
Abstract
Abdominal pain is one of the most common reasons why people seek medical care, and is often due to spasm of intra-abdominal visceral organs. Hyoscine butylbromide (HBB) is a quaternary ammonium compound which blocks the action of acetylcholine at parasympathetic sites (both muscarinic and nicotinic receptors) in smooth muscle, and in secretory glands. It causes decreased motility of the gastrointestinal tract and the urogenital tracts, and is useful in the treatment of spasms in these regions. Side effects are common, but tend to be minor and self limiting. Evidence exists to support its use in the management of non-specific colicky abdominal pain (in adults and children); irritable bowel syndrome; labor and delivery; dysmenorrhea; as an adjunct in the therapy of late stage cancer patients with inoperable bowel malignancies; and to facilitate improved resolution in certain imaging techniques. It may also be useful in certain procedures, such as colonoscopy and sigmoidoscopy, and may be useful in the management of renal colic (although NSAIDs seem clinically superior). The role of HBB in the management of esophageal food obstruction is unclear at this time; further studies need to be done.
Introduction
Abdominal pain is one of the most common reasons why people seek medical care (after headaches, backaches, and dizziness), and may be related to transient self limiting disorders or to serious life threatening disease requiring prompt medical intervention. Arriving at a definitive diagnosis may be difficult, because of the number of organ systems in the abdomen, and because a multiplicity of diseases may cause this symptom.
Because of the variety of illnesses which may result in this symptom, abdominal pain is a concern of general practitioners/family physicians, surgeons, internists, emergency medicine doctors, pediatricians, gastroenterologists, urologists, and gynecologists worldwide.
The pathogeneses of abdominal pain are varied and numerous, but tend to fall into one (or more) of the following categories:
Processes resulting in inflammation of the parietal peritoneum, and/or associated with inflammation of a solid viscus, tend to cause pain which is steady and aching, and worsened by changes in the tension of peritoneum caused by pressure/compression, stretch or positional change. It is often accompanied by guarding–-contraction of the abdominal muscles to relieve peritoneal tension.
The pain associated with obstruction of a hollow viscus is often intermittent or “colicky”, coinciding with the peristaltic waves of the organ attempting to clear the obstruction.
The pain associated with abdominal vascular disturbances (thrombosis or embolism) is related to the onset of hypoxia/ischemia of the tissue distal to the occlusion; it can be sudden or gradual in onset, and severe or mild in intensity.
Functional gastrointestinal disorders, such as functional dyspepsia and irritable bowel syndrome. 1
Abdominal pain may be referred from sites outside the abdomen (e.g. lower lobe pneumonia).
In terms of frequency, inflammation of the hollow and solid viscera, with accompanying peritoneal irritation, are among the most common causes of abdominal pain. Examples of these include common diagnoses such as gastritis, gastroesophageal reflux, peptic ulcer disease, appendicitis, cholecystitis, hepatitis, bowel obstruction, ureteric colic, cystitis, pyelonephritis, and primary dysmenorrhea.
Introduction to Hyoscine Butylbromide
Hyoscine-N-Butylbromide (HBB) is a derivative of hyoscine which is extracted from the leaves of the Duboisia tree found mainly in Australia.
Review of Pharmacology, Mode of Action, and Pharmacokinetics
Hyoscine-N-butylbromide is also referred to as Scopolamine-N-Butylbromide,N-ButylScopolammonium Bromide, and butylscopolamine. Its molecular formula is C21H30BrNO4 and it has a molecular weight of 440.37.
Hyoscine-N-butylbromide contains a nitrogen molecule with four different bonds to varying chemical groups, making it a quaternary ammonium compound. Hyoscine-N-butylbromide is highly polar, and in contrast to ammonium (NH4+) and other related compounds, it retains its polar nature regardless of the surrounding pH. Hence it is only partially absorbed (8%) following oral administration and the systemic availability was found to be less than 1%. Nevertheless, despite the briefly measurable low blood levels, hyoscine-N-butylbromide and/or its metabolites have been observed at the sites of action.
After intravenous administration, the substance is rapidly distributed into the tissues (t½ = 29 min). It does not pass the blood-brain barrier and plasma protein binding is low. Most of the drug is metabolized in the liver, with the half-life of the terminal elimination phase being approximately 5 hours. Approximately half the metabolites are excreted in the urine.
Background Physiology, Mechanism of Action, Clinical Use and Side Effects
The parasympathetic nervous system uses acetylcholine almost exclusively as its neurotransmitter. The acetylcholine acts on two types of receptors, the muscarinic and nicotinic cholinergic receptors. Most transmissions occur in two stages: When stimulated, the preganglionic nerve releases acetylcholine at the ganglion, which acts on nicotinic receptors of postganglionic neurons. The postganglionic nerve then releases acetylcholine to stimulate the muscarinic receptors of the target organ.
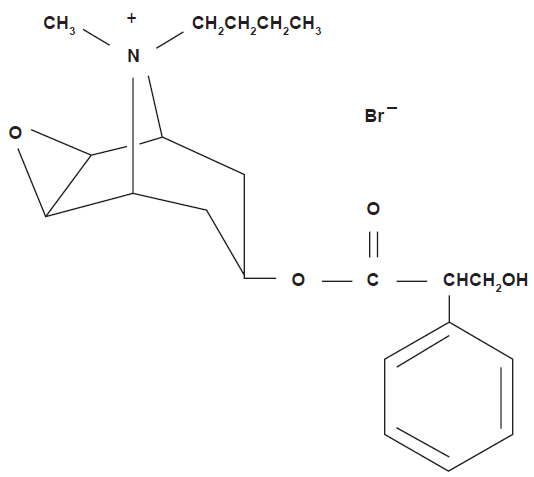
The molecular formula of hyoscine butylbromide.
The three main types of muscarinic receptors that are well characterized are:
The M1 muscarinic receptors, located in the neural system.
The M2 muscarinic receptors, located in the heart. These reduce the conduction velocity of the sinoatrial and atrioventricular nodes.
The M3 muscarinic receptors, which are located at many places in the body, notably the smooth muscle of the blood vessels, pulmonary bronchi and the gastrointestinal tract, and various glands associated with the respiratory and gastrointestinal tracts. Stimulation of these receptors indirectly leads to vasodilatation (through nitric oxide production), bronchoconstriction, and an increase in intestinal motility, as well as an increase in glandular secretions. M3 receptors are also found in the ciliary bodies and pupillary muscles of the eye, where they help with accommodation and control of the size of the pupil.
Of note both M2 and M3 receptors are found in the organs of the urogenital system.
M4 and M5 receptors also exist, with the former being found mainly in the central nervous system. The full characteristics of action and location of the M5 receptors have not yet been fully elucidated.
Recent studies have also shown that HBB potently blocks nicotinic receptors, in a non-competitive fashion, in vitro. If this action also occurs in vivo, then this would add an additional mechanism of action for the drugs spasmolytic activity. 2
Hyoscine butylbromide blocks the action of acetylcholine at parasympathetic sites in smooth muscle, and secretory glands. Both its primary therapeutic effects and its side effects are based on this. Thus:
It causes decreased motility of the gastrointestinal tract and the urogenital tracts, and is useful in the treatment of spasms in these regions, as may be seen in gastroenteritis, colitis, inflammatory bowel disease, diverticulitis, biliary colic, cystitis, ureteric colic, and primary dysmenorrhea. It is also used to prevent spasms of the gastrointestinal tract prior to invasive radiologic and diagnostic procedures, such as endoscopic retrograde cholangiopancreatography (ERCP) and colonoscopy.
Its inhibitory action on glands in the oral cavity, gastrointestinal tract, and respiratory tract causes a reduction in their activity, with a consequent reduction in secretions. This makes the drug useful prior to induction of general anesthesia, and as a part of adjuvant management in cases of intestinal obstruction, in circumstances where surgical correction is not feasible (e.g. peritoneal carcinomatosis).
As might be expected based on the action of the drug, potential side effects/adverse effects are numerous, and involve almost all organ systems. The most common are:
Ocular: Blurred vision, photophobia, increased intraocular pressure
Respiratory: Dry nose, bronchospasm (occasional)
Cardiovascular: tachycardia, palpitations
Gastrointestinal: Constipation, xerostomia (dry mouth), dry throat
Renal: Urinary retention.
Central nervous system side effects have also been described (e.g. headaches; drowsiness), but as the drug does not cross the blood-brain barrier, these are more likely secondary effects caused by a direct effect of the drug (e.g. decreased blood pressure).
In addition, it should be noted that the type and severity of side effects are quite closely linked to the method of administration. Because the oral absorption and subsequent systemic bioavailability are so low (8%, and 1%, respectively), side effects from this method of administration are much less common at standard doses, than with the equivalent dose given parenterally.
Fortunately, the most common adverse effects are usually mild, and resolve spontaneously as the medication is cleared from the system. Of note is the fact that as a quaternary ammonium derivative, hyoscine butylbromide does not enter the central nervous system. Therefore, anticholinergic side effects at the central nervous system do not occur. Peripheral anticholinergic effects result from a ganglion-blocking action within the visceral wall, as well as from anti-muscarinic activity.
Hyoscine butylbromide is contraindicated in myasthenia gravis, and in megacolon/Hirschsprung's disease. In addition, it should not be administered parenterally in patients with untreated narrow angle glaucoma; tachycardia; hypertrophy of the prostate with urinary retention; and mechanical stenoses of the gastrointestinal tract.
Review of Clinical Applications
Abdominal Pain (Non-Specific Colic) and Irritable Bowel Syndrome (IBS)
The basis for the use of hyoscine butylbromide (HBB) in the management of non-specific abdominal colic lies within its anti-muscarinic effects. This effect manifests clinically in relaxation of the smooth musculature of the gastrointestinal tract, with improvement/resolution of the spasms/cramps perceived by the patient. This effect has been objectively demonstrated by a study looking at both the electrical and biomechanical activity in the stomach, where 20 mg of intravenous HBB was shown to decrease the mechanical motility index by 50.9%, while for electrical motility index the reduction was 36.5%. 3
The main areas of clinical application, and therefore of review, of hyoscine butylbromide in abdominal pain were in the contexts of non-specific colicky abdominal pain, irritable bowel syndrome, biliary colic, and gastroesophageal reflux disease (GERD).
Hyoscine butylbromide (HBB) has been studied in the context of non-specific abdominal pain in several recent studies. One of the most recent large studies compared the efficacy and tolerability of oral HBB 10 mg given three times daily, paracetamol 500 mg three times daily, and their fixed combination, against placebo in patients with recurrent crampy abdominal pain. 4 A total of 1637 patients were all given a week of placebo, then randomized to three weeks of treatment with one of the four therapies. Pain intensity (as measured by the Visual Analogue Scale, and Verbal Rating Scale) decreased in all treatment groups, by statistically significant amounts, as compared to placebo. All treatments were well tolerated, with the incidence of side effects not significantly different between the groups.
Another study involved 204 children, observed over the course of a week, where the drug was compared to a homeopathic preparation. Both preparations were found to provide significant improvement in symptoms (severity of spasms, pain/cramps, sleep disturbances, eating or drinking difficulties, and frequent crying, as observed by a parent/minder) and were well tolerated. 5
Tytgat et al have published two review series looking at the use of oral/enteral HBB specifically for the treatment of cramping abdominal pain, 6 and another examining the drug in a number of clinical scenarios. 7 Ten placebo-controlled studies were evaluated in the first study, where the efficacy and safety of oral or rectal HBB was assessed. The drug was considered beneficial in all of these trials, which the author used as evidence to support its use in the treatment of abdominal pain caused by cramping.
The second study examined the drug and its use in treating abdominal cramps/spasm; for diagnostic imaging purposes; the therapeutic efficacy and safety of the parenteral administration of HBB for treating biliary and renal colic and acute spasm in the genito-urinary tract; and for labor and palliative care. The author concluded that the drugs rapid action and beneficial efficacy combined with good tolerability support its use in a range of indications related to acute abdominal spasm, in labor and palliative care and for supporting diagnostic and therapeutic abdominal procedures, where spasm may be a problem. 7
The pharmacological profile of hyoscine butylbromide intuitively makes it useful in the management of irritable bowel conditions, and this has been supported in the literature. One group of researchers performed a double-blind, randomized parallel group trial comparison involving 712 patients with irritable bowel syndrome. Patients were given HBB plus paracetamol, HBB, paracetamol or placebo over a treatment period of four weeks. A visual analogue scale was used for assessment of symptoms, and at the end of the four weeks over 75% of the patients in the HBB groups showed improvement in symptoms. 8 In addition, there was a statistically significant improvement in abdominal pain intensity in the HBB group versus the placebo group and versus the paracetamol group. Other researchers confirmed that HBB is as effective as other similar medications, such as cimetropium, otilonium, mebeverine, trimebutine and pinaverium bromide, and superior to placebo, in the management of irritable bowel syndrome,9,10 supporting the general consensus that antispasmodics are useful for the treatment of irritable bowel syndrome. 11
Our review found only one study which assessed the efficacy of hyoscine butylbromide and its use in biliary colic. This study involved 72 patients, half of whom received HBB, and the other half diclofenac. Diclofenac provided much more rapid relief of pain than HBB, as shown by significantly lesser pain scores after injection of the drug (complete relief occurred in four hours in 91.7% of patients on diclofenac, vs. 69.4% with HBB. 12 Another interesting finding of this study was that progression to acute cholecystitis was seen in only 16.66% of patients on diclofenac as compared to 52.77% on HBB, suggesting that in addition to being a superior analgaesic, diclofenac can also prevent progression of biliary colic to acute cholecystitis in a significant number of patients.
Previous research showing the efficacy of atropine in the management of reflux disease prompted one group of researchers to assess the efficacy of hyoscine butylbromide and its use in gastroesophageal reflux disease. 13 Ten normal subjects and 10 patients with gastroesophageal reflux disease were evaluated by recording esophageal and gastric pH-metry for a 24-h period, using a probe positioned in the gastric body, and another placed 5 cm above the lower esophageal sphincter, in each patient. Recording lasted without interruption for 48 h. Patients and normal subjects were assigned to receive HBB (10 mg p.o. t.i.d.) for 24 h followed by a placebo for another 24 h or vice versa in a random manner. The results indicated that the number of reflux episodes was significantly greater with HBB in comparison with a placebo in patients with gastroesophageal reflux disease, and in normal subjects. The percentage of time with pH < 4, was also significantly greater in patients with gastroesophageal reflux disease and in controls; however, the mean 24-hour gastric pH after HBB was not different from placebo in gastroesophageal reflux disease nor in controls. Thus, the researchers concluded that hyoscine butylbromide is not to be recommended in the treatment of gastroesophageal reflux disease.
Renal Colic
Renal colic is usually the consequence of a calculus (stone) lodged in the ureter (or less commonly the bladder); the intense, colicky pain associated with this condition results from the intermittent spasmodic contractions of the obstructed hollow viscus, in an attempt to clear the blockage. It seems logical that an agent with the ability to diminish these spasms in the renal tract would be an effective analgesic, and several studies have been done to evaluate this.
Six studies involving a total of 755 patients have been identified, where hyoscine butylbromide has been evaluated as a co-analgesic (with morphine and indomethacin) versus placebo, 14 versus non-steroidal anti-inflammatory drugs (NSAIDs),15–18 and versus other antispasmodics. 19 In the study assessing HBB as a co-analgesic, 14 the administration of HBB was not shown to reduce initial opioid requirements, or the need for ongoing opioid analgesia. In contrast, the combination of HBB plus pethidine was shown to be superior to administration of diclofenac sodium alone, 15 although both were greater than 90% effective in pain relief 30 minutes after administration. Studies comparing HBB alone, to dipyrone and diclofenac, 17 and to dipyrone and tramadol 19 have shown efficacy of the drug in providing pain relief, but also demonstrated that its duration of action is reduced compared to the other medications. Similarly, studies comparing combinations of HBB and dipyrone to tenoxicam, 16 and to flurbiprofen 18 have consistently shown that the combination is effective in providing significant pain relief, although these latter studies suggested that the NSAID drugs acted slightly faster, and had a longer duration of action.
Thus, the evidence seems to indicate that HBB is an effective drug for use in the management of renal colic, either alone or in combination with opioids and/or NSAID analgesics, but that the onset of effect, and duration of analgesia with NSAIDs is superior to that of HBB.
Dysmenorrhea
Two recent studies were identified which looked at the effect of hyoscine butylbromide on primary and secondary dysmenorrhea. The first was a double blind crossover study comparing HBB and paracetamol to lysine clonixinate and proprinox, and to placebo. 20 A total of 120 women were studied, and both treatment arms showed a consistent decrease in subjective pain scores in the groups receiving them, as compared to placebo.
The second study was a longitudinal, open study, which evaluated a combination of lysine clonixinate and HBB, in three successive menstrual cycles of 30 women. 21 All women started with highly severe (10.7%), severe (42.9%), or moderate (46.4%) pain. At the end of the study only one patient reported the persistence of moderate pain.
Labor
Only one study was found which looked at hyoscine butylbromide primarily as an analgesic for the pain associated with labor. This study looked at 104 primigravidae in active labor, and showed that intravenous HBB provided pain relief of up to 36%, as compared to placebo. 22
Several authors investigated the drug as a labor accelerant, with the premise that if labor pain could not be reduced safely, then the time spent in labor (and, therefore, in pain) could be safely decreased. Five such articles were found, with three studies comparing the drug to normal saline or no drug at all,22–24 and one comparing it to another spasmolytic drug (drotaverine), 25 and the last comparing all three (HBB, drotaverine, and no drug). 26 The drug was given intravenously in four studies, in doses between 20 and 40 mg, and rectally in the other study. 23 A total of 533 women, divided almost exactly evenly, were assessed in the first four studies, with HBB being shown to cause a statistically and clinically significant reduction in the time from drug administration to delivery, with no significant adverse effects on either mother of neonate. In contrast, the last study which compared HBB to drotaverine and to no drug (50 patients in each group), showed no difference between the three groups, resulting in the conclusion that neither drug has any place in the augmentation of labor. 26 However, on the basis of the other positive studies, the strong claim by one researcher that HBB was ineffective in general might be questionable.
Procedure Related Discomfort/Pain
Hyoscine butylbromide has been studied with regard to its role in facilitating various investigations of the gastro-intestinal tract, and closely related structures.
Three studies were found which investigated the efficacy of HBB compared to that of placebo (2 studies; 208 patients), and to glucagon (1 study; 100 patients) for the purpose of sigmoidoscopy and/or colonoscopy. One study comparing the drug to placebo, clearly demonstrated a reduction in procedure time in the group receiving HBB. 27 In the study comparing HBB to glucagon, factors such as caecal intubation time, patient pain scores, and assessment of cardiovascular status were assessed. 28 This study showed that HBB was effective in inducing a reduction in peristalsis of the small bowel, with no difference in total procedure time or pain scores between patients in either group. However, both this and the third study documented statistically significant differences in hemodynamic changes in the HBB group (as measured by changes in heart rate and blood pressure), and the latter study also demonstrated a reduction in operator satisfaction with the procedure in the HBB group. 29 Consequently, glucagon was stated to be the favoured drug to facilitate colonoscopic examination.
Magnetic resonance imaging may be used to acquire high resolution images of the upper gastrointestinal tract, and hyoscine butylbromide has been examined in this context. A study done by Wagner et al 30 showed that intramuscular HBB administration significantly improves image quality of respiratory-triggered T2-weighted abdominal magnetic resonance imaging by persistent reduction of peristaltic artifacts. The study further stated that magnetic resonance imaging of the liver and pancreas in particular benefits from the suppression of gastrointestinal peristalsis by HBB. However, a subsequent study was done looking at the aperistaltic effect of HBB versus glucagon on the small bowel, also assessed by magnetic resonance imaging. 31 Baseline motility frequency, onset of aperistalsis, duration of arrest, reappearance of motility and return to normal motility were analysed. In this study, there were no significant differences in terms of baseline and end frequencies for the onset of aperistalsis, nor for the return to normal motility. However, aperistalsis was not achieved in 50% of cases with HBB treated patients (whereas it always was in the glucagon group), and the time of aperistalsis was significantly less in the HBB group, compared to the glucagon group (6.8 +/−5.3 min compared with 18.3 +/−7 min). Thus, glucagon was, once again, shown to be the superior agent, for this purpose.
Because of the wide scope for use of hyoscine butylbromide in the context of radiological investigations, a recent review of the literature was performed 32 and the following recommendations made to those administering hyoscine butylbromide:
Enquire whether there is an allergic history,
Ensure patient literature warns that “in the rare event that following the examination you develop painful, blurred vision in one or both eyes, you must attend hospital immediately for assessment”,
Warn patients to expect blurred vision and not to drive until this has worn off, and
Remind clinicians that special consideration needs to be given as to the method of investigating patients with cardiac instability, such as those recently admitted with acute coronary syndrome, recurrent cardiac pain at rest, uncontrolled left ventricular failure and recent ventricular arrhythmias.
Esophageal Obstruction
Two studies were found which compared the use of hyoscine butylbromide with no treatment, in the management of esophageal food bolus obstruction. In the first study, 33 82% of patients had the obstruction was relieved after being given HBB. Two had spontaneous relief >24 h later and two had surgical disimpaction. Where no medications were given, 78% cleared spontaneously and two had surgical removal. Fisher's exact test failed to show any significant difference between the two groups, but the authors conceded that not enough patients were included to make a definite judgement: in total, 29 patients were investigated, but about 280 would have been needed for a statistically sound result. The second study 34 showed that food bolus obstruction was relieved in 68% of the patients who had HBB and in 63% who did not have the medication. There was no statistically significant difference in both groups (P = 0.37). These authors concluded that the routine use of HBB in esophageal obstruction needs to be reviewed because of the lack of objective evidence of its efficacy, and that all treatment options need to be compared. A Cochrane review process on this issue has since been commenced.
Adjunctive Relief in Cancer Pain
More than two-thirds of patients with metastatic cancer experience pain. Relief of distressful symptoms in terminally ill patients is of prime importance, and a common practice is to administer opioid analgesics in conjunction with other drugs, such as hyoscine butylbromide, which is very useful in reducing secretions in patients with inoperable malignant bowel obstruction. Five studies were identified which looked at the stability of this drug in combination with other commonly used medications, such as tramadol, morphine, haloperidol, midazolam, metoclopramide, and dexamethasone.35–39 Out of 86 mixtures evaluated in vitro, 52 were found to be physically compatible, and 18 were administered to the patient population evaluated. HBB was found to be compatible with each of the individual drugs, and many drug combinations. Precipitation was always obtained when dexamethasone sodium phosphate was combined with haloperidol lactate and/or midazolam hydrochloride. 35 However, no precipitation occurred when morphine hydrochloride, the opioid most frequently used in patients of this type, and dexamethasone sodium phosphate were combined. Very good symptom control was obtained with all of them, and especially with the mixture of morphine + midazolam + haloperidol + HBB.
Conclusion
Hyoscine butylbromide is a generally safe and affordable drug with a wide scope of clinical applications. Evidence exists to support its use in the management of non-specific colicky abdominal pain (in adults and children); irritable bowel syndrome; labor and delivery; dysmenorrhea; as an adjunct in the therapy of late stage cancer patients with inoperable bowel malignancies; and to facilitate improved resolution in certain imaging techniques. It may also be useful in certain procedures, such as colonoscopy and sigmoidoscopy, and may be useful in the management of renal colic (although NSAIDs seem clinically superior). The oral form of the drug seems to be preferable for treatment of gastrointestinal disturbances, as it remains effective in the GI, but limits systemic side effects due to minimal absorption. The parenteral form is preferable for treatment of spasm in other systems, as there is greater bioavailability by these routes. The role of HBB in the management of esophageal food obstruction is unclear at this time; further studies need to be done.
Disclosure
The authors report no conflicts of interest.