
Abstract
Capsule
Male aging effects on aneuploidy rates in embryos.
Objective
Paternal age is associated with decreasing sperm quality; however, it is unknown if it influences chromosomal abnormalities in embryos. The objective of this study is to evaluate if the aneuploidy rates in embryos are affected by advanced paternal age.
Methods
A total of 286 embryos, obtained from 32 in vitro fertilization/intracytoplasmic sperm injection cycles with donated oocytes in conjunction with preimplantation genetic diagnosis, were allocated according to paternal age in three groups: Group A: ≤39 years (n = 44 embryos); Group B: 40-49 years (n = 154 embryos); and Group C: ≥50 years (n = 88 embryos). Fertilization rates, embryo quality at day 3, blastocyst development, and aneuploidy embryo rates were then compared.
Results
There was no difference in the seminal parameters (volume, concentration, and motility) in the studied groups. Fertilization rate, percentages of zygotes underwent cleavage, and good quality embryos on day 3 were similar between the three evaluated groups. The group of men ≥50 years had significantly more sperm with damaged DNA, low blastocyst development rate, and higher aneuploidy rates in embryos compared to the other two evaluated groups (P < 0.05).
Conclusions
Our findings suggest that advanced paternal age increases the aneuploidy rates in embryos from donated oocytes, which suggests that genetic screening is necessary in those egg donor cycles with sperm from patients >50 years old.
Keywords
Introduction
In today's society, the assisted reproduction technology permits treating the majority of infertile couples, achieving satisfactory pregnancy and implantation rates. In the vast majority of in vitro fertilization (IVF) laboratories around the world, embryo selection is still based on the assessment of morphologic criteria during the preimplantation stage, such as number of pronuclear and polar bodies, cell size and number, evenness of mitotic divisions, multinucleation, amount of cellular fragmentation, extent of blastocoel expansion, and quality of inner cell mass (ICM) and trophectoderm (TE).1–4 However, it is now known that the embryo morphology does not always translate into high implantation rates,5,6 and thus, embryos achieving the best morphologic scores often fail to achieve implantation or do not produce a live birth.7–9 In many cases, the underlying cause of embryo arrest, implantation failure, or miscarriage is the presence of chromosomal abnormalities or aneuploidy, and now it is generally accepted to be the principal genetic factor that affects the human reproduction success.
The frequency of aneuploidies in human preimplantation embryos generated during IVF is estimated to be between 56% and 84%, 10 and its occurrence is related to maternal and paternal factors. The principal female factor include aging, which increases the risk of defects in maternal mRNA, disturbing the pool of proteins and mitochondrial function, and finally an incorrect chromosome segregation during cell division process. 11 Duncan et al 12 showed a reduced cohesion molecule concentration in older women (responsible for binding the sister chromatids together), which causes an unequal separation of chromosomes leading to aneuploidy. Additional factors include accumulation of free radical in the oocytes, exposure to radiation or chemicals, poor vascularization of antral follicle during oocyte maturation, and depletion of critical nutrients during cell divisions leading to chromosome fragmentation and aneuploidy.13–15 In the case of paternal factors leading to embryo aneuploidy, alterations in centrosome, which is composed of two centrioles and paternally inherited, may result in abnormal spindle formation and chromosome malsegregation. 16 Besides, the generation of aneuploid gametes during spermatogenesis and patients with oligoasthenoteratospermia or nonobstructive azoospermia (testicular sperm extracted) with severe sperm defects may result in a higher percentage of mitotic abnormalities and chaotic embryos. 17 In the past years, male aging has been associated with a decrease in serum steroid levels, testicular volume, progressive motility, daily sperm production, inhibin B/follicle stimulating hormone (FSH) ratio, alteration in testicular histomorphology, risk of chromosomal disorders,18,19 and a significant increase in spermatic DNA fragmentation, particularly in men >50 years.20,21 These changes related to aging are factors that can increase the risk of aneuploidy in embryos causing failure to obtain blastocysts, blockage in embryo development after implantation, increased risk of recurrent miscarriages, reduced chance of successful implantation, and negative effects on the health of the offspring.22–24
Oocyte donation is a successful and well-established treatment where the oocyte and subsequent embryo qualities are optimized by donated oocytes from young women, 25 eliminating the effect of maternal age and resulting in high pregnancy rates and good obstetrical outcomes observed in recipients.26,27 It is in this manner that oocyte donation represents an optimal model to study the influence of male aging on reproductive potential.
The aim of the present study is to evaluate the development capacity, embryo quality, and aneuploidy rates in embryos obtained from donated oocytes according to male age.
Materials and Methods
Study design
This is a retrospective nonrandomized study conducted on 286 embryos obtained from 32 IVF/intracytoplasmic sperm injection (ICSI) cycles with oocytes donated in conjunction with preimplantation genetic diagnosis (PGD; IVF: n = 14; ICSI: n = 18). The procedures were done at FERTILAB Laboratory of Assisted Reproduction between January 2012 and August 2015. Written informed consents were obtained from all recipients, and their partners were included in this study to share the outcomes of their cycles for research purposes. This study was approved by the Institutional Review Board and the corresponding Ethics Committee from Clínica Oncogyn.
Thirty-two anonymous oocytes donors (21-28 years old) were subjected to physical, gynecological, and psychological examinations, and there was no family history of hereditary or chromosomal diseases. All participants had a normal karyotype and tested negative in a screening for sexually transmitted diseases. The recruitment of oocyte donors was done based on the recommendations given by other donors, and the donation of their gametes was merely by altruistic reasons.
Ovarian stimulation and oocyte collection
Donors’ menstrual cycles were stimulated using recombinant FSH (Gonal®) according to the previously established stimulation protocols. 28 Medication was started on day 2 of the menstrual cycle until at least three follicles reached ~18 mm in diameter. Oocytes were collected 36 hours after human chorionic gonadotropin administration (Pregnyl®) by transvaginal ultrasound ovum pickup. During the follicular aspiration procedure, oocytes were recovered in Global® HEPES-buffered medium (LifeGlobal) supplemented with 10% volume/volume (vol/vol) Serum Substitute Supplement (SSS; Irvine Scientific). After retrieval, cumulus–oocyte complexes were manually denuded from cumulus cells using sterile needles and cultured in ~200 μL drops of Global® Fertilization medium (LifeGlobal) plus 10% SSS under oil at 37°C and an atmosphere containing 6% of CO2, 5% of and 89% of N2 for five hours before the IVF/ICSI procedure.
Insemination, fertilization, and embryo culture
The recovered oocytes were assessed for their nuclear maturity, and only metaphase II oocytes were submitted to IVF/ICSI. The insemination was made with 50,000-100,000 motile spermatozoa in ~200 μL drops of Global® Fertilization medium + 10% SSS, where one to five oocytes were placed. In the cases of ICSI, all collected oocytes were denuded enzymatically off cumulus cells with hyaluronidase (80 IU/mL; LifeGlobal) and injected following the routine procedures. 29
Normal fertilization status, indicated by the presence of two pronuclei, was evaluated for 16-18 hours after IVF/ICSI. The zygotes were individually cultured under mineral oil, in 10-μL droplets of Global® medium (LifeGlobal) supplemented with 10% vol/vol SSS until day 3 when the embryos were moved to fresh 10-μL droplets of Global® medium + 10% SSS and cultured for two more days up to blastocyst stage. On day 3, the embryos were evaluated for cell number, fragmentation, and multinucleation, and on day 5, they were evaluated for blastocyst development and expansion. Good quality day 3 embryos were defined as those with six to eight cells and ≤10% of fragmentation. Good quality blastocysts were defined as having an ICM and TE type A or B. 30
Embryo biopsy, fixation, and FISH analysis
On the third day after insemination, one cell per embryo was biopsied following a protocol described elsewhere. 31 Individual embryos were placed into calcium/magnesium-free media (PGD Biopsy Medium; LifeGlobal) through a hole of the zona pellucida opened with Tyrode's acid solution; one nucleated blastomere was removed by aspiration. After biopsies, the embryos were rinsed thoroughly and returned to culture under mineral oil, in 10-μL droplets of Global® medium (LifeGlobal) supplemented with 10% vol/vol SSS.
Blastomeres were fixed individually following the routine protocols to minimize signal overlap and loss of micronuclei. 32 PGD analysis was performed by FISH using probes specific for 12 chromosomes 8, 13, 14, 16, 18, 20, 21, 22 (Abbott Laboratories), X, Y, 15, and 17 (Cellay Inc.) following the manufacturer's instructions.
Sperm collection
Semen samples were collected by masturbation after three to five days of abstinence and on the day of oocyte retrieval for ICSI. Semen analysis was performed according to World Health Organization (WHO) criteria. 33 After semen liquefaction, motile spermatozoa were separated from the seminal plasma by centrifugation at 300 × g for 10 minutes through 1.0 mL 95% and 45% Isolate gradients (Irvine Scientific). The pellet was washed once by centrifugation for five minutes and was resuspended in 0.1 mL of Global Fertilization medium + 10% SSS for IVF/ICSI.
Sperm DNA fragmentation assessment
Prior to the hormonal stimulation, sperm DNA fragmentation values were evaluated with the sperm chromatin dispersion test 34 using the Halosperm® Kit (Halotech DNA). Briefly, sperm samples from each patient, with a concentration not <5 million and not >10 million spermatozoa per milliliter, were used. The kit contains aliquots of agarose gel in Eppendorf tubes. Each semen sample was processed after the agarose gelled (from immersion in a water bath at 90°C for five minutes). When the Eppendorf tubes reached a temperature of 37°C (five minutes at 37°C in a dry atmosphere), 25 μL of sperm were added and gently mixed. Twenty microliters of this mixture were placed on precoated slides and covered with 22 × 22-mm coverslide. The slides were maintained at 4°C for five minutes to produce a microgel containing embedded spermatozoa. The coverslides were gently removed, and the slides were immersed in a previously prepared acid solution (80 μL of HCl added to 10 mL of distilled water) for seven minutes. After removal from this solution, the slides were incubated for 25 minutes in 10 mL of lysing solution (provided in the Halosperm kit). After rinsing in distilled water, the slides were dehydrated for two minutes in three concentrations of alcohol (70%, 90%, and 100% vol); each and either were stored (storage was possible several months in optimal conditions) or were processed immediately with staining solution for 10 minutes with continuous airflow. Staining was performed with 1:1 (vol/vol) by using Wright's solution (Merck) and phosphate-buffered saline solution (Merck). The slides were rinsed in tap water, allowed to dry at room temperature, processed for upright or inverted bright-field microscopy at 100×, and covered with 22 × 22 coverslide. Operators scored ≥500 spermatozoa for each patient according to the patterns established by Fernández et al 34 Strong staining is preferred to visualize the dispersed DNA loop halos. Removal of sperm nuclear proteins results in nucleoids with a central core and a peripheral halo of dispersed DNA loops. The sperm tails remain intact. The acid treatment produces DNA unwinding that is restricted in those nuclei with high levels of DNA strand breakage. After the subsequent lysis, sperm nuclei with fragmented DNA produce very small or no halos of dispersed DNA. However, nuclei without DNA fragmentation released their DNA loops to form large halos.
Statistical analysis
Statistical analysis was carried out using the statistic package Stata 10 (StataCorp). Data were represented as mean ± SD. Group comparisons were made using the χ2 test and Student's t-test. It was considered a statistical significant difference when P < 0.05.
Results
Results of chromosomal status from 286 biopsied embryos were allocated to three groups according to paternal age as follows:
≤39 years (range 34-39 years; n = 5)
40-49 years (range 40-47 years; n = 17)
≥50 years (range 50-72 years; n = 10)
There was no difference in the age of oocyte donors (22.7 ± 1.53, 24.2 ± 1.74, and 24.1 ± 1.85 years), days of stimulation (8.4 ± 1.14, 8.9 ± 1.11, and 8.3 ± 1.06), and mean of recombinant FSH treatment (1345 ± 329.96, 1363.2 ± 288.61, and 1385 ± 290.64 IU/mL) between the three evaluated groups (data not shown).
The results of the basic semen parameters and sperm DNA fragmentation according to male age are presented in Table 1. Our data showed that men ≥50 years old had significantly high percentages of sperm with fragmented DNA (37.1 ± 17.61% versus 17.4 ± 10.79% and 21.3 ± 13.48%; P < 0.05). Values of semen volume, sperm concentration, and progressive motility were similar in the three evaluated groups (P = not significant). According to WHO (2010) criteria, men ≥50 years old had significantly less sperm with normal morphology (4.7 ± 3.51°% versus 11.3 ± 4.88% and 7.9 ± 3.99%) compared to men from groups ≤39 years old and 40-49 years old, respectively (P < 0.05).
Comparison of seminal characteristics between three evaluated groups.
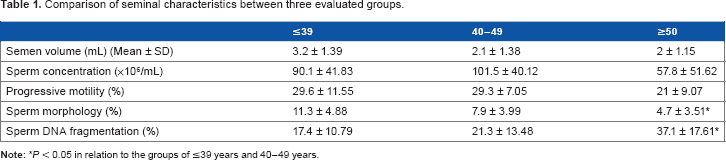
P < 0.05 in relation to the groups of ≤39 years and 40-49 years.
Results of laboratory and preimplantation genetic screening (PGS) from evaluated groups are summarized in Table 2. A total of 58, 207, and 131 oocytes were inseminated from the groups of ≤39 years, 40-49 years, and ≥50 years, respectively. There was no difference in the normal fertilization (2PN) between the studied groups (≤39 years: 82.8%; 40-49 years: 75.8%; and ≥50 years: 82.4%). Percentages of zygotes that underwent cleavage (100%, 92.2%, and 95.4%), mean cell number (7.3 ± 1.01, 7.3 ± 0.93, and 6.5 ± 1.22), and good quality embryos on day 3 (83.3%, 85.2%, and 70.4%) were similar from the groups of ≤39 years, 40-49 years, and ≥50 years, respectively. Blastocyst formation rate was significantly lower in the group of men ≥50 years compared to the other two evaluated groups (P < 0.05), but the percentages of good quality blastocysts were not associated with advancing paternal age (P = no significant). According to the chromosomal status of embryos, the advanced paternal age was significantly associated with high aneuploidy rates in embryos; thus, 73.9% embryos from the group of ≥50 years were aneuploidies compared to 59.1% in the group of ≤39 years and 61.1% in the group of 40-49 years (P < 0.05) (Fig. 1).
Results of fertilization, embryo cleavage, blastocyst development, and aneuploidy rates according male age.

P < 0.05 in relation to the groups of ≤39 years and 40-49 years.

Sperm DNA fragmentation, aneuploidy rate, and blastocyst formation according to male age.
Discussion
In the present study, we have evaluated the effect of male age on embryo quality/development and aneuploidy rates, including only IVF/ICSI cycles using donor oocyte for controlling female age. The data obtained demonstrate a significant negative effect of paternal age beginning from ≥50 years on the aneuploidy and blastocyst formation rates. These results are very important because they directly show the paternal aging effect on chromosomal status in embryos when the effect of the female age is controlled. Other studies that evaluated the paternal contribution to aneuploidy have shown an increase in the proportion of chromosomally abnormal embryos according to the severity of the male factor condition 17 but have no relationship to paternal aging in the first trimester pregnancy loss. 35
Nowadays, it is known that most human aneuploidies found in embryos originate from the egg and not the sperm,36–39 likely due to one critical difference in the meiotic process between males and females. It is now well established that aneuploidy is present in embryos from infertile patients and dramatically increases with maternal age40–42 from 73% for patients younger than 35 years and 87% for patients 41 and older. 10 Nevertheless, controversy exists whether aneuploidy rates in embryos are influenced by the advanced paternal age.
Deficiencies in sperm nuclear genome can be detected as early as the one-cell human zygote (early paternal effect) or throughout preimplantation development after eight-cell stage (late paternal effect). 43 During early paternal effect, centrosome dysfunction, disturbance in the number and spatial distribution of the nucleolus precursor body at pronuclear zygote stage, delayed cleavage divisions, and increases in the degree of cleaving embryo fragmentation can occur. The late paternal effect causes failure in the blastocyst formation and low clinical outcomes, and this effect has been associated with an increased incidence of sperm DNA fragmentation.43,44 The present study has not shown difference in fertilization rates, mean cell/embryo, and good quality at day 3 in the three age groups, suggesting a minimal or absence of early paternal effect on preimplantation development. Similar results were reported for fertilization rates45–47 and embryo quality45,47,48 when the effect of paternal age on assisted reproduction outcome was tested.
Evaluating the late paternal effect, a statistically significant decrease in the number of blastocysts on day 5 directly related to an increase in the sperm DNA damage was observed in the group of aging men. In patients ≥50 years old, only 26.9% of the embryos reached the blastocyst stage by the fifth day of development compared to 54.2% and 49.1% in the other two groups of younger men. These data confirm that when the male genomic activation occurs between the four- and eight-cell stage of human preimplantation development, factors such as age and sperm DNA quality induce chromosomal alterations that affect directly the embryo's capacity to reach the blastocyst stage, and then these strong paternal influences reduce the pregnancy and implantation rates in aging men inclusive of those cases using donated oocytes. Similar results were shown by Frattarelli et al 47 and Luna et al. 49
Sperm DNA fragmentation might be the most frequent cause of paternal DNA anomaly transmission to progeny and is found in a high percentage of spermatozoa from subfertile and infertile men. Apoptosis, abnormal chromatin packaging, and reactive oxygen species are the principal molecular mechanisms leading to sperm DNA fragmentation. 50 Studies by Lopes et al 51 and Gandini et al 52 have shown that spermatozoa with DNA fragmentation are able to fertilize an oocyte but are related to poor quality embryos, blockage of blastocyst development, and lower pregnancy rates through either natural or using intrauterine insemination, IVF, or ICSI procedures.53–56 Our study, similar to that of García-Ferreyra et al, 20 Plastira et al, 57 and Vagnini et al, 58 showed an age-dependent increase in sperm DNA fragmentation, but additionally we observed that this event was significant and directly related to embryonic aneuploidy when the male was ≥50 years old. These embryos with chromosomal abnormalities could be the more important cause to miscarriages in subfertile couples, older patients, and those cases from donated oocyte, including older men. This finding is important because it shows that advanced paternal age actively contributes to the generation of chromosomal abnormalities in the resulting embryos, and when the type and extent of DNA damage cannot be balanced by the reparative ability of the oocyte (including cases of egg donor), then the genetic screening in embryos should be considered to improve the clinical outcomes.
Male germ cells divide continuously. Approximately 30 spermatogonial stem cell divisions take place before puberty, while undergoing meiotic divisions. From then on, 23 mitotic divisions per year occur, resulting in 150 replications by the age of 20 years and 840 replications by the age of 50 years. 59 In older men, these numerous divisions in the stem cells joined to possible attacks from endogenous and exogenous factors can induce a wide range of DNA lesions, affecting normal cellular processes such as transcriptions, recombination and replication. 60 One of the main theories of aging states that aging results from the accumulation of unrepaired DNA lesions over life in many tissues, including the brain, the liver, and the testis.61,62 Paul et al 62 showed that there is an age-related accumulation of DNA damage in the testis, particularly caused by oxidative stress in the form of 8-oxodG lesions, and a lower capacity of germ cells to repair such DNA damage that leads to a decline in genome integrity that may produce aneuploidy embryos and/or be passed on to future generations, specifically the offspring of older males.
Chromosomal mosaicism is defined as the presence of two or more karyotypically distinct cell lines within an individual, occurs in ~15-90% of all cleavage human embryos,63,64 and may represent a major source of misdiagnosis in PGS because of both false-positive and false-negative results. 65 The genetic analysis on one cell or two cells reduces the chance of misdiagnosis because of mosaicism; however, based on the low incidence (5%) of mosaicism encountered in spontaneous abortions and vital pregnancies (2%), it is likely that most mosaic embryos are eliminated before the first trimester of pregnancy. 66 Developmental potential in mosaic embryos is related to the proportion and type of aneuploid cells involved, and when multiple chromosome anomalies on different cells are present, high rates of developmental arrest are observed. On the other hand, studies of Johnson et al 67 and Fragouli et al 68 have showed lower level of mosaicism at the blastocyst stage (16-33%), suggesting that preimplantation genetic screening via TE biopsy may reduce misdiagnosis by mosaicism. We suggest that future studies should be carried out by TE genetic analysis to avoid mosaic embryos misdiagnosed.
Programs of IVF with egg donor are believed to be so successful largely because oocyte quality is greatly improved when the donor's age is low, thus yielding better pregnancy rates and reduced miscarriage risk. One would hope that these good clinical outcomes could be due to absent or minimal chromosomal errors present in oocytes from healthy young donor; however, a previous study showed that 17% of human egg collected from healthy women at the age of 22-25 during natural cycle had spindle abnormalities, 69 which cause aneuploidy in embryos derived from donated oocytes. Our study showed a global aneuploidy rate of 65.1%, which is similar to the previously observed rates by Sills et al 70 and Haddad et al, 71 but unlike these studies, we have also showed that the advanced paternal age significantly increases the aneuploidy embryo rate since ≥50 years old, and this event is related to high values of sperm DNA fragmentation.
Conclusion
This study shows that male aging actively contributes to the generation of chromosomal abnormalities in the resulting embryos from oocytes donated and the effect on aneuploidy and blastocyst development rates significantly begin
from ≥50 years old. Embryonic genetic screening should be performed in cycles of egg donor if paternal age is >50 years to improve the clinical outcomes and reduce the miscarriage risk in this group.
Author Contributions
Conceived and designed the experiments: JGF. Analyzed the data: JGF and DL. Made critical revisions and approved final version: JGF, DL, LV, RR, PZ, RH, and JDC. All the authors reviewed and approved the final manuscript.