
Abstract
Objective
To examine the association between body mass index and time to conception.
Methods
Secondary data analysis of The Asthma in Pregnancy Study, a Prospective cohort of 2205 women assembled from April 1997-June 2000.
Results
Time to conception in women not on contraception, by BMI category, did not show a significant difference among the groups, p = 0.81 for test of equality over the strata.
Conclusions
No association between time to conception and BMI was demonstrated in these data.
Introduction
During the past twenty years, the prevalence of obesity among adults in the United States has risen significantly. (Ogden) Results from the National Health and Nutrition Examination Survey (NHANES) 2003-2004 showed that approximately 66% of U.S. adults age 20 and are either overweight (Body Mass Index, BMI, 25-29.9 for adults) or obese (BMI > 30 for adults). The NHANES data also demonstrate that there has been an increase in the proportion of obese adults, from 15% between 1976-1980, to 32% in 2003-2004. (Flegal) These increasing rates are a cause for concern given the health implications: obese adults are at greater risk for hypertension, type II diabetes mellitus, coronary heart disease, stroke, gallbladder disease, sleep apnea, and estrogen dependent cancers. Abdominal/visceral fat in particular predisposes to the metabolic syndrome, characterized by accelerated atherogenesis and insulin resistance. (Vasan)
There is an association between higher BMI and poor pregnancy outcomes: higher risks for miscarriage, gestational diabetes, hypertensive disorders of pregnancy, fetal macrosomia, and a higher rate of congenital anomalies such as neural tube defects accompany elevated maternal BMI. (Villamor) These births also eventuate in a higher cesarean section delivery rates, with resultant postoperative infections, and higher maternal death rates. (Dietz)
An increased body mass index (BMI) may alter fertility via several established biochemical mechanisms:
Increased volume of distribution contributed by adipose tissue, with respect to either endogenous or exogenous steroidal hormones, and storage of lipid soluble steroids, leading to decreased free hormone levels. (Pasquali)
Changes in metabolism and excretion of hormones, or altered production of steroid hormone binding proteins such as sex hormone binding globulin.
Alterations/polymorphisms of estrogen and/or insulin receptors, such as those involved in the pathophysiology of polycystic ovarian syndrome.
Enhanced peripheral conversion of adrenal androgens to additional estrogens, via adipose tissue aromatase, 3β-dehydrogenase, and 17β-hydroxydehydrogenase activity. (Speroff)
Clarification of the potential relationship between BMI and desired/planned fertility could alter the treatment recommendations for a significant proportion of the 10% of US women that currently require fertility treatments to achieve a desired pregnancy, (Zhu) as well as the study of potential associations of oral contraceptive failure rates with obesity (Brunner-Huber).
Methods
The Asthma in Pregnancy Study was a prospective study, which collected data from April 1997-June 2000 (Bracken). It was designed to examine the relationship between maternal asthma, asthma symptoms/therapy, and pregnancy outcomes of fetal growth and gestational age at delivery. 2,205 pregnant women were recruited from 15 clinics and 56 obstetric practices in CT and MA, prior to 24 weeks of gestation. Demographic information, pregnancy history, and self-report measures of potential con-founders such as smoking and alcohol consumption were included in the questionnaire. Last method of contraception used, date of last use, and number of months between contraceptive use and pregnancy was recorded. Pregnancy outcomes were abstracted from obstetric records. Demographic information, such as race-ethnicity, marital status, years of education, and annual household income, was included, as well as possible confounding variables: self-report age, weight, height, gravidity, parity, duration of OCP use, frequency of sexual activity, exercise frequency in the year prior to pregnancy, alcohol, and tobacco use. Age was categorized into a 3 level variable: 15-24, 25-34, and 35-44 years. BMI was categorized according to WHO and NIH criteria: underweight < 18.5 kg/m2, normal weight was defined as a BMI of 18.5-24.9, overweight as 25-29.9, and obesity as > 30. (Catalano)
Inclusion criteria were a previous pregnancy reported as live birth, stillbirth, abortion, or miscarriage, assuring proven fertility, in order to minimize confounding by factors such as fallopian tube scarring or oligo-spermia in the male partner.
Exclusions were antecedent ectopic pregnancy, as the majority of such conceptions are secondary to tubal disease, which could confer decreased fertility.
55 women were further excluded for missing height, weight, demographic or covariate information. Total subjects for analysis were 362.
Using SAS (version 9.1) software, bi-variate associations were determined, using X2 tests of significance for categorical variables and t-tests for continuous variables. Kaplan-Meir curves were generated to analyze time to conception in those not using contraception in the year prior to pregnancy, to examine the hypothesis that a delay in conception may be secondary to elevated BMI. (Hatch). Hazard ratios (HR) for WHO categories of BMI and conception were calculated using Cox Proportional Hazard regression analysis.
Results
The respondents had a mean age of 28.9 years, mean weight at conception of 147.9 pounds, and mean weight at the time of interview of 154.4 pounds, mean height of 64 inches. 67.7% were married, 28.3% never married, 2% divorced, 1.7% separated. Race-ethnic groups were 66% white, 9.6% black, 1.3% Asian, 17.1% Hispanic, 2% Black/Hispanic, and 4% other. 54.4% exercised 4-6 times a week, 9.6% once a day. Annual household incomes were skewed to above $60,000. 58.9% had sexual activity at least once a week, 48.5% at least twice per week. (Table 1) Mean time to pregnancy was 5.83 months. 22.7% were obese.
Description of the sample a

Table values are mean ∓SD for continuous variables and n (column%) for categorical variables.
Numbers may not sum to total due to missing data, and percentages may not sum to 100% due to rounding).
Kaplan Meir curves of time to conception, by BMI category, did not show a significant difference among the BMI groups, p = 0.81 for test of equality over the strata. The mean number of months to pregnancy predictably was less for those in the lowest age category 15–24 years, 1.9 months (1.5–2.5) p = 0.06, but did not differ by smoking status, pre-pregnancy exercise, or any of the other variables examined. (Table 2 and Figs. 2–4) Cox proportional hazard regression, controlling for age, smoking, and exercise, also failed to find an association between BMI and time to conception. Smoking showed the only significant relationship, with a hazard rate of 2.44, p = 0.03.
Time to pregnancy analysis.

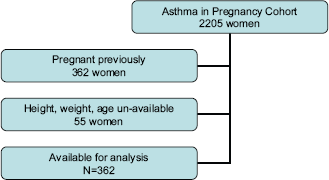
Selection of study sample.
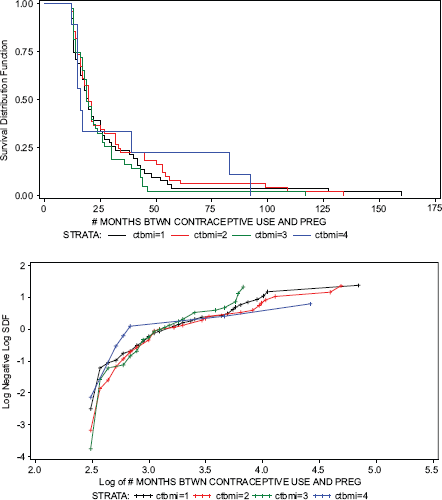
Time to pregnancy by BMI category.

Time to pregnancy by age category.
Discussion
The recall validity of time to pregnancy has been found to be high. (Zhu) Although retrospectively assessed, differential recall between BMI categories is unlikely. Residual confounding could have occurred if other hindrances to conception, such as undiagnosed pelvic infection, had occurred in the preceding inter-pregnancy interval. Losses to follow up and time to events are likely to be nondifferential between BMI categories. The dichotomous exposure assessment of smoking precludes the calculation of a dose-response relationship. A history of cigarette smoking has been found to be associated with increased serum testosterone (Barbieri).
The sample, which is composed primarily of White, college educated, affluent women, might not be generalizable to other populations.
Obese women are reported to have a higher prevalence of amenorrhea and infertility, yet the underlying biologic mechanism remains largely unexplained. Obesity represents a state of sexhormone imbalance, as levels of SHBG decrease linearly with percentage of body fat, leading to increased free androgen levels. Adipose tissue also releases leptin and adiponectin, which are associated with hyper-insulinemia, reduced GH levels, and increased testosterone production, especially in the presence of abdominal as compared to peripheral, distribution of obesity. PCO is associated with abdominal obesity even among women with normal BMI. (Pasquali) Inclusion of waist circumference in addition to BMI as a predictor variable might therefore enhance the ability to detect an association between exposure and outcome of interest. No studies have been completed measuring these covariates in relation to BMI/fecundability.
Cox proportional hazard regression analysis 1
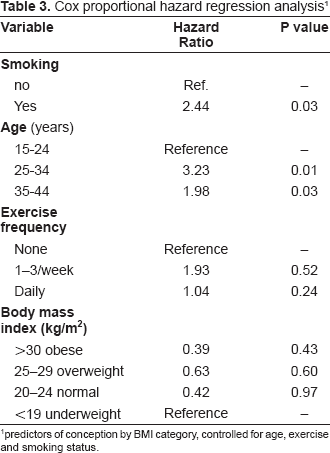
predictors of conception by BMI category, controlled for age, exercise and smoking status.
Polycystic ovarian syndrome (PCO), the commonest cause of anovulatory infertility, is estimated to affect only 4-7% of women overall. 35-40% of women with PCO are obese; 50% of overweight women have PCO compared to 30% of lean women. (Yu) In these cases, insulin resistance is associated with hyper-androgenism, elevated IGF production by the liver, pituitary down-regulation by chronically elevated estrogen levels, and consequent anovulation.
Obesity susceptibility factors such as PCO, should be statistically modeled as exposure-effect modifiers of the potential association between BMI and fertility/infertility. This would require measurement of validated biomarkers such as serum free androgens, estradiol, LH, insulin, TSH, pro-lactin, and glucose, adding considerably to the expense of study. Even these parameters may not accurately reflect the steroid tissue pool residing in adipose tissue. Obesity may be a surrogate marker for the metabolic perturbations of this syndrome, or an indication of cumulative exposure, rather than an independent risk factor. Cross sectional study cannot provide information about the temporal sequence of exposure. (Hayes)
Genetic heritability is estimated to account for between 30-70% of the expression of BMI in adult life. (Bell) Molecular or genetic epidemiologic linkage studies may prove to be superior for the identification of common markers of obesity and fertility/infertility exposure, susceptibility, and outcome, such as those chromosomal regions coding for estrogen receptors, leptin, adiponectin, and insulin receptor polymorphisms. (Rankinen)
This population-based study found no association between obesity and time to conception. Misclassification or uncontrolled confounding may obscure a true relation. A large, prospectively collected data set, with clearly defined standardized methods, and consistent definition and characterization of BMI categories, is needed to adequately determine the magnitude and direction of any true association.

Time to pregnancy by pre-pregnancy exercise frequency.