
Abstract
The drug Levodopa (LD) is an efficient compound for the treatment of patients with Parkinson's disease (PD). Its short half life generates plasma behaviour of LD with peaks and troughs. Therefore, following the LD transport into the brain and the conversion to dopamine, an alternating stimulation of nigrostriatal postsynaptic dopamine receptors takes place. In the long term these fluctuations of dopamine concentrations supports onset of motor complications (MC) in PD patients. General opinion is that loss of central compensatory mechanisms of dopamine metabolism is responsible for the development of MC. However, in the periphery, LD troughs are preponderantly associated with the MC wearing off, which is the reappearance of motor symptoms with decreasing drug effect. Addition of the catechol-O-methyltransferase (COMT) inhibitor Entacapone (EN) to LD/carbidopa (CD) improved wearing off, since EN prolongs LD half life and avoids troughs. Plasma LD peaks are mostly related to the clinical manifestation of the MC dyskinesia, which appear as involuntary movements. One time addition of EN to a LD/CD formulation showed no increase of peripheral maximum LD concentration. But repeat combination of EN to each LD/CD intake elevated plasma LD bioavailability and peaks. Therefore switch from a LD/CD–-to a LD/CD/EN regime may also ask for reduction of LD/CD dosing or delay of the next LD/CD intake, to avoid onset of the most common peak dose dyskinesia. In conclusion, pharmacokinetic studies on peripheral LD metabolism and mode of intake underline their importance as peripheral components for MC manifestations in PD patients.
Introduction
Parkinson's disease (PD) is one of the most worldwide spread, chronic neurodegenerative disorders of the elderly. Several studies have sought to define the incidence of PD. Reported standardised incidence rates of PD are 8–18 per 100,000 person-years. PD may occur before the age of 50 and may account for around 10% of the 1.5 million people with the disease. A sharp increase in incidence is seen after the age of 60. 1 Although PD per se is not a direct cause of death, death may occur as a secondary result of severe motor dysfunction, e.g. falls in advanced PD. Despite the differences in methodology, the results of most epidemiological studies consistently suggest that PD reduces life expectancy. In more recent years, there seems to be a reduced mortality from PD owing to the use of more effective therapies.2–5
Response of Motor Features of PD by Levodopa (LD)
James Parkinson's original description of PD characterised slowly deteriorating motor function as the essential clinical characteristic symptom beside an array of further more secondary clinical signs. Slowly ongoing loss of nigral dopaminergic presynaptic neurons causes occurrence of bradykinesia, rigidity and to a lesser extent tremor, all of which results from a reduction of about 70%–80% striatal dopamine in combination with a less distinct altered transmission of further neurotransmitters. This dopamine deficit in the basal ganglia inaugurated the therapeutic concept of dopaminergic substitution. Nearly all motor symptoms respond to application of the blood brain barrier trespassing precursor of dopamine, LD, in clinical practice (LD).6–10 Objectives of this review are (I) to discuss available modes of oral LD administration in the treatment concepts for PD patients, (II) to investigate the role of peripheral LD metabolism on the generation of motor complications (MC) and (III) to highlight the role of COMT inhibition by entacapone (EN) as therapy and putative cause for various subtypes of MC.
Basic Principles of LD Administration
The introduction of LD was a milestone in the treatment of PD. Initially LD was administered as an infusion, then in oral form without inhibition of LD degrading enzymes (Fig. 1A). Oral LD application was later combined with dopadecarboxylase inhibitors (DDI).6,7 This pharmacological principle of enzymatic inhibition of LD metabolism reduces the peripheral degradation of LD to dopamine. Therefore, plasma half life of LD increases, which results in a better efficacy of the compound (Fig. 1B). DDI such as Benserazide (BE) and Carbidopa (CD) do not cross the blood-brain barrier. Addition of DDI to LD allows for a four- to fivefold oral LD dose reduction. As a result, the frequency of LD-related peripheral side effects, i.e. nausea and vomiting, lowers. 8 LD absorption and efficacy can be delayed or diminished by amino acids in protein meals, since they may interact with the active large amino acid transporter of the gastrointestinal tract and of the blood brain barrier.11,12
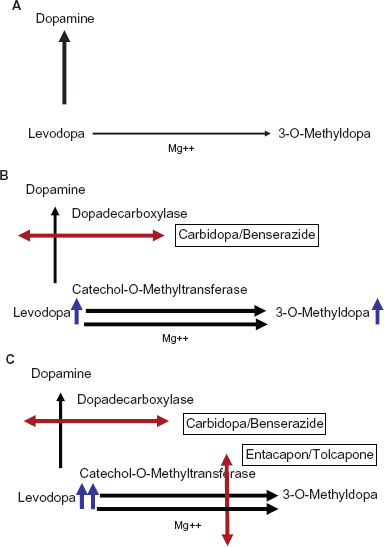
Modes of LD metabolism without (1A) and with (1B, 1C) inhibition of LD degrading enzymes.
Supplementation of LD/DDI application with inhibitors of catechol-O-methyltransferase (COMT)
Inhibition of LD degradation by combination with a DDI supports LD metabolism via the enzyme COMT (Fig. 1B). As a result, an increased synthesis of the LD metabolite 3-O-methyldopa (3-OMD) occurs. Blocking of COMT activity further reduces peripheral LD degradation, as it prolongs plasma half life of LD and elevates delivery of LD to the brain. Moreover the peripheral LD degradation to 3-OMD is reduced. Experimental and clinical outcomes confirmed the efficacy of this therapeutic principle with peripheral dual inhibition of both main LD metabolizing enzymes (Fig. 1C).13–16
Clinical effects of oral LD/DDI application in the treatment of PD patients
The introduction of oral LD/DDI treatment was a breakthrough in the drug treatment of PD. However, a debate was soon started on the saga of LD neurotoxicity based on the clinical observation of fluctuations of movement as long term consequence of LD/DDI treatment and outcomes of experimental animal–- and cell culture studies. 17 As consequence, the Earlier vs. Later L-DOPA (ELLDOPA) trial was designed to answer whether LD is harmful or not. 18 There were many investigations, which demonstrated the clinical efficacy of LD. However the ELLDOPA trial was one of the first double blind trials, which compared the therapeutic efficacy of LD/CD in three different daily dosages of 150 mg, 300 mg or 600 mg with placebo treatment according to the guidelines of good clinical practice in PD patients. Additionally functional brain imaging with the [123J]-β-CIT-SPECT was employed as biomarker to evaluate the integrity of the nigrostriatal system during LD treatment and to demonstrate a PD accelerating effect of LD. The ELLDOPA trial produced conflicting results. Treatment with LD/DDI was associated with a significant increase in declining rates of [123J]-β-CIT imaging marker uptake over nine months compared with placebo, a finding consistent with a toxic effect of higher LD dosages. Clinical evaluation, however, showed that patients on LD/DDI treatment had better Unified Parkinson's Disease Rating Scale (UPDRS) scores compared with placebo administration after two weeks of washout. This would, in contrast, be indicative of a protective, benign PD modifying effect of LD. However, intellectual parsimony would dictate that the simplest explanation for this clinical effect is that the washout period was too brief to eliminate the symptomatic benefits of LD despite the short plasma half life of the drug. 18 An alternative hypothetical explanation of this outcome may be that LD maintained body function and prevented onset of secondary long term changes and adaptation occurring after the manifestation of PD. This consideration may allow the more general conclusion that the clinical results of the ELLDOPA trial also support the concept of an early as possible diagnosis of PD with subsequent immediate initiation of treatment similar to conclusions, which may drawn from the positive outcomes of studies on the efficacy of antiparkinsonian drug rasagiline in early PD patients with a delayed start design. These trial results may also indicate that PD patients with a more earlier treatment performed better than the ones with a delayed start.18,19
Reasons for delayed LD/DDI treatment initiation in PD patients
Current guidelines suggest delay of LD use in PD patients as long as possible. Particularly, if one may assume a further long lasting necessary treatment of PD due to a relative young biological age. Avoidance of LD implementation is known to postpone onset of motor complications (MC). This is of outstanding importance for PD patients with an early onset of the disease or young biological age, since MC limit quality of life and cause caregiver burden considerably.20–23
Causes for the Onset of MC
MC are fluctuations of movement behaviour dependent, which is called predictable, respectively independent, which is classified as unpredictable, on previous dopaminergic drug intake. MC are looked upon as a clinical milestone, which indicates an advanced stage of PD. MC are predominantly associated with oral LD/DDI treatment due to the short plasma half life of LD. Accordingly peaks and troughs of LD plasma levels appear. Following the LD transport into the brain and the conversion to dopamine in presynaptic neurons, fluctuations of dopamine brain concentrations generate MC by irregular, not continuous stimulation of nigrostriatal postsynaptic dopamine receptors. Loss of presynaptic dopaminergic autoreceptor function and other compensating abilities to avoid not physiologic high dopamine concentrations in the synaptic cleft are currently looked upon as the main central cause for MC appearance. Onset of MC is predominantly looked upon as the clinical consequence of the induction of frequent alternating postsynaptic dopamine receptor stimulation with further downstream intracellular changes in neuronal nigrostriatal cells, which regulate motor behaviour. Continuous stimulation of these postsynaptic dopamine uptake sites may delay onset of MC, which often appear in combination with a wide array of non motor symptoms.20,24–26 Peripheral components of drug intake, like compliance, which is a problem in many PD patients, or absorption of the applied compound often in combination with other drugs may also influence the occurrence of MC.27–31
Consequences of MC in clinical practice
Generally, intervals and intensity of MC may differ from day to day. They may be brief or long, lasting between several minutes or hours. These fluctuations of movement behavior cause patient disability, embarrassment, frustration.20,24,32,33 The ELLDOPA trial confirmed the view, that the higher the daily administered LD dose was, the more frequent MC were observed. Their occurrence rate was equal to placebo in the 150 mg daily LD dose treated cohort, but rose up to 3-fold in the 600 mg daily dose treated group. 18 Therefore generally, fear of MC limits the long term value and the patients’ acceptance of LD/DDI intake. As an alternative, dopamine agonists (DA) were developed and launched.
Preventive strategies of MC DA and MC
Unlike LD, DA act directly on postsynaptic dopamine receptors without the need for metabolic conversion to dopamine, storage and release in degenerating nigrostriatal nerve terminals. In addition, DA decrease endogenous dopamine turnover, which is enhanced by LD and is a potential source of increased synthesis of neurotoxic free radials attributable to oxidation of accumulating dopamine. However, DA are less tolerated compared with LD, but they postpone MC onset due to their longer plasma half life and–-at least partially–-a higher affinity to postsynaptic dopamine uptake sites. Common peripheral side effects of all DA include nausea, vomiting, postural hypotension, dizziness, bradycardia and other effects related to stimulation of the peripheral autonomic system. Co-administration of the peripheral dopamine-receptor blocker domperidone (off-label use, i.e. in the USA) can be used to counteract these symptoms.9,10,34 One assumes that the more recent launch of retarded release DA will further reduce the number of PD patients suffering from MC, since the retarded release formulations will further minimise alternating DA levels in the periphery and in the brain. Moreover these compounds showed a better tolerability and efficacy on additional non motor symptoms, i.e. sleep, in clinical trials.35–37 In daily practice, their handling and thus their efficacy is also better, since patients are asked to take the drug one time daily only, which improves compliance. But it is known that MC may also even occur with long-term DA use only, but far more rarely compared with intake of LD/DDI formulations.35,36
Monoaminooxidase B (MAO-B) inhibition and MC
To stabilise respectively to decrease metabolism of dopamine in the synaptic cleft of nigrostriatal neurons with predominant glial MAO-B inhibition is a further therapeutic concept for dopaminergic substitution in PD patients. Two compounds of the propargylamine group, selegiline and rasagiline, both irreversible MAO-B inhibitors, have demonstrated a symptomatic effect in PD patients. 38 MAO-B-inhibition catalyses the oxidative deamination of active amines and therefore causes prolonged dopamine activity. Selegiline and rasagiline are relative specific inhibitors of MAO-B activity. However this selectivity gets lost at higher drug doses, i.e. selegiline >20 mg/day and rasagiline >2 mg/day. These dosages also inhibit MAO-A, which converts other amines, like norepinephrine. Therefore, although low, there is a risk of tyramine-induced hypertension, which is called the “cheese effect”, at higher doses by these agents. These compounds are also known to enhance the activity of catecholaminergic neurons by mechanisms other than MAO-B inhibition. 39 Other pharmacological activities such as effect on mitochondrial membrane potential activity, anti-apoptotic and antioxidant efficacy may explain potential neuroprotective mechanisms seen in the laboratory. Correspondingly, clinical trials investigated this putative benign influence on the course of PD. 39 One of them was the DATATOP study, a prospective, randomised, double-blind, placebo-controlled study that included 800 patients with PD. After randomisation to either selegiline, α-tocopherol (vitamin E), a combination of both or placebo, the patients were followed up with no other treatment until clinical deterioration calling for initiation of symptomatic LD therapy as clinical endpoint. Selegiline, but not α-tocopherol, resulted in a significant delay for LD/DDI requirement compared with placebo (26 versus 15 months; p < 0.0001). However, this beneficial effect of selegiline vanished in the further follow-up investigations of the trial. The main limitation of this study after careful analysis was the potential confounding symptomatic effect of selegiline on the results. Moreover the endpoint of this trial–-the need for LD therapy–-is under debate.40,41 Further trials examined the disease modifying potential of rasagiline.39,42–44 Both double-blind, parallel group, randomised, delayed-start clinical studies included early PD patients. They were randomised to receive rasagiline 1 or 2 mg/day or placebo for a certain period, followed by rasagiline application in general. The relative weak degree of motor improvement was comparable to that seen for selegiline in the DATATOP study, but not as great as that observed for the dopamine agonists. In addition, patients who received 1 mg rasagiline during the whole study interval had less functional decline, as assessed by the Unified Parkinson's Disease Rating Scale (UPDRS), than patients who received placebo initially for a certain period.19,45,46 These results support a disease modifying effect of the drug, which will consequently delay occurrence of MC further. Additionally rasagiline was also shown effective for the symptomatic treatment of MC. 47 Nevertheless all these compounds for dopamine modulation or–-substitution improve motor behaviour only to a certain extent. Therefore the introduction of LD/DDI is a necessity at a certain moment, which is looked upon as an essential milestone in each life of a PD patient.
LD/DDI treatment and MC in PD patients
Initially LD is well tolerated and provides no MC. This is called the honeymoon period of LD therapy, followed by the insidious onset of MC and associated non motor features, when the drug efficacy vanes. Therefore pharmacologic strategies were necessary to prolong the half life of LD, as a more continuous LD delivery to the brain helps to prevent and improve predominantly LD/DDI associated MC. 10 The efficacy of this concept and the importance of not fluctuating LD brain delivery was convincingly shown by duodenal LD infusion systems, as PD patients suffering from severe MC experienced an enormous deterioration of the intensity and frequency of MC due to the stable LD plasma concentrations.48,49 But performance of duodenal LD infusions is a rather complex and an expensive technique with a considerable demand for caregiver burden.
Preventive strategies for MC onset by oral LD application
Earlier, LD/DDI application with oral slow release formulations were developed and tested as an alternative to provide more constant LD plasma behaviour. Clinical studies showed a reduced efficacy of these retarded release LD/CD formulations in comparison with conventional LD/CD tablets, when the same oral LD dosage was administered. Moreover they did not delay onset of MC. However one must consider that these trials did not evaluate MC with too much detail.50,51 Nevertheless an unmet need was to establish further, alternative strategies of oral LD application to prolong peripheral half life of LD. Therefore COMT inhibitors, i.e. EN, were introduced.
Clinical Efficacy of COMT-inhibition in Combination with LD/DDI
Numerous phase II, III and IV trials demonstrated that COMT-inhibition with EN or tolcapone given as extra tablet improves efficacy of LD/DDI [examples given:52–54]. A more recent and important trial on the efficacy of COMT inhibition with EN was the FIRST-STEP (Favorability of Immediate-Release Levodopa/Carbidopa vs. STalevo Short-Term comparison in Early Parkinson's disease) study. It aimed to compare the efficacy of these two different modes of LD application, the conventional LD/CD administration versus LD/CD with the COMT-inhibitor EN in one tablet (LD/CD/EN) in early PD patients with a need for LD therapy. This multicenter, double-blind, randomized, parallel-group study administered a fixed oral LD dose of 300 mg/day, distributed as 100 mg LD doses three-times daily at 5-hour intervals to 424 PD patients. In this 39 weeks lasting study, the PD patients in the LD/CD/EN arm performed significant better than the ones in the LD/CD treated cohort after week four throughout the remaining course of the study. This was found when the sum scores of the UPDRS part II (activities of daily living) and UPDRS part III (motor examination) were compared as main primary outcome at the remaining study visits. The statistical analysis investigated the intention to treat population and employed the last observation carried forward procedure. The FIRST-STEP trial demonstrated that LD/CD was inferior to LD/CD/EN treatment. 55 Thus it confirmed the known additional LD/DDI efficacy enhancing effects of EN, when given as extra tablet, to an existing LD/CD regimen in treated PD patients, which was proven by pharmacokinetic investigations before.15,16,53,54,56–60
Safety and tolerability
Phase III studies and post marketing surveillance showed the safety, tolerability and efficacy of LD/DDI combination with EN even with co-administration of selegiline, dopamine agonists and antidepressants like i.e. imipramine. The most common observed side effect was harmless discoloration of the urine. A further non dopaminergic adverse event of COMT inhibition is diarrhoea sometimes occurring even up to two to four months following treatment initiation. This may be due to the inhibition of 5-HT metabolism in the gastrointestinal tract, which causes an increase of gastrointestinal motility in some PD patients. 61 Centrally acting, stronger direct EN competitor tolcapone was temporarily withdrawn due to reports on serious hepatic reactions with development of severe, sometimes even fatal, hepatic disease as well as possible occurrence of rhabdomyolysis and neuroleptic malignant-like syndrome. Nowadays one assumes that patients with mutations in the UDP-glucuronos-yltransferase 1A9 gene, which leads to defective glucuronidation activity, may predispose for tolcapone induced hepatotoxicity. 61
Regulatory affairs
The discussion on the liver toxicity of tolcapone with a demand for liver function tests on regular basis still bias the preference for EN intake. An additional negative criterion for tolcapone use is the need for a previous failed response or intolerance of EN intake. 61 However tolcapone therapy asked for the additional intake of three tablets to a consisting LD/DDI regime only. EN, given as an extra tablet, should be combined with every LD/DDI intake with an upper limit of a daily dose of 1600 mg EN. This may increase the number of tablets and reduce compliance. This disadvantage of EN therapy was improved with the introduction of the triple combination LD/CD/EN.33,62
LD/CD/EN in one tablet
More advanced PD patients must often take LD/DDI doses sometimes up to every two hours. This LD “fractionation” reduces temporary loss of efficacy, which is associated with reappearance of motor symptoms. The LD/CD/EN introduction was an essential step forward in contrast to the older LD/DDI plus EN administration as extra tablet, since in addition to the reduction of tablet intake, the LD/CD/EN pill size was distinct smaller. This further eased swallowing and favoured patients’ acceptance. 33 The unmet need of LD therapy, treatment or even prevention of MC or an subtype of MC, the wearing phenomenon, was still of importance.
Wearing off
PD patients tend to experience fluctuations of movement with progression of the disease. They switch from ON to OFF and vice versa. The ON state is characterised by good movement behaviour. OFF is associated with temporary onset of the cardinal motor symptoms. When this reappearance of motor symptoms indicates the decreasing efficacy of the last dopaminergic drug intake before the next one, they are described as wearing-off.20,24
EN and the treatment of wearing off
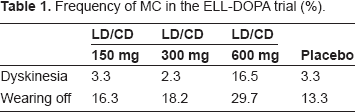
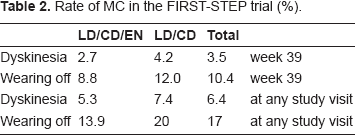
Both studies, FIRST-STEP and ELLDOPA, provided also some interesting findings regarding the onset and frequency of wearing off in PD patients (Tables 1 and 2). In the FIRST-STEP trial, the number of monitored wearing off was higher in the LD/CD–-compared with the LD/CD/EN treated PD patients (Table 2). The frequency of noted wearing off phenomena was rather low in relation to the size of the study population and the short observation interval. Therefore this did not turn out as statistical relevant in the investigated early PD patients, who were probably in the honeymoon period of LD application with good tolerability and efficacy. This may indicate that EN prevents onset of wearing off. 55 In the ELLDOPA trial, the number of observed wearing off increased with higher LD/CD dosing (Table 1). Therefore one may assume that EN in combination with LD/CD not only improves but also may prevent onset of wearing off phenomena. Accordingly, pharmacokinetic studies showed that EN supplementation to LD/CD avoids troughs, elevates half life of LD and thus contributes to more stable plasma levels after twice administration every three hours.14,15 The prolongation of plasmatic LD half life was even shown after one time application. All these outcomes contribute to prevent and to improve wearing off phenomena. 63 The latter feature was the reason for approval of EN, but the value of EN supplementation to LD/CD in the treatment or prevention of other kinds of MC such as dyskinesia still remained unsolved.
Frequency of MC in the ELL-DOPA trial (%).
Rate of MC in the FIRST-STEP trial (%).
Dyskinesia
Unwanted, abnormal involuntary movements are termed as dyskinesia. They develop as a complication of dopaminergic stimulation. Dyskinesia can occur during both ON and OFF intervals. Classification of dyskinesia is generally performed in relation to the timing of LD dosing. ON dyskinesia appears either during the period when patients are obtaining maximal relief from their motor symptoms. Then they are looked as peak-dose dyskinesia.20,24 They may be also biphasic, occurring soon after LD is taken and as the patient is beginning to turn ON and again when the LD effect is wearing off and the patient is beginning to turn OFF. They are mostly absent when the LD dose is having its maximal effect. The maximum plasma LD level following intake may cause peak-dose dyskinesia as the most common form of these kind of involuntary movement behaviour. As the disease progresses, patients may develop dyskinesia throughout the whole ON time. In a study of 168 PD patients with dyskinesia, 50% experienced only one type of dyskinesia (ON period, diphasic or OFF dyskinesia), 40% experienced two types, while 10% of patients experienced all three types of dyskinesia. Generally advanced PD patients better tolerate on intervals with mild dyskinesia than OFF periods. The risk of developing dyskinesia has been associated with a number of clinical factors. The severity of PD, the dosage and duration of LD therapy, and a younger age of the PD patient are currently believed to be among the variables that best predict the development of dyskinesia. Analysis of multiple clinical data sets has allowed an assessment of the frequency of dyskinesia in patients with PD since the advent of LD in the late 1960s. The main finding was that among modern era patients, who were diagnosed with PD since LD has been available as treatment, the median dyskinesia frequency was approximately 40% after 4-6 years of LD therapy. In contrast, patients who developed PD before LD first became available experienced dyskinesia much sooner after the initiation of LD treatment than modern era patients. This is because these patients had a longer duration of PD, and therefore probably had more severe PD, before they received LD treatment. Since PD is a chronic progressive disease, longer disease durations and therefore more advanced central neurological changes may play a critical role in the development of LD induced dyskinesia. But dose, dosing strategy and duration of LD treatment are also believed to be important factors in the development of dyskinesia. It was suggested that after 9 or more years of treatment with LD almost 90% of patients may experience dyskinesia. Dosing strategy, particularly the timing of dosing in relation to meals, may influence the likelihood of MC developing because this affects potency of LD. Patients with young-onset (<40 years) PD appear to be at much greater risk of developing dyskinesia early in their course of treatment. Young-onset patients had a significant higher frequency of dyskinesia at 3 and 5 years of LD therapy compared with matched older-onset PD patients. In another study that assessed the 5-year incidence of dyskinesia in a population-based cohort in the US between 1976 and 1990, the incidence was 16% in patients with PD onset after 70 years of age, whereas with PD onset from 40 to 59 years of age, the incidence was much higher at 50% (for review:9,20).
Preventive treatment concepts for dyskinesia
Studies in drug-naive animal models of PD have shown that continuous dopaminergic stimulation is associated with reduced incidence and severity of dyskinesia compared with pulsatile administration.64,65 Continuous dopaminergic stimulation due to a more continuous delivery of dopaminergic drugs to the brain may be achieved through the administration of transdermal dopamine agonist administration, retarded release dopamine agonists or intra-duodenal LD application or by administering frequent doses of LD/DDI, so called LD fractionation, with or without a COMT inhibitor.35,48,49,63,66
COMT inhibition and dyskinesia onset
But addition of COMT-inhibitors to LD/DDI may induce dyskinesia according to pharmacokinetic and clinical trials, since the addition of COMT-inhibitors increases peak levels and the amount of plasma LD, which is delivered to the brain. Therefore in clinical practice, there is a need to titrate and to adjust the oral LD/DDI intake, when a COMT inhibitor is additionally introduced.
May early initiation of LD/CD/EN delay onset of dyskinesia?
The ELLDOPA study confirmed that LD dose is a factor in causing dyskinesia and that these can even develop as early as 5–6 months after treatment initiation. Patients receiving 600 mg/day experienced significantly more dyskinesia than patients receiving placebo, 150 or 300 mg/day (p < 0.001) (Table 1). The FIRST-STEP trial reported a not significant tendency towards a lower number of observed dyskinesia in the LD/CD/EN treated arm compared with the LD/CD treated PD patients (Table 2). The study was not powered to demonstrate this effect. An experimental animal trial showed lower frequency and less intensity of dyskinesia, when a treatment with LD/DDI with the COMT inhibitor EN, given four times daily, was started right from the beginning. 65 A further confirmatory result should be provided by the outcomes of the STRIDE-PD study (STalevo Reduction In Dyskinesia Evaluation), however this trial failed. 67 The reasons remained unclear. However nowadays we know that repeat EN dosing may also alter peripheral pharmacokinetic behaviour and gastrointestinal components of LD absorption, both of which were presumably underestimated respectively not known, when STRIDE-PD was designed.14,68
Different Pharmacokinetic LD Plasma Behaviour with and without COMT Inhibition
There are certain decisive different features between the LD/DDI administration with and without COMT inhibition.
Gastrointestinal absorption
Generally, LD uptake depends on the gastric emptying time, gastrointestinal absorption and transport via the gastrointestinal amino acid transporter system.28,68–72 PD Patients often receive a drug combination therapy that involves multiple daily dosing of a particular compound and additional supplementation with other drugs at least partially sharing the modes of action. Efficacy of all administered compounds depends on patient compliance, the nature of the delivery system, physicochemical properties of the drug and physiological considerations. Each of them is interrelated to the other ones and affects the rate at which the drug is absorbed throughout the gastrointestinal tract and thus its bioavailability and pharmacokinetic profile.28,68,72 In this respect EN improves the properties and dose of LD/DDI by prolonging the half life of LD. This was shown in pharmacokinetic trials with one time application of EN. However after repeat administration, COMT inhibition may also promote the synthesis of more basic LD metabolites, i.e. the tyrosine aminotransferase dependent substrates dihydroxyphenylpyruvate acetate and trihydroxyphenylacetate (Fig. 2). Therefore COMT inhibition may model the environmental pH and the physicochemical properties of LD for its duodenal absorption. COMT is located in higher concentrations in the membranes of the gastrointestinal tract. Generally, these physicochemical properties of a drug also affect its absorption through the gastrointestinal tract.14,68 Compounds, including LD, are weak bases or weak acids or are the salts of them and as such demonstrate pH dependent solubility. The pH partition hypothesis asserts that the passage rate of a drug through a membrane is dependent on the environmental pH and pKa of the drug. Drugs with low pKa are not ionized in the stomach and subsequently rapidly absorbed. On passage to the small intestine with comparatively increased pH, the rate of ionisation is changed and absorption subsequently slowed. The converse is true for drugs with higher pKa value. This influences the bioavailability of hydrophilic drug formulations. They have a narrow window of absorption, limited predominantly to the stomach or the upper intestine. Absorption is also limited by low pKa value and/or the site of active transport absorption mechanism, like in the case of LD.68,72,73 Additionally, absorption behavior of orally administered LD also depends on gastrointestinal transit rates, since uptake of LD occurs mainly in the proximal third of the small intestine (duodenum/jejunum) but not in the stomach. Intestinal LD absorption is rapid and complete, but the plasma bioavailability of LD is only 30% as a result from prior degradation to dopamine by DDI and to a lesser extent to 3-OMD by COMT, i.e. in the gut membranes. The longer LD is retained in the stomach and in the small intestine the more extensively it is metabolized and made less available for absorption. A formulation, which shares the peripheral absorption site profile of LD, is sodium-octanoate, which is employed as [13C] marked substrate in breath tests.4,68,72–76 These investigations are a non-invasive, feasible, alternative method without ionizing radiation to measure gastric emptying of solids and liquids. After intake, [13C]-sodium-octanoate is rapidly absorbed from the proximal intestine and carried to the liver via the portal venous system. There it is oxidized and eliminated as CO2 in the breath, reflecting gastric emptying as the rate limiting step of the process. Accordingly, significant associations between pharmacokinetic plasma behavior of LD and the outcomes of the [13C]-octanoic acid breath test appeared. In this study no impact of EN addition on gastric emptying time was found. But COMT inhibition with EN increased the recovery rate of the salt [13C]-sodium-octanoate (Fig. 3). 68
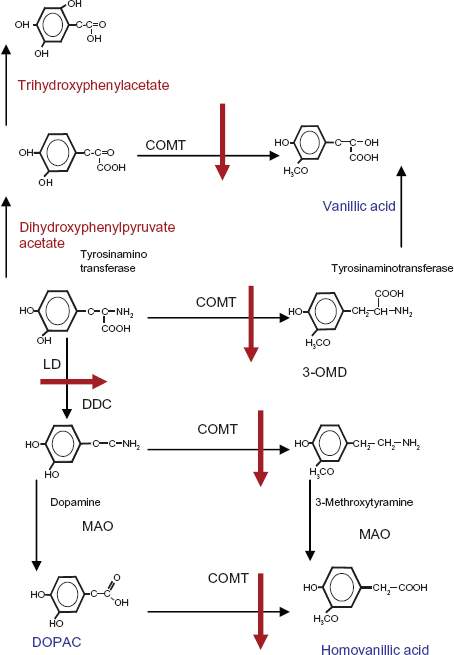
Metabolites of LD with (red) and without COMT-inhibition (blue).
Gastrointestinal LD absorption and onset of dyskinesia
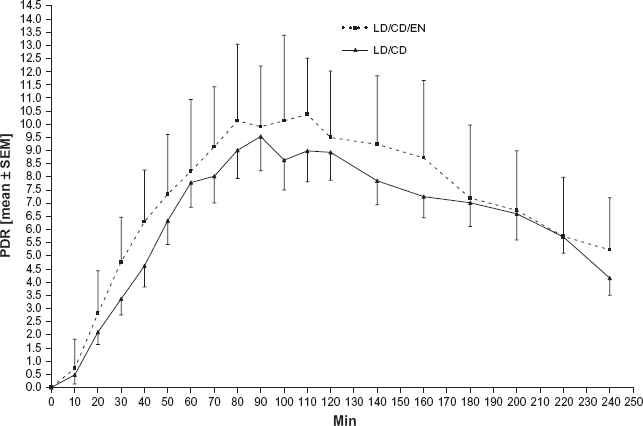
Therefore one may assume that LD is better absorbed with LD/CD/EN–-than with LD/CD treatment. In the long term, this results in higher LD plasma levels, which support onset of dyskinesia as shown in the ELLDOPA Study. Consequently one may additionally assume that repeat administration of LD/CD with COMT inhibition may also cause higher maximum concentrations of LD plasma levels than without. Studies, in which an additional application of COMT inhibitors was performed, partially showed an increase of the peak LD level dependent on the study design with frequent estimation of LD concentrations (Fig. 4).4,77,78 This figure also mirrors the individual variability of LD absorption, which may be reproduced, when strict standardized conditions are employed. 14
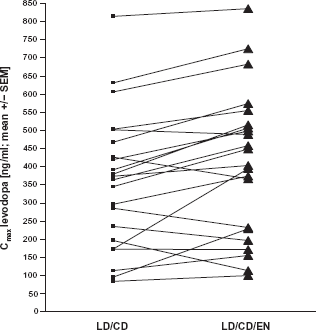
Data of peak LD plasma levels during the condition with repeat LD/CD and LD/CD/EN intake taken from. 14
The role of 3-OMD
3-OMD levels were also determined in these more recent pharmacokinetic studies, in order to investigate the metabolism of this LD derivative with its long plasma half life. 3-OMD competes with LD at the large neutral amino acid transport carriers of the gastrointestinal tract and of the blood brain barrier. High 3-OMD levels during the LD/CD administration may contribute to a reduced LD delivery to the blood and to the brain in particular during repeat administration. In contrast COMT inhibition decreases 3-OMD and thus improves absorption and blood brain barrier transfer, both of which support higher LD brain levels.16,68
Repeat EN administration increases the maximum LD plasma level
Pharmacokinetic trials demonstrated that switch from LD/CD- to the corresponding LD/CD/EN dosage improves motor symptoms despite the administration of the same oral LD dose. This is in line with prior trial outcomes on EN supplementation, applied with an extra tablet. Such a switch from LD/CD to LD/CD/EN in one tablet was well tolerated and showed an increased and prolonged LD efficacy by COMT inhibition. But EN supplementation also caused higher LD maximum plasma levels and an increased LD plasma bioavailability after repeat applications, which may be further enhanced by the putative long term effects of COMT inhibition provided by its effects on gastrointestinal absorption of LD and the subsequent transporter systems in relation with its metabolite 3-OMD.14,15,33
Conclusion
Supplementation of COMT-inhibitors, like EN, to a LD/DDI regime is complex and asks for close patient supervision and interaction through the treating physician. It may be necessary to reduce the total oral LD dosage or delay the intake of the next LD/CD/EN tablet in the long term following the COMT-inhibitor supplementation. This fine titration of drug therapy may be necessary due to a putative certain long term increase of LD plasma levels,27,31 resulting from altered gastrointestinal absorption and LD transport processes as consequence of chronic COMT-inhibitor addition.28,68,74,75 To date these predominant peripheral mechanisms have not been investigated and discussed in the context of COMT-inhibitor addition to a LD/DDI drug regime in detail yet. However they may hypothetically contribute to onset of MC, particularly of dyskinesia, following a switch from LD/CD to LD/CD/EN from one day to another in nearly prior optimum treated PD patients in clinical practice. From this point of view the recent introduction of more LD/CD/EN formulations to a now available portfolio with 50, 75, 100, 125, 150 or 200 mg LD containing tablets considerably eased necessary titration steps. This adaption may even be necessary after a certain interval, when the due to additional COMT inhibition associated metabolic long term changes of LD absorption come into account with the clinical manifestation of e.g. peak dose dyskinesia as long term effect in clinical practice. From this point of view, LD/CD/EN application may be of a certain advantage in contrast to the COMT-inhibition with 3 x 100 mg dosing of tolcapone which asks for a fixed combination regime with the available LD/DDI preparations.
Disclosure
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author reports no conflicts of interest.