
Abstract
Background
The age-related reduction in live-birth rate is attributed to a high rate of aneuploidy and follicle depletion. We showed in an animal model that treatment with Coenzyme Q10 (CoQ10) markedly improved reproductive outcome. The aim of this study was to compare the post-meiotic oocyte aneuploidy rate in in vitro fertilization (IVF) and intra cytoplasmic sperm injection (ICSI) patients treated with CoQ10 or placebo.
Methods
We conducted a double blind placebo controlled randomized trial that included IVF-ICSI patients 35-43 years of age. The patients were treated with either 600 mg of CoQ10 or an equivalent number of placebo caps. We compared the post-meiotic aneuploidy rate using polar body biopsy (PBBX) and comparative genomic hybridization (CGH). According to the power calculation, 27 patients were needed for each arm.
Results
Owing to safety concerns regarding the effects of polar body biopsy on embryo quality and implantation, the study was terminated before reaching the target number of participants. A total of 39 patients were evaluated and randomized (17 CoQ10, 22 placebo), 27 were given the study medication (12 CoQ10, 15 placebo), and 24 completed an IVF-ICSI cycle including PBBX and embryo transfer (10 CoQ10, 14 placebo). Average age, base line follicle stimulating hormone (FSH), peak estradiol and progesterone serum level, as well as the total number of human menopausal gonadotropin (hMG) units–-did not differ between the groups. The rate of aneuploidy was 46.5% in the CoQ10 group compared to 62.8% in the control. Clinical pregnancy rate was 33% for the CoQ10 group and 26.7% for the control group.
Conclusion
No significant differences in outcome were detected between the CoQ10 and placebo groups. However, the final study was underpowered to detect a difference in the rate of aneuploidy.
Keywords
Background
A frequent and difficult challenge in women's reproductive health relates to the decline in reproductive outcome and the associated increase in chromosomal aberrations with increased female age. The Centers for Disease Control (CDC) in Atlanta provides a comprehensive annual report that includes the results for 90% of the infertility clinics in USA. For the year 2005, the average live-birth rate for in vitro fertilization (IVF) and fresh embryo transfer procedures was 34%. The live-birth rate sharply declined with age, from 43% in women aged <35 years to 6% in women aged ≫42 years. 1 The decline in live-birth rate reflects a decline in response to ovarian stimulation, reduced embryo quantity and quality, decreased implantation rates, and an increased incidence of miscarriages and fetal aneuploidy. The lack of an age-related decline in pregnancy outcome when donor oocytes are used suggests that the target of the reduced fecundity with aging is the oocyte. Moreover, there is a well-established association between late maternal age and an increased risk for oocyte and embryo aneuploidy.2,3
Unlike other cells, the mammalian oocyte and early embryo are completely dependent on mitochondrial oxidative phosphorylation (OXPHOS) for their supply of energy. 4 There is an increased rate of consumption of ATP in the mature oocyte that is essential for its ability to undergo normal fertilization. Therefore, it is possible that as women and their oocytes age, oocyte mitochondrial function may decrease influencing many of the processes of oocyte maturation, especially nuclear spindle activity and chromosomal segregation, resulting in an increased rate of aneuploidy.5,6 This hypothesis is supported by data demonstrating that mitochondrial mutations in follicular cells increase with age suggesting that OXPHOS and ATP production in the follicle are impaired in older women. 7 It has been demonstrated that embryo implantation potential is correlated with the ATP content of the embryo. 8 Wilding et al 9 used radiometric fluorescence techniques to measure changes in mitochondrial inner membrane potential (δΨm) of two-to-three-day-old fresh human embryos. The δΨm was highly correlated with mitochondrial capacity to produce ATP and ROS. The above authors found a strong correlation between low δΨm and the age of the patient as well as a state of random segregation of chromosomes between the blastomeres, likely resulting from the presence of an abnormal meiotic spindle. The embryos that had chaotic mosaics were significantly slower in their rate of cleavage and significantly more common among the older group of patients.
We initially sought to determine whether it is possible to improve oocyte mitochondrial function of elderly gravidas using “mitochondrial nutrients.” This is a group of endogenous vitamins that were previously shown to directly or indirectly protect mitochondria from oxidative damage. They were also reported to increase mitochondrial function, including energy production. The best studied of these nutrients to date are alpha-lipoic acid (R-ALA), Coenzyme Q10 (CoQ10), and resveratrol, all of which have been shown to have numerous benefits in neurodegenerative and cardiovascular diseases.10–13
We used an aged mouse model comparing retired breeders, eight-month olds, and mice randomized to receive either CoQ10, resveratrol, R-ALA or vehicle alone for a period of 18 weeks before superovulation. Compared to aged controls, CoQ10 treatment significantly increased the number of ovulated oocytes, increased oocyte mitochondrial ATP production, and reduced ROS levels to levels comparable to those detected in oocytes of young animals. 14
CoQ10 is a lipid soluble electron transporter that transports electrons from complexes I and II to complex III in the mitochondrial respiratory chain and is essential for the stability and action of complex III. 15 It also participates in the transport of protons in the mitochondria to maintain the membrane potential and drive ATP formation through ATP synthetase. 16 CoQ10 is a major cellular antioxidant. 17 There is a gradual, age-related decline in the tissue levels of CoQ10. 18 Mutations of genes involved in CoQ10 synthesis may lead to CoQ10 deficiency, characterized by clinical disorders involving mitochondrial dysfunction in the nervous system, skeletal muscles, and endocrine glands. 19
One study examined the use of CoQ10 in the in vitro culture of bovine embryos and found a superior rate of early embryo cleavage, blastocyst formation, percentage of expanding blastocysts, and a larger inner cell mass. These changes were associated with an increased ATP content in the group of embryos cultured with CoQ10. Other investigators have demonstrated an increased ATP production in lymphocytes supplemented with CoQ10. 20
As a result of this preliminary mouse study, we decided to conduct a comparative human study.
We hypothesized that the administration of CoQ10 two months before and during an IVF–intra cytoplasmic sperm injection (ICSI) cycle will improve oocyte energy production and reduce free oxygen radicals, thus resulting in a lower rate of oocyte aneuploidy. The aim of the study was to compare the post-meiotic rate of aneuploidy using polar body biopsy and comparative genomic hybridization (CGH) array for all chromosomes among patients treated with CoQ10 and placebo.
Material and Methods
The study was a double blind, placebo-controlled, randomized trial recruiting patients from two sites and using a single lab (Toronto Center for Advanced Reproductive Technology–TCART). The study was approved by the Mount Sinai Hospital–-Toronto, ethics review board (REB # 08-0205-A).
Trial Registration
The trial was registered on the clinical trials website (www.clinicaltrials.gov) (NCT01048385).
Inclusion criteria were infertility requiring IVF–ICSI and age 35-43.
Exclusion criteria were:
body mass index (BMI) ≫ 38 kg/m2 early follicular phase (day 2-4) serum follicle stimulating hormone (FSH) level ≫ 20 mIU/mL abnormal uterine cavity as evidenced by sonohysterogram or hysterosalpingography any current use of systemic steroid medication or any infertility treatment within three months of study enrollment any contraindication to being pregnant and carrying a pregnancy to term contraindication for the use of CoQ10, superfact, menopur, hCG, estrase, and progesterone suppositories any ovarian or abdominal abnormality that may interfere with adequate TVS evaluation absence of one or two ovaries clinically relevant systemic disease (eg insulin-dependent diabetes, adrenal dysfunction, organic intracranial lesion, polycystic ovarian syndrome, hyperprolactinemia, or hypothalamic tumor) or serious illness (neoplasia) history (within past 12 months) or current abuse of alcohol or drugs administration of any investigational drugs within three months before the study enrollment any medical condition that may interfere with the absorption, distribution, metabolism, or excretion of the study drugs; gastrointestinal diseases; mal absorption syndromes; and liver dysfunction unexplained gynecological bleeding ejaculated sperm not sufficient for ICSI abnormal controlled ovarian hyperstimulation (COH) screening blood done for both partners, including prolactin, thyroid stimulating hormone, HIV serology, Hepatitis B and C serology, Rubella, group and screen, and syphilis serology before participation in the study and the concurrent use of any of the following drugs:
daunorubicin, doxorubicin, blood pressure medications, warfarin, timolol, atorvastatin, cerivastatin, lovastatin, pravastatin, simvastatin gemfibrozil, tricyclic antidepressant medications (including amitriptyline, amoxapine, clomipramine, desipramine, doxepin, imipramine, nortriptyline, protriptyline, and trimipramine), multivitamins, or any vitamin supplementation except folic acid.
Patients were assigned in chronological order according to the day of study enrollment to a computer-generated randomization. Each enrolled participant received a pre-assigned package containing either placebo or CoQ10 for the duration of the study. Both the physician and the patient were blinded regarding assignment of the patients. Randomization was done following the signing of the informed consent.
In the first cycle, each patient received six capsules of micronized CoQ10 (100 mg softgels) or placebo (softgels and gelatin capsules containing rice oil and starch, respectively) (AOR–-Advanced Orthomolecular Research Inc., 19 St NE Calgary, AB, Canada, NHPD registration code 135307). Study participants took 600 mg of CoQ10 once a day with breakfast, orally, or identical placebo capsules for up to three cycles if pregnancy did not occur. All subjects took either CoQ10 or placebo for two months. On day 3 of the following cycle, they started ovarian stimulation for IVF while continuing the consumption of the supplements. COH was performed using the short microdose GnRH agonist flare protocol (SMF) or the long mid-luteal GnRH agonist protocol (LMG) according to the discretion of the primary physician. All gonadotropins used for this study were human menopausal gonadotropin (hMG) (Identical Batch of Menopur, Ferring Pharmaceuticals, Toronto, ON, Canada) and subcutaneous (SC) buserelin acetate 0.05 mg twice daily for the microdose flare protocol and 0.2 mg daily for the long luteal protocol (Suprefact, Sanofi-Aventis Canada Inc, Laval, QC, Canada), and continued until the day before human chorionic gonadotropin (hCG) administration (10,000 units; Pregnyl, Merck, Kirkland, QC, Canada). The dosage was maintained for the duration of the study. Both drugs were continued daily until follicular development was considered adequate (at least three follicles ≫17 mm and the E2 level acceptable for the number of follicles present). Oocyte retrieval was done 36 hours following the hCG injection under ultrasound guidance and with the use of local anesthesia and mild sedation. The oocytes were fertilized with ICSI with no regard to the quality of the sperm to prevent contamination of the polar body biopsy sample with sperm DNA. One or two polar bodies were biopsied simultaneously following proof of fertilization. The biopsied polar bodies were then sent to Mount Sinai Services (MSS Genetic Lab, Toronto, CA, USA) for DNA extraction and whole genome amplification followed by array CGH, a microarray-based CGH to analyze copy number of all 24 chromosomes (BlueGnome Ltd, Breaks House, Mill Court, Great Shelford, Cambridge CB22 5LD, UK). The results of the polar body chromosome analysis were available 24 hours after the biopsy to serve for embryo selection and allow either day 3 or day 5 embryo transfer.
One to three embryos were transferred mostly on day 3 post-retrieval when available. The rest of the viable embryos were frozen for subsequent embryo transfer in another cycle if needed. Luteal support consisted of 100 mg of progesterone suppositories (Kingsway Pharmacy, Toronto, ON, Canada) vaginally three times a day starting on the day of embryo transfer and continued for two weeks until the serum beta hCG result. If pregnant, the subjects stopped CoQ10/placebo and luteal support continued until 10 weeks of gestation.
The primary outcome measure was the number of euploid eggs per retrieval, and secondary outcome measures included cumulative pregnancy rate per retrieval and cumulative live-birth rate per retrieval.
Statistical analysis was done using GraphPad (Prism version 5.00 for Windows, GraphPad Software, San Diego, CA, USA, www.graphpad.com). Power analysis was calculated using the following assumptions: alpha 0.01, 90% power, background oocyte aneuploidy for the chosen group of patients–80%, the intervention will result in a 25% reduction in aneuploidy rate, and an expected average of six mature oocytes per retrieval in this group of patients. Based on these assumptions, we found that a total of 54 patients would be needed for this two-treatment parallel-design study.
Parametric data were analyzed using unpaired
Results
Characteristics of patients included the CoQ10 and placebo.

Treatment outcome for the patients in the CoQ10 and the placebo group.
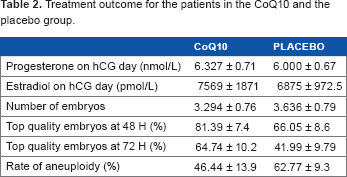
A total of 114 zygotes underwent PBBX, DNA extraction and amplification, and a CGH array. In all, 41 were from the CoQ10 group and 74 from the placebo group. The rate of aneuploidy in the CoQ10 embryos was 46.5% and in the placebo group was 62.8%. None of the results reached statistical significance.
Two of the transfers in each group were done five days after the retrieval whereas all the rest were done on day 3. Three patients did not have a transfer for the lack of any normal embryos (one in the CoQ10 group and two in the placebo group).
The clinical pregnancy rate was 33.3 and 26.7%, and live-birth rate was 25 and 26.7% for the CoQ10 and placebo groups, respectively.
Discussion
The decline in reproductive outcome associated with late maternal age is becoming a significant public health concern because of the current tendency of women to delay their childbirth. Thus far, there is no intervention apart from donor eggs capable of negating the adverse effects related to age.
There is plenty of data supporting a role for the rate of metabolism and mitochondrial function with aging and longevity.22,23 Small animals with a high rate of metabolism show an accelerated rate of aging in general as well as an accelerated reproductive senescence.24–26 This allows for the use of mice as a model to study ovarian aging as well as potential interventions. 27 In our animal model, we were able to show that prolonged exposure of elderly mice to CoQ10 was able to improve oocyte mitochondrial function, reduce the rate of decline of ovarian reserve, and restore reproductive outcome to a level comparable to young mice. Wilding and colleagues associated the age-related decline in oocyte mitochondrial function to a dysfunction of the spindle apparatus and an abnormal segregation of chromosome leading to aneuploidy. 9
In the present study, we treated patients undergoing IVF-ICSI with either CoQ10 or placebo for two months before and up to oocyte retrieval, and compared the rate of oocyte aneuploidy between the two groups. Owing to the premature termination of the study for safety concerns, we were not able to reach the target number of patients defined by a power analysis. The results show a lower rate of aneuploidy in the CoQ10 group although the results did not achieve statistical significance. One simple explanation for the lack of significant differences between the CoQ10 and the placebo groups is the small sample size. Based on a power calculation, the study had to include a minimum of 27 patients in each arm. However, because of the premature termination of the study, the CoQ10 group had only one-third and the control group half of the target number.
Another possible explanation for the difference in outcome between our human and animal study is the relative length of time in which CoQ10 was given. In the mouse study, the animals were treated for a quarter of their life span before being super-ovulated compared to only two months in humans.
CoQ10 is an essential part of the cellular energy production machinery; however, it is also a potent cellular antioxidant. There are data showing that cells severely deficient in CoQ10 show a reduced ATP concentration that can be corrected following one week of incubation with CoQ10. 28 Aging was associated with differing levels of CoQ10 deficiency both in rats and humans. Even in the very old age group, in most tissues the decline of CoQ10 concentrations was not below 50% of peak concentration. 29 Ovary is an organ that shows preferential absorption of exogenous CoQ10. 30 We can, therefore, make the assumption that treatment with CoQ10 for two months may have been sufficient to restore normal energy production in the ovary.
Recently, several publications studying the origin of the age-related increase in aneuploidy have pinpointed it to the second meiotic division, and in the vast majority of cases, it appears to be the result of premature separation of sister chromatids.31,32 This phenomenon is mostly attributed to a dysfunction of two nuclear proteins–-cohesin complex and shugoshins–-which in addition to crossover chiasmata maintain sister chromatid cohesion during meiosis. These proteins show no turnover and are of the same age as the oocyte. In addition, cohesin complexes and shugoshins have been shown to lose function after prolonged exposure to ROS. 33
Tarin et al have shown that the administration of the antioxidants Vitamins E and C was able to correct some of the age-related decline in reproduction in mice. 34
Quinzii et al used a model of gradual inhibition of CoQ10 production creating different levels of CoQ10 deficiency. 29 They were able to show that at the level of CoQ10 typically seen in the elderly, the effect observed in mitochondrial function is not a decline in ATP production, but rather an increase in ROS production. In reviewing these data, we conclude that the administration of CoQ10 for two months, although sufficient to correct a potential lack of ATP in the oocyte, might not be enough to prevent the effects of prolonged exposure to ROS on the meiotic apparatus. More research is needed to study the effects of a longer duration of intake of CoQ10 on female reproductive function in women of various ages.
Author Contributions
YB, AJ, NE, and RFC conceived and designed the experiments. YB, AJ, NE, and RFC analyzed the data. YB, TH, AJ, NE, and RFC wrote the first draft of the manuscript. YB, TH, AJ, NE, and RFC contributed to the writing of the manuscript. YB, TH, AJ, NE, and RFC agreed with manuscript results and conclusions. YB, TH, AJ, NE, and RFC jointly developed the structure and arguments for the paper. YB, TH, AJ, NE, and RFC made critical revisions and approved the final version. All authors reviewed and approved the final manuscript.
Dsiclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgment
We wish to thank Ferring Pharmaceuticals for their support to the study.