
Abstract
The gonadal arteries normally arise from the abdominal aorta. There are reports about the variant origin of these arteries. In the present study, we investigated the origin and course of the gonadal arteries and clinical implications of variant gonadal arteries are discussed. Out of 60 dissections, in 55 cases the gonadal artery was seen arising from abdominal aorta. In the remaining 5 cases, gonadal artery of renal origin was present in 3 cases, two on right and one on left side and of middle suprarenal origin was present in 2 cases on the left side. The present study agreed with the text book account i.e. right testicular artery passing anterior to inferior vena cava in majority of the cases i.e. 27 (90%). In the remaining 3 cases (10%), the right testicular artery was posterior to inferior vena cava. In our study, out of a total of 60 dissections, 57 dissections confirmed to type I pattern (95%). In 2 cases (3.3%) (11 M, 16 M) a type II pattern was seen on the right side. In 1 case (1.7%) (20 M), the left testicular artery arose directly from the aorta and arched over the renal vein giving a type III pattern. Awareness of variations of the testicular arteries such as those presented here becomes important during surgical procedures like varicocele and undescended testes. The variations described here are unique and provide significant information to surgeons dissecting the abdominal cavity.
Introduction
Variations in the origin of arteries in the abdomen are very common but with the invention of new operative techniques within the abdominal cavity, the anatomy of abdominal vessels has assumed much more clinical importance. The gonadal arteries arise from the front of the aorta, usually 1-2 inches (2.5-5 cm) below the renal arteries. These arteries are small and variable in their origin.
In the male, the arteries diverge from each other and pass laterally over the front of the psoas major muscle in a retroperitoneal position. Each artery crosses in front of the corresponding ureter giving a branch to it. The right artery runs behind the terminal portion of the ileum, while the left one passes behind the sigmoid colon. The artery skirts the pelvic brim, and crosses anterior to the distal end of external iliac artery to enter the internal inguinal ring. 1 Then it accompanies the ductus deferens through the inguinal canal to the testis. 2
The ovarian arteries diverge slightly less than the testicular arteries but have a similar downward and lateral course in their upper portions. Each artery crosses anterior to the ureter of its side and often supplies a ureteric twig. It enters the pelvis by crossing the common or external iliac artery. 1 It then passes between layers of suspensary ligament of the ovary to reach the broad ligament of the uterus. Them it runs medially below the uterine tube and turns backwards into the mesovarium where it breaks up into branches which enter the ovary at the hilus. 2
In 5%-20% of cases, the gonadal artery has a high origin (superior to L2) and in 5%-6% of cases it originates from the main or accessory renal artery. The latter is referred to here as an aberrant gonadal artery. 3
In the present study, we investigated the origin and course of the gonadal arteries and clinical implications of variant gonadal arteries are discussed. Awareness of variations of the gonadal arteries such as those presented here becomes important during surgical procedures like varicocele and undescended testes. A gonadal artery with origin from an inferior polar renal artery may be injured during the percutaneous treatment of the syndrome of pielo-ureteral junction, so it becomes a major contraindication. Also, this anatomical variation enhances the importance of the arteriography or Doppler ultrasound examination of the renal hilum. Sometimes, the gonadal artery may pass posterior to the proximal ureter that can be disturbed in traject, leading to hydronephrosis. As the number of abdominal surgical interventions and radiological investigations increase, a better understanding of the anatomy of gonadal arteries gains importance.
No other variation in any abdominal organ or abdominal vasculature was noticed during the dissection.
Material and Methods
The material for this study comprised of 30 well embalmed adult human cadavers of known sex obtained from the Department of Anatomy, Govt. Medical College, Amritsar. They were serialized from 1-30 with suffix ‘M’ for male and ‘F’ for female.
The abdominal cavity was opened by a cruciform incision passing through the whole thickness of the anterior abdominal wall. Flaps were reflected. The abdominal viscera i.e. stomach, intestines liver, pancreas and spleen were systematically removed according to Cunningham's Manual of Practical Anatomy. 4
The abdominal aorta was cleaned along its whole length and the origin of various branches was traced. Parietal peritoneum on posterior abdominal wall was reflected and the gonadal vessels were exposed and cleaned. The relation of gonadal artery to inferior vena cava was observed. The origin and course of gonadal arteries together with variations in the arteries were discussed and compared with available literature.
Comparison of the vertebral level of origin of gonadal arteries.

Our study is thus in complete corroboration with Cauldwell and Anson. 6
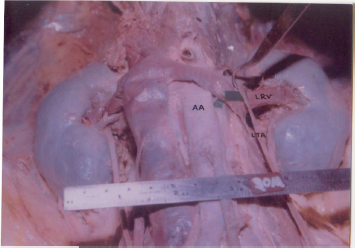
Left testicular artery (LTA) arching over left renal vein (LRV).
Results
Variations in the testicular or ovarian arteries in relation to renal pedicle are important as it may cause compression of the renal vein resulting in obstruction of the blood flow from the kidney and gonadal glands. 5
Origin
Vertebral level
In the present study, the vertebral level of origin of the artery ranged from the disc of L1 and L2 to upper 1/3rd of the L3 vertebra on the right side and between upper 1/3rd of L1 to upper 1/3rd of L4 vertebra on the left side.
Source
Variation in the origin of gonadal arteries in the present study showed no significant difference between male and female as also observed by Notkovich. 5 Out of 60 dissections, in 55 cases the gonadal artery was seen arising from abdominal aorta. In the remaining 5 cases, gonadal artery of renal origin was present in 3 cases, two on right and one on left side and of middle suprarenal origin was present in 2 cases on the left side. Gonadal artery arising from coeliac trunk or superior mesenteric artery was not observed in the present study; an observation reported by Merklin and Michels. 7
The incidence of gonadal artery arising from renal artery was thus 10.0%, comparable to the range falling between 3% to 16.1% as reported by previous workers (Table 2). Bremer 8 explained that the spermatic branches of renal origin were due to an early connection of a mesonephric artery with the kidney, which is normally lost.

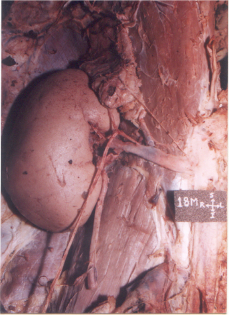
Left testicular artery (LTA) arising from the aberrant left renal artery (AbLRA).
Relation of right testicular artery to inferior vena cava
The present study agreed with the text book account i.e. right testicular artery passing anterior to inferior vena cava in majority of the cases i.e. 27 (90%). In the remaining 3 cases (10%), the right testicular artery was posterior to inferior vena cava. This reversal of relation is explained by Notkovich 5 on the basis that usually the lateral splanchnic artery persists on the right side and passes caudal to supracardinal anastomosis which forms a part of inferior vena cava when it passes cranial to this, the right testicular artery comes posterior to inferior vena cava.
Comparison of the prevalence of gonadal arteries of renal origin.

Right testicular artery (RTA) taking origin from right inferior suprarenal artery (RISA).
The course of gonadal artery has been grouped into 3 types of Notkovich 5 in relation to renal pedicle as:
In our study, out of a total of 60 dissections, 57 dissections confirmed to type I pattern (95%). In 2 cases (3.3%) (11 M, 16 M) a type II pattern was seen on the right side. In 1 case (1.7%) (20 M), the left testicular artery arose directly from the aorta and arched over the renal vein giving a type III pattern. This type III variation has previously been reported by Pick and Anson, 9 Notkovich 5 and Anson and Kurth. 10
The internal spermatic artery in 1 case (10 M) was double on the left side in the current study. As also observed by Cauldwell and Anson 6 in 10.3% cases who explained the multiplicity of gonadal arteries to be due to the persistence of more than one branch to the gonads.

Double testicular artery (TA1, TA2) seen on left side with superior testicular artery (TA1) taking origin from inferior renal artery (RA2) and the inferior testicular artery (TA2) arising directly from abdominal aorta (AA).
Discussion
The anatomy of the gonadal arteries has assumed importance because of the development of new operative techniques within the abdominal cavity for operations such as varicocele and undescended testes 11 During laparoscopic surgery of the male abdomen and pelvis many complications are due to unfamiliar anatomy in the operative field. 12 Thus it becomes imperative to carefully preserve the gonadal artery in order to prevent any vascular troubles of the gonad, the genital artery being its unique source of blood supply. All these indicate the importance of the arteriography or Doppler ultrasound examination of the renal hilum, prior to any surgical procedure within the region. 13
The variations of gonadal arteries are common and have been reported. The testicular artery may vary at their origin, they may be absent or may be doubled, tripled or quadrupled. 14 An additional left testicular artery has been reported by Loukas and Stewart 15 The anomalous origin of the testicular artery from the inferior polar artery of the kidney and its surgical importance have been reported by Ravery et al. 16 High origin of gonadal arteries from abdominal aorta have been reported in two individuals by Ozan et al. 17 Rusu 18 described a case of bilateral doubled testicular arteries with a left testicular arterial arch around the left renal vein. Naito et al 19 described two cases of the left testicular artery arching over the ipsilateral renal vein. Similar variation i.e. Type III course has been described in the present study in 1 case. Considering that the incidence of a left arching testicular artery is higher than that of a right one, an arching left artery could be an additional cause of left renal vein (LRV) hypertension) resulting in varicocele, orthostatic proteinuria and haematuria. The surgeons should take into account the aberrant origin and course of the gonadal arteries when operating near a renal pedicle or in the retroperitoneum. A deep knowledge of these variations and their relations to the adjacent structures is very important in avoiding the complications in operative surgery. With the advent of newer surgical and diagnostic techniques, understanding of atypical anatomical presentations gains more importance.
Publish with Libertas Academica and every scientist working in your field can read your article
“I would like to say that this is the most author-friendly editing process I have experienced in over 150 publications. Thank you most sincerely.”
“The communication between your staff and me has been terrific. Whenever progress is made with the manuscript, I receive notice. Quite honestly, I've never had such complete communication with a journal.”
“LA is different, and hopefully represents a kind of scientific publication machinery that removes the hurdles from free flow of scientific thought.”
Available to your entire community free of charge
Fairly and quickly peer reviewed
Yours! You retain copyright
Footnotes
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors report no conflicts of interest.