
Abstract
Serotonin-type 3 receptor antagonists have been available as intravenous and oral formulations. Recently, granisetron transdermal system has won a firm position in the antiemesis of cancer chemotherapy. Its pharmacokinetic profile has been shown by pooled population analysis incorporation data. The 52 cm2 patch, which contains 34.3 mg granisetron, releases 3.3 mg daily and reaches the maximal plasma concentration after 48 hours, maintaining a 2.2 ng/mL stable average concentration over six days. This level is similar to the one obtained with daily oral 2 mg of granisetron. Three randomized clinical studies evaluating its efficacy have been published. Transdermal granisetron showed noninferiority to other formulations of serotonin-type 3 receptor antagonists for highly and moderately emetogenic – including multiday – chemotherapy. The adverse effects were not significantly different from other formulations. The system has possible applications in oral chemotherapy, radiotherapy, dexamethasone sparing, palliative care, and refractory emesis due to benign disease.
Keywords
Introduction
Problem of chemotherapy-induced nausea and vomiting
Chemotherapy-induced nausea and vomiting (CINV) is a nonhematological toxicity accompanied with cancer chemotherapy. Despite significant progress in its management, CINV continues to be among the most feared side effects in cancer patients receiving chemotherapy. 1 Uncontrolled CINV impairs patients’ quality of life, increases the use of health-care resources, and may occasionally compromise adherence.2,3 The control of CINV is very important for the success and efficacy improvement of cancer chemotherapy, avoiding some clinical complications, dose reduction, or delayed treatment.
Risk factors and classification of CINV
The risk of CINV is divided into two categories: patient-related factors and treatment-related factors. Two of the important patient-related factors are sex and age, with female and younger patients being at greater risk. 4 In addition, patients with a high pretreatment expectation of severe nausea are more likely to have nausea after chemotherapy. 5 Conversely, patients with a history of high alcohol consumption have a lower risk of CINV. 6 However, treatment-related factors such as chemotherapy dose and emetogenicity are the most predictive risk factors. 7 Intravenously administered chemotherapeutic agents are divided into four emetogenic levels: high (>90%), moderate (31%–90%), low (10%–30%), and minimal (<10%). 7 Percentages indicate vomiting risk with agents of each level in the absence of prophylactic antiemetic therapy. Recent evidence-based guidelines for preventing CINV reflect acceptance of this classification as the standard for defining the emetogenicity of chemotherapeutic agents. Additionally, radiotherapy is another important treatment-related factor. The irradiated site (upper abdomen) and radiation field size (>400 cm2) resulted as the most significant radiotherapy-related risk factors of radiotherapy-induced emesis. 8
Another important classification that leads to the specific therapeutic approaches is based on its temporal pattern of onset. 9 The temporal pattern of CINV is divided into three types as follows:
Acute CINV occurs during the first 24 hours after administration of chemotherapeutic agent.
Delayed CINV occurs from at least 24 hours, or later, after the administration.
Anticipatory CINV occurs before the administration, usually when CINV has been poorly controlled in previous chemotherapy course. This type of CINV is a conditional or learned response.10,11 The incidence of anticipatory CINV has reduced as antiemetic treatment advanced. Behavioral therapeutic approach should be preferable to pharmacological interventions.
Based on each treatment risk factor and temporal pattern of onset, different antiemetic drugs have been combined and the incidence and severity of CINV drastically reduced. 12 In contrast, the methodology of antiemetic prophylaxis considering patient-related factors remains controversial.
Pathophysiology of CINV
General mechanisms of CINV have been elaborated in a number of reviews.9,11 This section provides a brief overview of these reviews.
Emesis is the result of complex reflex mechanism, which involves certain neurotransmitters and their specific receptors in the central and peripheral nervous system. The emetic process is controlled by two areas in the brain: “the vomiting center” and the chemoreceptor trigger zone (CTZ). These areas receive and process the different emetic stimuli and also generate efferent signals to the respiratory, vasomotor, and salivary centers, as well to cranial nerves VIII and X, which results in emesis. 13 The CTZ is located in the area postrema in the floor of forth ventricle, outside the blood–brain barrier. 14 For this reason, substances with emetic potential circulating in blood or cerebrospinal fluid can activate the CTZ directly. The afferent pathway of the vagus nerve, activated by different gastrointestinal stimuli, is projected onto the nucleus tractus solitarius (vomiting center) and the area postrema (CTZ), provoking the efferent emetic reflex (Fig. 1). 9 Dopamine, opioids, histamine, acetylcholine, substance P, and serotonin are the main neurotransmitters involved in the stimulation of the central nervous system and in peripheral nerve fibers. Therefore, the pharmacologic emesis treatment is mainly aimed at blocking the specific receptors of these neurotransmitters.

Pathways by which chemotherapeutic agents produce emetic reflex. From N Engl J Med. Hesketh PJ. Chemotherapy-induced nausea and vomiting, 358:2482–94. Copyright © 2008 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Chemotherapy administration causes the release of mediators, mainly serotonin, through stimulation of the enterochromaffin cells of intestinal mucosa. These mediators bind to the specific receptors in vagal primary afferent neurons (Fig. 1). 9 The projection of vagal stimulus in the central nervous system (vomiting center and CTZ) triggers the emetic reflex. The most important neurotransmitters in CINV are serotonin, dopamine, and neurokinine-1 (NK-1) receptors, which bind substance P. 15 Another way of emesis activation may be the direct stimulation of CTZ by metabolites of chemotherapy or intestinal peptides circulating in the blood. This mechanism is considered possible and reasonable, but is yet to be fully demonstrated. 9
Brief review of selective serotonin-type 3 receptor antagonists and evidence-based recommendations for CINV prevention
The incidence of CINV has been reduced to 25% as antiemetic treatment advanced over the recent decades. 12 CINV prevalence could not be drastically reduced without selective serotonin-type 3 receptor antagonists (5HT3RA) such as granisetron, ondansetron, dolasetron, tropisetron, and palonosetron. They were confirmed superior to other antiemetic agents in meta-analyses. Between older 5HT3RA, except for palonosetron, no clinically relevant differences were demonstrated in efficacy.16,17 Newer 5HT3RA, palonosetron, shows a greater binding affinity for serotonin-type 3 receptor than older 5HT3RA, and prolonged half-life (approximately 40 hours).18,19 The efficacy of 5HT3RA for acute CINV was established in controlled clinical trials. Recently, a meta-analysis showed the superiority of palonosetron over older 5HT3RA for delayed CINV with moderately emetogenic risk. 20 For the management of emesis with highly emetogenic chemotherapy (HEC) and moderately emetogenic chemotherapy (MEC), highly qualified guidelines recommend 5HT3RA containing regimens:
HEC: Use a three-drug regimen combining 5HT3RA, dexamethasone, and NK-1 receptor antagonist to prevent acute CINV, and two-drug regimen combining the latter two drugs for delayed CINV.
MEC: Use a two-drug regimen combining 5HT3RA and dexamethasone to prevent acute CINV and either one of three drugs for delayed CINV12,21–24
Unmet needs in CINV treatment and transdermal granisetron
Until recently, intravenous and oral 5HT3RA had been available. At the approved doses, the oral formulation is therapeutically equivalent to the intravenous administration.7,21–24 However, older 5HT3RA showed much lower efficacy for delayed CINV 18 Delayed CINV remains a significant management problem even now. It occurs either as a result of reduced plasma concentration or inefficacy of ongoing oral antiemetic medication.2–4 A new formulation of a 5HT3RA (granisetron) delivered by transdermal route has been approved or made available in 12 countries and regions consisting of USA, Denmark, Finland, Germany, Italy, Netherlands, Norway, Sweden, UK, Taiwan, Hong Kong, and Singapore. Granisetron transdermal system (GTS) was developed to maintain effective plasma concentration for several days after chemotherapy. GTS has provided helpful alternatives to patients receiving HEC or MEC, including multi-day. It is expected to be effective in patients at risk of emesis induced by oral chemotherapy, radiotherapy, malignant bowel obstruction, and gastroparesis.
Mechanism of Action, Metabolism, and Pharmacokinetic Profile
Pharmacodynamics
The pharmacodynamic properties of granisetron are relatively well established and have been discussed in detail previously. This section provides a brief overview, including supplemented data from the U.S. manufacturer's prescribing information.25,26 Granisetron, an indozole, is chemically 1-methyl-
Pharmacokinetics
Granisetron metabolism includes
The GTS is supplied in the form of a 52 cm2 patch containing 34.3 mg of granisetron. It is composed of a transparent backing, a drug matrix (6% weight/weight), and a release liner. The patch releases granisetron 3.1 mg/day for up to seven days. Transdermal drug delivery is possible because the skin can absorb small, lipophilic molecules by passive diffusion. The pharmacokinetic properties of the GTS have been compared with those of oral granisetron in healthy male volunteers in a randomized, open-label, cross-over, phase I study.
28
Information is also available from a pooled population pharmacokinetic analysis, incorporating data from the phase I study (
Following patch application to intact skin, granisetron is slowly absorbed into the systemic circulation via passive diffusion. It avoids the plasma peaks and troughs associated with oral administration of granisetron, while still providing similar exposure. In the phase I study, pharmacokinetics of 52 cm2 granisetron patch was compared to that of daily oral 2 mg granisetron (Fig. 2 and Table 1).
28
Several differences are evident. The time at which maximum plasma concentration was achieved was 1.5–2 hours during oral dosing, and approximately the same maximum plasma concentration (
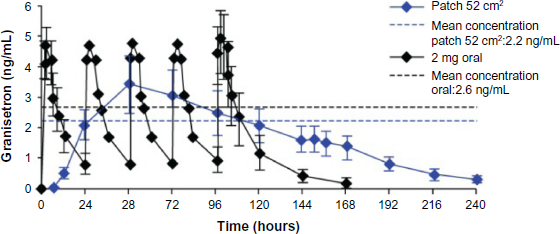
Granisetron plasma concentrations resulting from repeated oral and transdermal granisetron in a phase i study. Granisetron patch was removed at the end of day 6 (144 hours). From: Howell J, Clark G, Yellowlees A. J Oncol Pharm Pract. 15(suppl 2):20. Copyright © 2009 SAGE Publications. Reprinted by permission of SAGE Publications, Ltd.
Pharmacokinetic parameters of oral and transdermal granisetron in a phase I study. 29
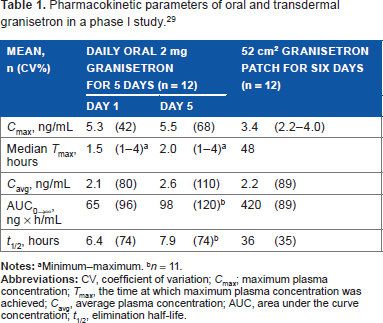
Minimum–maximum.
Clinical Studies
The efficacy and safety of GTS for CINV were evaluated in two randomized, double-blind, double-dummy, parallel-group, multicenter, premarketing studies: one was a phase II study (
Characteristics of published randomized controlled trials evaluating the efficacy of prophylactic transdermal granisetron.
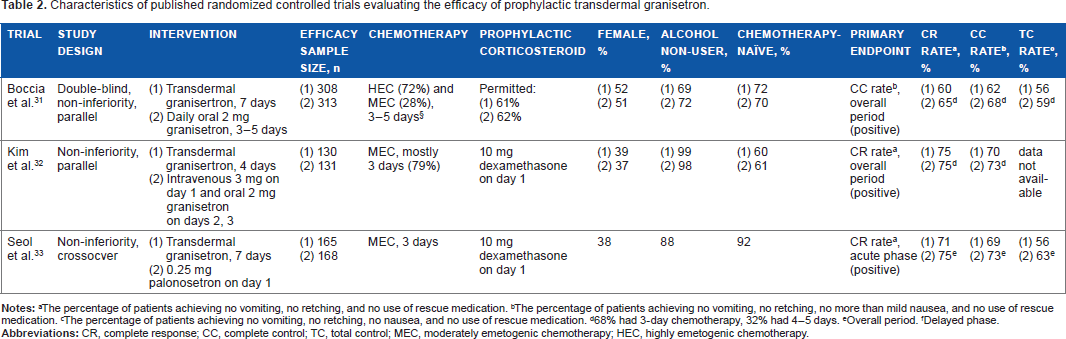
The percentage of patients achieving no vomiting, no retching, and no use of rescue medication.
The percentage of patients achieving no vomiting, no retching, no more than mild nausea, and no use of rescue medication.
The percentage of patients achieving no vomiting, no retching, no nausea, and no use of rescue medication.
68% had 3-day chemotherapy, 32% had 4–5 days.
Overall period.
Delayed phase.
Safety
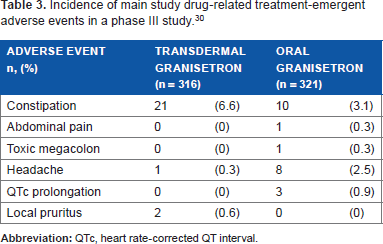
GTS was generally well tolerated in cancer patients receiving HEC and MEC (Table 3). In the premarketing phase III study, drug-related adverse events occurred in 7.9% of GTS recipients and in 5.6% of oral granisetron recipients. 30 The most common adverse event in both treatment groups was constipation. Constipation was reported more frequently by GTS recipients (6.6%) than in the oral granisetron group (3.1%). In contrast, headache was reported more frequently by oral granisetron recipients (2.5%) than by those in the GTS group (0.3%). Similar number of GTS and oral granisetron recipients (1.9%) withdrew from the study due to adverse events. Local skin tolerability of GTS was good. In the two phase III studies, two of 308 patients and one of 175 patients, or an average of 0.62%, developed skin irritation.30,31 No clinically significant electrocardiogram morphology changes were observed in either treatment course, and no cases of heart rate-corrected QT interval prolongation were identified in GTS recipients.
Incidence of main study drug-related treatment-emergent adverse events in a phase III study. 30
Efficacy
In patients receiving multiday HEC or MEC
GTS was found to be noninferior to intravenous and oral granisetron in the premarketing and Korean phase III studies.30,31 GTS controlled both acute and delayed CINV.
In the premarketing study in patients receiving repeated doses of HEC or MEC over three to five days, daily oral 2 mg of granisetron was given to 323 patients when chemotherapy was administered. 30 GTS was applied to 318 patients once 24–48 hours before chemotherapy and left in place for seven days. Over 70% of the patients received HEC. Similar number of patients received corticosteroids between treatment groups (data not reported). NK-1 receptor antagonist was not permitted – inconsistent with contemporary guidelines for HEC.12,21–24 Primary endpoint was complete control of CINV, which was defined as no vomiting, no retching, no more than mild nausea, and no use of rescue medication, from the first administration until 24 hours after last administration of chemotherapeutic agents. The complete control was achieved in 65% of patients in the oral granisetron group and 60% in the GTS group, which means no significant difference. Rescue medication use was different by the chemotherapy duration. With three-day duration, rescue medication was used equally in the two groups for delayed CINV. With four or five days’ duration, it was used more frequently in the GTS group. Patient global satisfaction scores were high and similar between both treatment groups. Mean visual analog scale was 8.2 cm for both groups.
In patients receiving MEC
In the Korean phase III study of patients receiving MEC, 137 patients were randomized to receive intravenous 3 mg of granisetron on day 1 and daily oral 2 mg on days 2 and 3. 31 GTS was applied in 139 patients once 24–48 hours before chemotherapy and left in place for four days. All patents received 10 mg dexamethasone intravenously on day 1. Over 70% of patients received three-day chemotherapy. Primary endpoint was complete response of CINV, which was defined as no vomiting, no retching, and no use of rescue medication, from the first administration until 24 hours after last administration of chemotherapeutic agents. The complete response was achieved in 75% of patients in the intravenous and oral granisetron group and in 75% in the GTS group, which means no significant difference. The complete response rate did not change after subgroup analyses by sex, age, chemotherapy naivety, analysis per day, and overall days of treatment. Patient Functional Living Index-Emesis scores also showed no difference. 33
Compared with palonosetron, GTS showed noninferiority in patients receiving MEC in another Korean cross-over phase IV study. 32 A total of 196 patients were randomized to 0.25 mg of palonosetron on day 1 and 7-day GTS. All patients received 5-fluorouracil and leucovorin with irinotecan (FOLFOX) or oxaliplatin (FOLFIRI) with intravenous 10 mg of dexamethasone on day 1. Most patients had gastrointestinal malignancies. Primary endpoint was complete response of acute CINV. It was achieved in 80% (134 of 168) of patients in the palonosetron cycles and 75% (124 of 165) of patients in the GTS cycles, which means no significant difference. The severity of CINV per day and total days of treatment was also not significantly different between the two cycles. A small number of patients in the GTS and palonosetron cycle had severe acute CINV, 3 of 175 patients and 1 of 173 patients, respectively. Patient Functional Living Index-Emesis scores showed no difference. 33
Loss of adhesion results in reduced drug delivery and can result in insufficiency. In the premarketing phase III study, 63% had ≥90% adhesion, 90% had ≥75% adhesion, and two patients (1%) had complete patch detachment. 30 In the other phase III study, 3 of 175 patients had complete patch detachment. 31 This low rate of complete patch detachment in these two phase III studies is impressive. Without organized data in medical literature against which to compare the adhesion success of GTS, detachment of at least 10% of the patch surface was noted in 36% of patients in the two phase III studies.
Patient Preference
Comfort, convenience, and compliance of patients are important and must be considered. GTS is the only antiemetic in the 5HT3RA group that can be used by patients unable or unwilling to use the oral or parenteral route. GTS can avoid venous manipulation required in chemotherapy, especially multiday. The patch is easy to apply and maintain during chemotherapy with mild skin problems if any. Especially in patients who do not swallow easily and in patients with complications such as mucositis, dysphagia, oral structural changes, and CINV (high-risk factors), GTS can deliver granisetron more reliably and less invasively than the parenteral route. The most important drawback of GTS is the need to apply the patch 24–48 hours before chemotherapy. It can cause unintended noncompliance and unnecessary exposure and increased expense in patients whose chemotherapy is unexpectedly delayed. Such delays, which may be required for a variety of diseases or drug-related comorbidities, are commonplace and usually initiated immediately before chemotherapy – well after the patch would have been applied. For example, at least one chemotherapy delay was reported in 45% (70 of 157) of patients treated with a platinum- and taxane-based regimen after cytoreductive surgery for ovarian cancer. 34 A potential workaround to avoid unnecessary deployment of GTS is to administer oral or parenteral granisetron on the day of chemotherapy and apply GTS on the same day.
Patients with severe dermatitis, itching, perspiration, or exercise habit to receive direct natural or artificial sunlight are not good candidates for GTS, because these patients would have to protect the patch from water, motion stress, and sunlight. Patch detachment may lead to decreased granisetron blood levels. Based on the result of an in vitro study, direct sunlight or sunlamps during and after 10 days of the patch removal may cause skin photogenotoxicity. 26
Place in Therapy
GTS has an important role in preventing CINV. It is a unique formulation with a number of advantages related to its delivery. Perhaps its greatest advantage is the ability to deliver an effective dose of granisetron over at least five days, without producing supratherapeutic concentrations that could cause adverse effects. This property makes GTS effective in prevention of not only acute but also delayed CINV without repeated administration. Additionally, it has been shown to have a much lower potential for inducing QT prolongation in comparison to two of the other drugs in the 5HT3RA group, dolasetron and ondansetron.35,36
GTS is effective and safe in preventing CINV with HEC and MEC for three to five days. The efficacy and safety are noninferior to those of oral and intravenous granisetron or intravenous palonosetron. It is expected to be used for relatively long-term prevention of emesis in radiotherapy and oral chemotherapy. For radiotherapy-induced emesis, American and European guidelines recommend prophylactic granisetron for patients with mild-to-high risk of irradiation site. Patients who receive radiation therapy in body trunk are all included in this risk category.21,23
Can GTS possibly take the therapeutic position of palonosetron? The answer is still unclear. In the two Korean studies, patients had relatively low CINV risk. Almost no regimens contained carboplatin, and only few regimens in the phase III study contained irinotecan.31,32 Carboplatin and irinotecan have high emetogenicity in MEC. Female rate was also relatively low in the two studies. It is thus not clear whether GTS has the same effect in MEC with high patient- or treatment-risk factors. In fact, GTS had numerically lower complete response, complete control, and total control rates compared with palonosetron in almost all evaluation periods. 32 Further study with GTS, palonosetron, and NK-1 receptor antagonist is needed to evaluate the efficacies in MEC, especially with high CINV risk factors.
Regarding dexamethasone sparing, GTS will certainly play a role in MEC. Using palonosetron, dexamethasone on days 2 and 3 can be spared in MEC with low patient-related CINV risk factors.37–41 Showing noninferiority to palonosetron in MEC, GTS will presumably allow for dexamethasone sparing. 32 The sparing may reduce its side effects such as oral and esophageal candidiasis, hyperglycemia, prolongation of chronic viral hepatitis, glaucoma, osteoporosis, moon face, and polytrichosis.
GTS is apparently less expensive than intravenous palonosetron. This is an important advantage to select GTS over palonosetron. In contrast, GTS is more expensive than other 5HT3RA and its generics. It is desirable to select the best 5HT3RA based on CINV risk factors, its estimated period, patients’ preference, and their financial situation.
GTS may also be useful in controlling emesis related to both benign and malignant disease. GTS was effective in reducing refractory emesis from gastroparesis in 50% (18 of 36) of patients. 42
Conclusion
GTS has a firm position in CINV prevention, especially multiday, due to its specific pharmacokinetic profile, providing stable serum granisetron level for over five days. Although new formulations of existing drugs and new chemical entities are under development, GTS will likely retain its firm position for the foreseeable future. It also has possible applications in oral chemotherapy, radiotherapy, dexamethasone sparing, palliative care, and refractory emesis due to benign disease. Further study is needed to evaluate the efficacy in combination with NK-1 receptor antagonist and in patients with other backgrounds. Also of interest is how GTS pharmacokinetics affects the pharmacodynamics, and how the single-peak, sustained GTS pharmacokinetics affects its efficacy compared to the reduced peak–tail fluctuations of long-acting palonosetron. Whether we should select GTS or palonosetron in HEC or high-risk MEC is the next clinical question to be answered.
Author Contributions
Wrote the first draft of the manuscript: HK. Contributed to the writing of the manuscript: HK. Agreed with manuscript results and conclusions: HK. Jointly developed the structure and arguments for the paper: HK. Made critical revisions and approved the final version: HK. The author reviewed and approved the final manuscript.
Footnotes
Acknowledgment
The author would like to thank Mr. David Hochman for reviewing the language of our article.