efficacy to enoxaparin for VTE prophylaxis in patients undergoing orthopedic surgery, as well as comparable safety and efficacy to warfarin for VTE treatment. The ease of oral administration, no need for routine coagulation monitoring and lack of significant drug interactions, along with rapid onset and predictable pharmcaodynamics, favor the use of dabigatran etexilate over warfarin and parenteral anticoagulants. Further data from ongoing long-term studies evaluating treatment of VTE and other indications are needed to confirm its efficacy and long-term side effects, especially potentials for liver toxicity and development of ACS events.
Footnotes
Disclosures
This manuscript has been read and approved by the author. This paper is unique and not under consideration by any other publication and has not been published elsewhere. The author reported no conflicts of interest. The author confirmed that they have permission to reproduce any copyrighted material.