
Abstract
Bipolar disorder is a common and serious illness usually requiring long term medication. We critically review the available evidence surrounding the increasing use of quetiapine, a second generation antipsychotic, in both the acute and maintenance phases of bipolar disorder. Large scale, randomized controlled data supports the use of quetiapine in both acute mania and acute bipolar depression, as a safe and effective treatment and probably best used in combination with a traditional ‘mood stabiliser’ such as lithium or divalproex. Also, quetiapine monotherapy has been shown to be effective in bipolar depression. Two recently published studies also confirm that quetiapine in combination with either lithium or divalproex ‘adds value’ to the maintenance treatment of bipolar disorder in terms of delaying relapse compared to either lithium or divalproex alone. Quetiapine is generally well tolerated, although further work on long term weight gain and emergent diabetes would be helpful.
Introduction
Bipolar affective disorder is a serious mental illness which is ranked as the fifth most disabling disease in the world by an influential WHO report, 1 and often has a chronic fluctuating course. Bipolar disorder is common, with a lifetime prevalence of 1.3%-1.6%, and more worryingly 10%-20% of individuals with bipolar disorder will commit suicide. 2 It has also been estimated that the annual cost to society of bipolar disorder in the UK is about £2 billion. 3
The treatment of bipolar disorder usually requires psychotropic medication to reduce symptom severity, stabilize mood, and prevent relapse. Consideration of the different phases of bipolar illness is helpful when treatment is being instituted namely, acute phase–-both manic and depressive; and long-term or maintenance phase treatment. Despite the relative paucity of high quality scientific data to aid prescribing, numerous guidelines exist around the world which summarise the expert view on the available evidence, as illustrated in Table 1. Table 1 shows that various expert committees have come to some rather differing conclusions as to the pharmacotherapy of the different phases of bipolar disorder, and also cannot make any recommendations for some phases (presumably due to limited data).
Guideline recommendations for pharmacotherapy in the various phases of bipolar disorder.
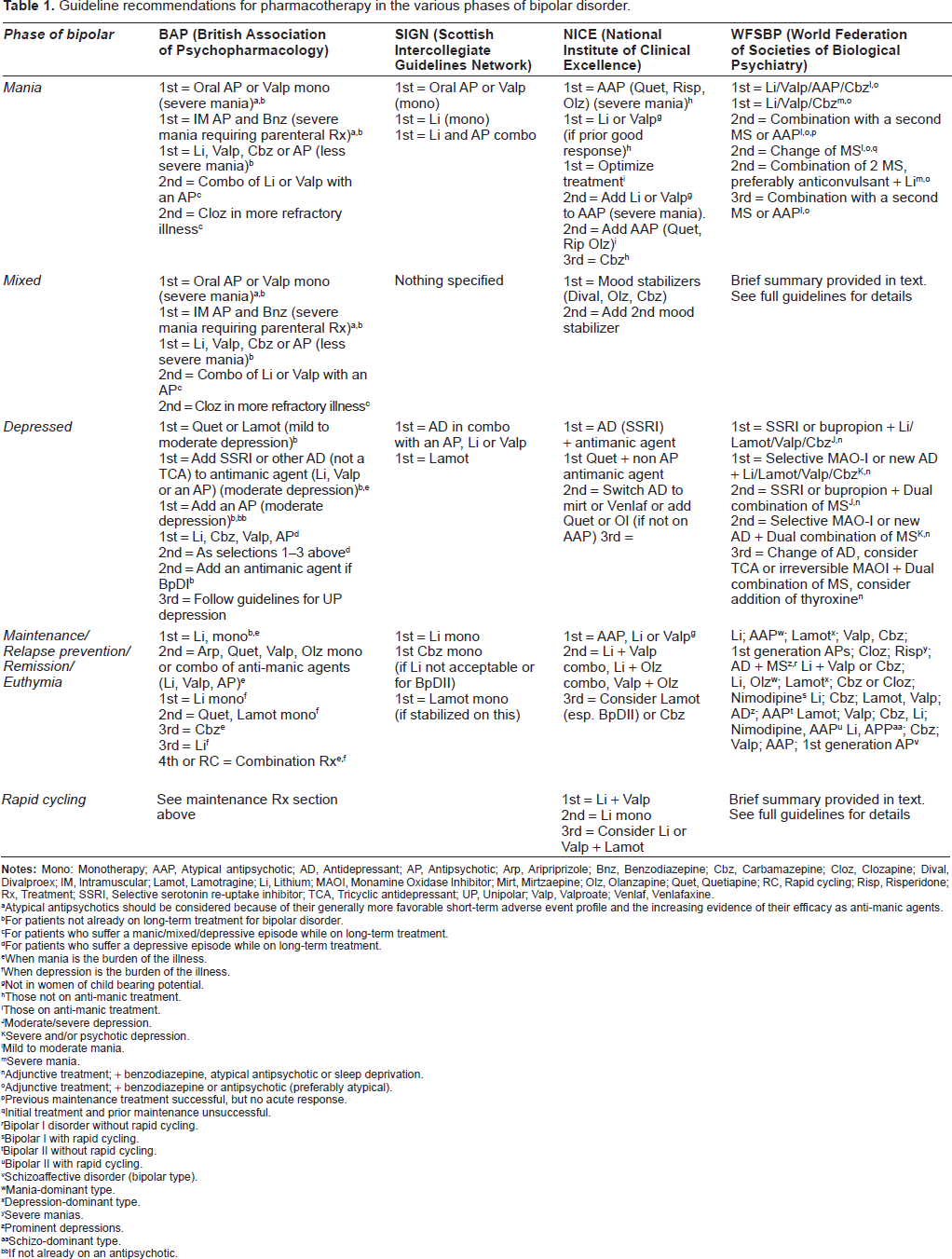
Atypical antipsychotics should be considered because of their generally more favorable short-term adverse event profile and the increasing evidence of their efficacy as anti-manic agents.
For patients not already on long-term treatment for bipolar disorder.
For patients who suffer a manic/mixed/depressive episode while on long-term treatment.
For patients who suffer a depressive episode while on long-term treatment.
When mania is the burden of the illness.
When depression is the burden of the illness.
Not in women of child bearing potential.
Those not on anti-manic treatment.
Those on anti-manic treatment.
Moderate/severe depression.
Severe and/or psychotic depression.
Mild to moderate mania.
Severe mania.
Adjunctive treatment; + benzodiazepine, atypical antipsychotic or sleep deprivation.
Adjunctive treatment; + benzodiazepine or antipsychotic (preferably atypical).
Previous maintenance treatment successful, but no acute response.
Initial treatment and prior maintenance unsuccessful.
Bipolar I disorder without rapid cycling.
Bipolar I with rapid cycling.
Bipolar II without rapid cycling.
Bipolar II with rapid cycling.
Schizoaffective disorder (bipolar type).
Mania-dominant type.
Depression-dominant type.
Severe manias.
Prominent depressions.
Schizo-dominant type.
If not already on an antipsychotic.
Second generation or ‘atypical’ antipsychotics are increasingly licensed (and used) for bipolar disorder as illustrated in Table 1, and also are known to be frequently used ‘off license’ in bipolar disorder.4,5 Initially these antipsychotics were proven to be effective in the treatment of acute phases of bipolar disorder, and more recently antipsychotic treatment studies have extended into the maintenance phase. 6
Quetiapine is a second generation antipsychotic medication initially approved by the U.S. Food and Drug Administration in 1997 for the treatment of patients with schizophrenia, but due to its favorable side-effect profile it has been beneficially used across a range of mental disorders 7 including mood disorders. 5 The quetiapine molecule was originally modelled on clozapine, and has multi-receptor affinity. Colloquially it would appear to have a dose related ‘tri-phasic’ receptor uptake pattern, with sedative histaminic properties apparent at low dose (e.g. <200 mg per day); some antidepressant serotonergic and α-adrenergic effects seen at moderate dosages (e.g. 200-400 mg per day, although antidepressant effects at lower doses has been described), and the antipsychotic dopaminergic properties being most apparent at higher daily doses (e.g. >400 mg per day). Jensen et al 8 have also identified that a metabolite of quetiapine, N-desalkylquetiapine, is a potent norepinephrine (noradrenaline) reuptake inhibitor and partial 5-HT1A agonist which could explain the antidepressant activity similar to tricyclic antidepressants.
Quetiapine is the only antipsychotic currently approved for use in the United States for the treatment of bipolar mania and bipolar depression, and quetiapine XR (or XL in Europe), which is a prolonged release variant of quetiapine allowing once daily dosing, is FDA approved for mixed state bipolar disorder and bipolar depression.
Here we examine the burgeoning evidence surrounding the use of quetiapine in bipolar disorder, both in the acute and maintenance phases of the illness. For example, at the beginning of 2009 an electronic search of medical databases using the keywords “quetiapine”; “seroquel”; “bipolar disorder”; and “manic depression” revealed 237 relevant matches. We critically review the available scientific data, consider the important gaps in the literature, and speculate about any future developments concerning quetiapine use in mood disorder.
Treatment of the Acute Phase of Bipolar Disorder
Treatment of Acute Mania
Current NICE Guidelines for the treatment of acute mania and hypomania recommend starting an antipsychotic, valproate or lithium (see Table 1). Only lithium, olanzapine, quetiapine, risperidone and valproate semi sodium are licensed for the acute treatment of mania in the UK. A meta-analytic review 9 of randomized controlled trials looking at the use of second generation antipsychotics in the treatment of acute mania reviewed 24 studies (with 6187 patients included) and found that whilst the second generation antipsychotics displayed efficacy comparable with that of mood stabilisers, the most efficacious treatment was a combination of a mood stabiliser and a second generation antipsychotic.
A number of studies have looked at quetiapine monotherapy and quetiapine in combination with lithium or valproate semi sodium, otherwise known as divalproex, in the treatment of bipolar mania.
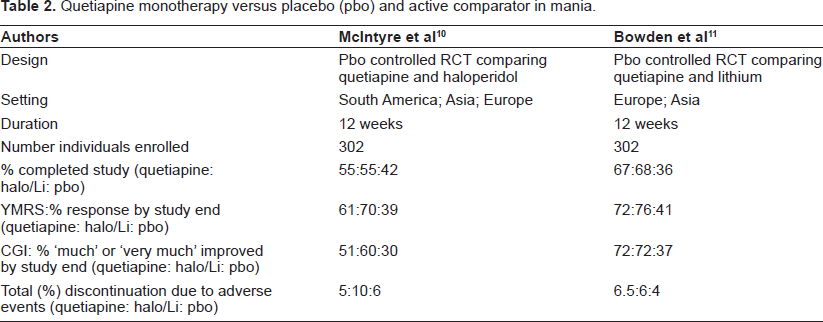
McIntyre et al 10 found that quetiapine and haloperidol were equally efficacious as monotherapy for bipolar (type I) mania in a 12 week randomized trial, with the most effective dose range for quetiapine being 400-800 mg per day for resolution of manic symptoms according to the Young Mania Rating Scale (YMRS). A further study 11 evaluated the efficacy and tolerability of quetiapine monotherapy versus placebo for the treatment of mania over a 12 week period. This randomized, double blind, placebo–-controlled study again used a reduction in YMRS as the primary outcome measure and concluded that quetiapine demonstrated superior efficacy to placebo in patients with bipolar mania and was well tolerated. Both these studies are summarised in Table 2.
Quetiapine monotherapy versus placebo (pbo) and active comparator in mania.
The efficacy and tolerability of quetiapine in Chinese patients hospitalized with acute bipolar mania was compared to lithium over a 4 week period in a randomized double blind study. 12 135 people completed the study, with YMRS as a primary endpoint. This study found that both response rate at 28 days and the overall remission rate were significantly greater with quetiapine than lithium which is arguably unexpected, although possibly these results cannot be generalised to other ethnicities.
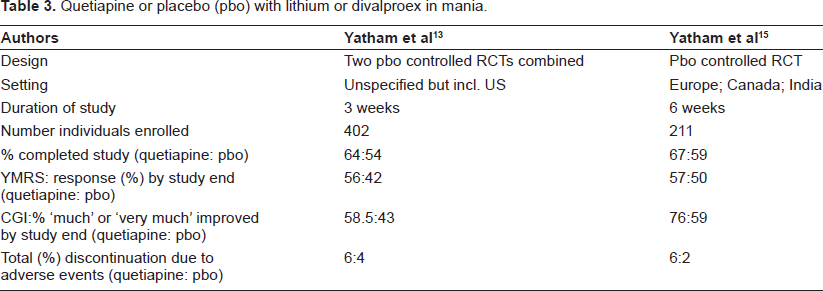
Quetiapine combined with lithium or divalproex for the treatment of bipolar mania has been evaluated in three double-blind, placebo-controlled studies.13–15 Yatham et al 13 perhaps unusually combined the results of an earlier randomized study 14 with an identically designed later study “to increase power”. A total of 402 patients were randomized, with the primary outcome being improvement in the YMRS. At day 21 in the quetiapine plus lithium or divalproex was statistically superior to the placebo plus lithium/divalproex group. Improvements in the Clinical Global Impression-Bipolar severity of illness scores by day 21 were also significantly greater in quetiapine plus lithium/divalproex treated patients. However, a second trial by Yatham et al 15 of quetiapine combined with lithium or divalproex showed an improvement in YMRS of only 2 points when compared with lithium/divalproex and placebo, and this was not statistically significant. These two trials by Yatham et al are summarized in Table 3.
Quetiapine or placebo (pbo) with lithium or divalproex in mania.
A post hoc analysis 16 of four similar, randomized, double-blind, placebo controlled trials of quetiapine in bipolar mania showed that quetiapine as monotherapy, or in combination with lithium or semi-sodium valproate, was effective for acute mania and that quetiapine is efficacious even when medically serious symptoms are present. In all the studies mentioned above the daily dose range of quetiapine was between 300 and 800 mg.
Thus in summary, for acute bipolar mania, both quetiapine monotherapy and quetiapine in combination with a ‘mood stabiliser’ such as lithium or divalproex appear effective and well tolerated treatments. No study comparing quetiapine alone versus quetiapine plus a mood stabiliser has been identified and this would be useful in determining which is superior. Clinical experience and naturalistic work 5 would suggest that combination therapy adds value, as recommended by meta-analysis, 9 in terms of balancing symptom resolution against side effect profile.
Treatment of Acute Bipolar Depression
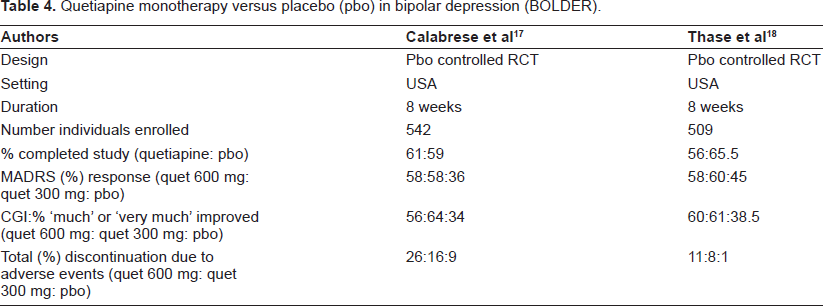
The treatment of bipolar depression with quetiapine monotherapy was studied in two AstraZeneca funded trials known by the acronym BOLDER,17,18 conducted in the US. Both of these 8-week, placebo-controlled, double-blind studies compared two doses of quetiapine -300 mg per day and 600 mg per day, and included patients with bipolar I and bipolar II depressive episodes and eligible patients with histories of rapid cycling mood disorder. Both studies used change in the Montgomery-åsberg Depression Rating Scale (MADRS) total score as the primary endpoint.
BOLDER I 17 enrolled 542 patients meeting criteria for a current episode of bipolar I (n = 360) or bipolar II (n = 182) depression. 326 patients completed the 8 week study. Both doses of quetiapine resulted in significant improvements in MADRS total scores at all time points measured, with statistical significance over placebo detected after only 1 week of treatment (the first assessment point of the study) and maintained at every time point thereafter. The proportion of patients classified as responders to treatment, defined as a ≥50% improvement in MADRS total score at study endpoint, was significantly higher in both groups receiving active quetiapine (58% in both groups) than in the group randomized to placebo (36%). Remission rates (defined as a final MADRS total score ≤12) followed a similar pattern (53% for both 300 mg and 600 mg quetiapine, 28% for placebo). Dry mouth, sedation/somnolence, and dizziness were the common adverse events compared to placebo.
Cookson et al 19 undertook a post-hoc analysis of BOLDER I, and showed that the ‘number needed to treat'–-a clinically relevant measure of how often one can expect a response–-for quetiapine was five. This is impressively low, and reflects the underlying remission rates mentioned above. Furthermore, a secondary analysis of anxiety symptoms in BOLDER I 20 demonstrated that after 8 weeks both 300 mg and 600 mg of quetiapine significantly improved overall anxiety in those with bipolar I disorder.
Bipolar disorder is also associated with substantial impairment in health related quality of life, including social and emotional functioning, occupational impairment and high utilization of healthcare services. 21 BOLDER I and II also generated a post-hoc study 22 of the effect on quality of life and sleep with quetiapine monotherapy in bipolar depression. Both the 300 mg and the 600 mg doses of quetiapine significantly improved quality of life and sleep by day 57, with the effect being more pronounced at the higher dose. These were subjective measures though, and it is possible that the quality of life improvement may simply reflect symptomatic improvement. Quetiapine therapy also led to significant improvement in quality of sleep compared with placebo which is not a huge surprise.
The results of the later BOLDER II study 18 replicated the first study in terms of the primary outcome variable, with quetiapine-treated patients displaying significantly greater mean improvement in MADRS total scores than placebo-treated patients. 509 individuals were randomized in BOLDER II, and 301 completed the 8 week study, although here proportionately more dropped out from the quetiapine groups than placebo interestingly. Response rates for both doses of quetiapine monotherapy were also similar to those observed in the original study (60%, 58%, and 45% for the 300 mg, 600 mg, and placebo groups, respectively), as were remission rates (52% for both groups receiving quetiapine as compared to 37% for those receiving placebo). Again, dry mouth, sedation/somnolence, and dizziness were the common (short term) adverse events associated with quetiapine.
In both BOLDER studies the incidence of treatment emergence mania or hypomania was lower in the quetiapine treatment group than the placebo group, but the positive placebo response was higher in BOLDER II. The BOLDER studies concluded that quetiapine monotherapy is an effective and well tolerated treatment, over 8 weeks, for acute depressive episodes in bipolar disorder. Interestingly, the 300 mg daily dose appears to be more effective (and better tolerated) in bipolar depression than the 600 mg daily dose. The BOLDER studies are summarized in Table 4.
Quetiapine monotherapy versus placebo (pbo) in bipolar depression (BOLDER).
Suppes et al 23 conducted a placebo controlled RCT of quetiapine XL 300 mg per day as monotherapy for bipolar (I or II) depression. This was an 8 week study with 133 and 137 (placebo) individuals enrolled, but is only available in abstract form thus far. The primary outcome was MADRS improvement, and a significant improvement with quetiapine XL versus placebo was found (-17.4 vs. -11.9) after 8 weeks treatment, although about 8% of those on quetiapine developed ≥7% weight gain or high triglyceride levels.
To date, these encouraging results have not been confirmed in further work from AstraZeneca or elsewhere, although Oxford University (in the UK) have recently commenced a randomized pragmatic comparison of quetiapine monotherapy with lamotrigine and quetiapine combination–-the two current front-runners for added efficacy in bipolar depression–-called the CEQUEL trial.
Maintenance Pharmacotherapy in Bipolar Disorder
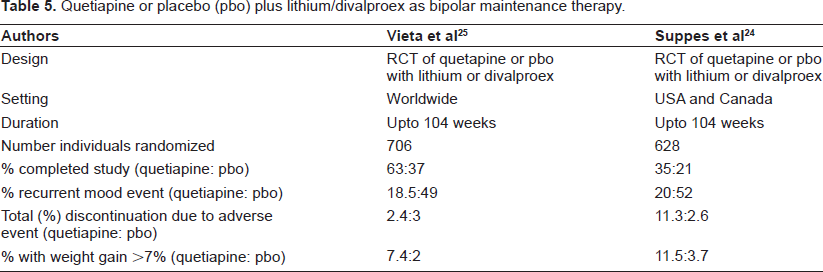
Suppes et al 24 compared quetiapine with placebo as an augmentation agent with either lithium or divalproex in a randomized double blind trial, as maintenance treatment for bipolar I disorder for a duration of up to 104 weeks. The primary outcome, after a 12 week run in phase, was recurrence of a ‘mood event’ (mania, depression, or a mixed episode) involving new medication. Hospitalization, study discontinuation, and significant change in the YMRS and MADRS were other outcomes studied. A total of only 176 patients completed the study from the 1953 individuals enrolled illustrating the complexity (and expense) of long term maintenance studies. Fewer individuals on quetiapine augmentation (20%) experienced a mood event compared to placebo (52%). Weight gain, sedation, and raised blood glucose were all more frequent in the quetiapine group. Study limitations included the (usual) exclusion of women who may become pregnant, and those with co-morbid medical illness or substance misuse, as well as selecting an ‘enriched’ sample of responders from the run-in phase.
Vieta et al 25 also separately studied quetiapine versus placebo as augmentation therapy with either lithium or divalproex in the prevention of recurrent ‘mood events’ in bipolar I disorder, again over up to 104 weeks. Here, 347 individuals (from a total enrolment of n = 1461) completed the study, with substantially more of the placebo group dropping out compared to quetiapine. Quetiapine again reduced the risk of a recurrent mood event compared to placebo (18.5% vs. 49%), corresponding to a relative risk reduction of relapse of 72%. Important adverse events noted, compared to placebo, after randomization in the quetiapine arm were weight gain, and a higher rate of emergent high fasting glucose. The same limitations as noted for the Suppes et al trial applied to this trial.
Taken together, these two published maintenance studies24,25–-summarised in Table 5–-of augmenting lithium or divalproex with quetiapine offer convincing evidence of a significant reduction in relapse rate in bipolar I disorder, compared to lithium or divalproex monotherapy.
Quetiapine or placebo (pbo) plus lithium/divalproex as bipolar maintenance therapy.
A further maintenance study in bipolar I disorder has been presented at conference, and compares quetiapine and lithium with placebo. 26 This study, which lasted a maximum of 104 weeks, indicates that quetiapine and lithium were equally effective maintenance treatments and both superior to placebo in reducing risk to a recurrent mood event, although the full study details are not yet in the public domain.
AstraZeneca also has two other studies27,28 of the maintenance treatment of bipolar depression, known by the acronym Embolden, which examine quetiapine and placebo with either lithium (Embolden I) or paroxetine (Embolden II). Unfortunately both these studies are only available in abstract form. Each study has two phases with over 500 patients, namely an acute phase replicating the BOLDER studies design and then a continuation phase where quetiapine responders were re-randomized to either quetiapine (300 mg) or placebo and studied for an additional 26-52 weeks. The abstracts indicate that quetiapine was more effective in reducing depressive symptoms compared with placebo or the other agents after an 8 week trial, although at this time little data on the maintenance phase treatment is in the public domain.
Other related work includes a naturalistic study from Italy, 29 where 232 individuals with either bipolar I or II were followed up for four years. Using survival analysis, they found that quetiapine (in low dose) plus lithium or valproate was superior compared to either monotherapy in maintaining euthymia (mood stability), although they acknowledged the limitations of a lack of randomization or control groups.
Finally, concerning the risk of diabetes in bipolar disorder, a long term retrospective review 30 from a large US medical claims database observed that the development or exacerbation of diabetes was associated with antipsychotic use in bipolar disorder. In particular, the hazard ratios (HR) were greatest for clozapine (HR = 7.0), with risperidone (HR = 3.4) and olanzapine (HR = 3.2) being intermediary, and quetiapine having an HR = 1.8. As always when prescribing, a risk/benefit balance needs to be achieved when a decision to prescribe is made, after discussion between the doctor and patient.
Quetiapine use in Bipolar Disorder with Comorbid Substance Misuse
Both alcohol and drug misuse are commonly seen in those with bipolar disorder, often representing self-medication and thrill seeking. Clinician reported rates of comorbid substance misuse, in ‘real world’ populations, can be up to 40% of all cases 4 and constitutes a significant management problem which can exacerbate prognosis.
Nejtek et al 31 studied 124 outpatients with cocaine or metamphetamine use or craving and bipolar (I or II) disorder who were entered into a randomized controlled trial comparing risperidone and quetiapine prescription. 80 outpatients were eligible for analysis, and both risperidone and quetiapine improved mood symptoms and reduced drug cravings equally. The absence of a control group, and the necessary use of inclusion and exclusion criteria in this study limit the generalizability of these findings. Brown et al32,33 also conducted two small open label pilot studies of quetiapine use in bipolar disorder with drug dependence, and found that drug use and craving reduced subsequent to quetiapine use.
The same group from Texas, 34 in a separate study, randomly assigned 115 outpatients with bipolar (I or II) disorder and alcohol abuse or dependence to quetiapine or placebo as ‘add-on therapy’. Here, impressively, 102 outpatients lasted the 3 year study but quetiapine was no better than placebo in terms of reducing alcohol use or the YMRS score, although depressive symptoms (as measured by the Hamilton Rating Scale for Depression) did significantly improve with quetiapine use. A small 12 week open label study 35 examining quetiapine use in bipolar disorder with co-existent alcohol dependence did however find a significant reduction in drinking at endpoint, although Longoria et al 36 found the number of alcoholic drinks did not diminish in 14 individuals with alcohol craving and bipolar disorder who were prescribed quetiapine. Again, this was a small short uncontrolled study.
Conclusions
Bipolar disorder is usually a chronic disabling condition requiring long term medication. Here we critically appraise the evidence surrounding the use of quetiapine in bipolar disorder–-both in the acute and maintenance phases.
In the acute phase of bipolar disorder, there can be a serious risk of self harm, aggression, and even suicide, and medication is usually essential. When considering the use of quetiapine in acute bipolar disorder, there is convincing evidence supporting quetiapine therapy in acute bipolar I mania, at mid-to-high (i.e. 300-800 mg per day) dose, in combination with either lithium or divalproex.
With regard to the use of quetiapine in acute bipolar depression, the two BOLDER studies also support the use of quetiapine in acute bipolar depression, either as monotherapy or in combination with a mood stabiliser with the most effective daily dose of quetiapine being nearer to 300 mg than 600 mg. Ideally, however, the BOLDER studies should be independently replicated by other research groups to confirm these promising findings. In the future, we suspect that bipolar (I or II) depression may become (along with maintenance therapy) the primary indication for quetiapine use in bipolar disorder, and that quetiapine and lamotrigine 37 will become first line treatments for bipolar depression.
Turning to the long term maintenance medication for bipolar I and II disorder, the twin studies of Suppes et al, and Vieta et al provide persuasive evidence that quetiapine augmentation of either lithium or divalproex is an efficacious and safe strategy. Again, independent replication of these results would be desirable, and concerns over weight gain and emergent diabetes need to be further addressed although early evidence30,38 suggests that quetiapine is not the worst offender amongst second generation antipsychotics. These adverse event risks need to be balanced against the risks of un-treated or under-treated bipolar disorder mentioned above.
The prolonged release version of quetiapine (known as XR in the US and XL in Europe) is now available, and although it has the same half-life as the original quetiapine, it has a gel polymer ‘wrapping’ delaying gastro-intestinal release. Quetiapine XR is FDA approved for bipolar depression and mixed state bipolar disorder. It is worth noting that quetiapine XR/XL should be taken at least one hour before or after a meal, and dosing is straightforward–-namely 300 mg on day 1 and 600 mg on day 2 for bipolar mania (and schizophrenia).
The data on quetiapine use in bipolar disorder with comorbid substance use are equivocal, so no firm recommendation can be made here. Nevertheless, this is a clinically important area that deserves further study, perhaps using innovative combinations of anti-craving drugs (e.g. naltrexone) and conventional bipolar therapies. Finally, we also expect to see future trials of quetiapine use in other mood disorders such as refractory depression and borderline or emotionally unstable personality.
Declaration of Interest
MT and PS have received hospitality and fees from pharmaceutical firms, including AstraZeneca, the manufacturers of quetiapine.