
Abstract
Ectopic pregnancy is defined as implantation and subsequent development of an embryo outside the uterine lining. It has wide range of presentation from acute hemoperitoneum to chronic ectopic pregnancy. This is an unusual case of chronic ectopic pregnancy with large hematosalpinx without classical symptoms. A 22-year-old South Indian woman reported to the outpatient clinic with irregular spotting for a duration of 2 months which was not associated with pain. There was no preceding amenorrhea and previous menstrual cycles were regular. Clinically, the patient was hemodynamically stable but severely anemic. The abdomen was soft on palpation, cervical movements were not tender, and human chorionic gonadotropin was absent in the urine. Ultrasound revealed a complex adnexal mass. Magnetic resonance imaging (MRI) revealed a large hematosalpinx. Laparoscopic left salpingectomy was conducted and histopathology confirmed ectopic pregnancy. Ectopic pregnancy presents diagnostic dilemmas in the absence of classical symptoms. MRI and laparoscopy are important tools in such a diagnostic dilemma.
Introduction
Ectopic pregnancy is the presence of gestational sac outside of the endometrial cavity. Ectopic pregnancy turns chronic when there are multiple small hemorrhages into the peritoneal cavity with the formation of pelvic hematocele. Chronic ectopic pregnancy has relatively less acute symptoms. 1 It rarely presents as large hematosalpinx 2 without classical symptoms as in our case as we did not have any symptoms.
Case Report
A 22-year-old South Indian woman reported irregular bleeding for 2 months, associated with discomfort in the lower abdomen. There was no history of preceding amenorrhea. She was primi para with one live child who was delivered by caesarean section 4 years prior. There were no menstrual irregularities in the past. There was no history suggestive of prior pelvic infection or endometriosis. She was a non-smoker. She was not using any contraceptive methods.
On examination, pallor was present. Pulse rate was 78 beats per minute and blood pressure was 130/80 mmHg. Abdomen was scaphoid and soft on palpation. There was no localized tenderness, no guarding or rigidity, and no palpable mass. Speculum examination revealed minimal bleeding through the external ostium uterus and a healthy vagina. Bimanual examination revealed a retroverted normal-sized uterus with fullness in the left fornix. Cervical movements were not tender.
On investigation, hemoglobin was 5% g (reference range 12-14% g), urine for human chorionic gonadotropin (hCG) was negative. The diagnosis of ectopic pregnancy cannot be ruled out when urinary hCG is negative. Hence, we measured the serum βhCG level, which was 9.84 IU/mL (reference range < 1 IU/mL in non-pregnant premenopausal age). Clinical examination suggested an adnexal mass. There was a possibility of endometrioma and ovarian mass; hence, serum level of cancer antigen 125 was measured and was found to be 39.3 IU/mL (0.1-35 IU/mL).
Ultrasonography of the pelvis revealed a complex adnexal mass. However, a definite diagnosis could not be made and the patient was subjected to magnetic resonance imaging (MRI) (Fig. 1). MRI revealed a complex tubular, peripherally enhanced lesion arising in the left adnexa and traversing anterosuperior to the uterus to the right side. Few incomplete folds were observed, indicating the lesion as a dilated fallopian tube. The contents of the tube showed high signal intensity on T1-weighted fat-suppressed images and a diagnosis of hematosalpinx was made. A small amount of T1 hyperintense fluid was also noted anterior to the urinary bladder, suggesting minimal hemoperitoneum. Incidentally, a simple cyst was noted within the left ovary.
MRI findings.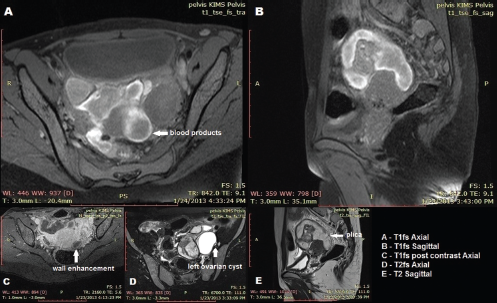
Diagnostic laparoscopy was performed, which revealed adhesions between the bowel loops hiding the left tube and ovary. These adhesions were gently released and a large hematosalpinx of size 8 X 6 cm was exposed. The right tube was normal and a simple cyst of 4 X 3 cm was noted in the right ovary. Left salpingectomy and right ovarian cystectomy were performed. Histopathological examination of the left tube showed chorionic villi with in the tubal lumen, confirming the diagnosis of ectopic pregnancy (Figs. 2 and 3).
Histopathology showing tubal lining and villi suggestive of ectopic pregnancy.
Discussion
Ectopic pregnancy exhibits a wide range of clinical presentation. Chronic ectopic pregnancy is a challenge for obstetricians because of its non-classical symptoms and limitations in its diagnosis. 1
Hematosalpinx is defined as bleeding into the tubes; tubal pregnancy is the most common cause of hematosalpinx. The course of tubal pregnancy is determined by the site of blood collection. It presents as a broad ligament hematoma if the tube ruptures at the inferior end. This can form pelvic hematocele if the tube ruptures on the antemesentric border. Intraperitoneal collection can also occur by tubal abortion without rupture of the tube. If the bleeding occurs within the tube without rupture or abortion, hematosalpinx can result. 2
It is rare for a chronic ectopic pregnancy to present as hematosalpinx as was observed in our case. Chronic ectopic pregnancy typically results from a small but recurrent bleed into the pelvic peritoneal cavity. The resultant effect is the formation of pelvic hematocele which is organized clot in between the pelvic structures. This is the triggering factor for the formation of adhesions to the adjacent organs. 3 In certain conditions, this bleeding accumulates with the tube itself to form a hematosalpinx without communicating into the peritoneal cavity. 4
The symptoms and signs of chronic ectopic pregnancy are not classical. Adding to the confusion are negative results of the relevant investigations, including negative urine analysis for pregnancy 5 and negative culdocentesis. The surgical management is further challenging because of chronic inflammation and resultant adhesions between the pathology and adjacent bowel/bladder.
The diagnosis of acute ectopic pregnancy can be made by combination of clinical, sonological, and laboratory findings.
Ultrasound plays an important role in diagnosing this condition. 6 Ultrasound could not clearly identify the origin of the mass in our case and hence we conducted magnetic resonance imaging. MRI can be used in cases of diagnostic difficulties. The structural pathology can be studied and surgical procedure could be planned with more clarity.
The normal fallopian tubes are rarely seen on MRI unless surrounded by fluid as occurs in ascites. 7 When dilated, the fallopian tube appears as a fluid-filled tubular structure arising in the region of the uterine cornua and occupying the adnexa. The presence of multiple interdigitating folds of incompletely effaced mucosal and submucosal plicae have been described as a characteristic feature of a dilated fallopian tube. 8 However, in a markedly dilated tube, these plicae may be completely effaced. 9 Sometimes, a dilated fallopian tube can resemble a multicystic mass which can be confused for an ovarian tumor. 10 Thus, demonstration of a normal ovary separate from such a dilated tube maybe very useful in making a correct diagnosis. Difficulty may also occur in differentiating a dilated fallopian tube from a small bowel loop. Presence of air (no signal intensity), thicker enhancing walls, and change in position of the bowel loop may aid diagnosis.
In a simple hydrosalpinx, the tubal contents are of low signal intensity on T1 and high signal intensity on T2 weighted images. However, the presence of blood (hematosalpinx) or proteinaceous material within the tube often returns high signal intensity on T1-weighted images, best demonstrated by fat suppression. The walls of the dilated fallopian tube are typically thin and may show contrast enhancement.
MR imaging may also provide clues regarding the cause of hematosalpinx when present. The most common reported cause of hematosalpinx is tubal endometriosis. 11 The presence of typical endometriotic ovarian cysts (T1 hyperintense with T2 shading), features of adenomyosis in the junctional zone of the uterus, and the presence of T1 hyperintense pelvic deposits may all point towards endometriosis being the causative factor. However, isolated hematosalpinx has also been reported in endometriosis. 12 The presence of an enhancing solid component within the dilated tube suggests the possibility of fallopian tube neoplasm. However, this appearance is uncommon and fallopian tube cancer is often seen as a complex cystic- solid enhancing adnexal mass, many times indistinguishable from a primary ovarian malignancy. 13
The presence of a gestational sac with or without an embryo in the hematosalpinx (seen as an enhancing thick-walled ring-like structure) is a conclusive sign of ectopic pregnancy within the fallopian tube. 14 Other imaging features indicating fallopian tube pregnancy include presence of hemoperitoneum associated with hematosalpinx and prominent enhancement of the tubal walls. However, the most common appearance of a tubal ectopic is in the form of a heterogeneous adnexal mass with or without the ipsilateral ovary seen separately. 15 Fibrin strands containing chorionic villi may appear as a multiple linear branching structures have also been reported. 16 Most of these features are well seen on USG and MRI is often not required for straight-forward cases. With increasing awareness and training in laparoscopy, conservative surgery such as salpingectomy can be conducted by laparoscopy, even in rural areas. 17
Conclusion
Chronic ectopic pregnancy is a challenge to the obstetricians with difficulty in diagnosis and management. Chronic ectopic pregnancy can present as hematosalpinx. Diagnosis in difficult cases can be accomplished by MRI and laparoscopy.
Author Contributions
Conceived and designed the experiments: MN, VSV, SBG, VKK. Analyzed the data: MN, VSV, SBG. Wrote the first draft of the manuscript: AA, MN, VSV, VKK. Contributed to the writing of the manuscript: AA, MN, VSV, SBG, VKK. Agree with manuscript results and conclusions: MN, VSV, SBG, VKK, AA. Jointly developed the structure and arguments for the paper: MN, VSV, SBG, VKK, AA. Made critical revisions and approved final version: MN, VSV, SBG, VKK, AA. All authors reviewed and approved of the final manuscript.
Dsiclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.