
Abstract
Circadian rhythm abnormalities, as shown by sleep/wake cycle disturbances, constitute one the most prevalent signs of depressive illness; advances or delays in the circadian phase are documented in patients with major depressive disorder (MDD), bipolar disorder, and seasonal affective disorder (SAD). The disturbances in the amplitude and phase of rhythm in melatonin secretion that occur in patients with depression resemble those seen in chronobiological disorders, thus suggesting a link between disturbed melatonin secretion and depressed mood. Based on this, agomelatine, the first MT1/MT2 melatonergic agonist displaying also 5-HT2C serotonergic antagonism, has been introduced as an antidepressant. Agomelatine has been shown to be effective in several animal models of depression and anxiety and it has beneficial effects in patients with MDD, bipolar disorder, or SAD. Among agomelatine's characteristics are a rapid onset of action and a pronounced effectiveness for correcting circadian rhythm abnormalities and improving the sleep/wake cycle. Agomelatine also improves the 3 functional dimensions of depression—emotional, cognitive, and social—thus aiding in the full recovery of patients to a normal life.
The Link between Circadian Rhythm Disturbances and Human Depression
Depression and Circadian Rhythms
Depression is a family of complex multifactorial illnesses that are characterized by disruptions of several physiological, neuroendocrine, and behavioral processes. According to a WHO report, the depressive disorders account for the fourth leading cause of global burden of disease and by the year 2020 they are expected to be the second highest cause of morbidity. 1
Circadian rhythm abnormalities, as shown by sleep/wake cycle disturbances, constitute one the most prevalent signs of depression; advances or delays in the circadian phase are documented in patients with major depressive disorder (MDD), bipolar disorder, or seasonal affective disorder (SAD).2,3 Disturbance of the sleep/wake cycle is one of the DSM-IV diagnostic criteria for depression, 4 and people with major depression commonly experience changes in sleep/wake cycle regulation that are seen as abnormal total sleep duration, poor sleep efficiency, overwhelming rapid eye movement (REM) sleep, and early morning awakening.5,6
In addition to an altered sleep-wake cycle, daytime mood variation and periodic recurrences are clinical findings that relate depression with the circadian system. 7 A significant proportion of patients show regular changes in the intensity of depressive mood during the day, with parallel changes in anxiety symptoms, attention capacity, and psychomotor symptoms that frequently accompany depression. Depressive patients with melancholic characteristics typically have an early morning awakening and morning worsening in their mood state. Both symptoms are part of the clinical diagnostic criteria of the melancholic depressive subtype. While the findings imply that altered circadian rhythms have a primary causal influence in depression, definitive evidence on this point is not yet available. 8
An internal desynchronization of circadian oscillators with a strong oscillator being linked to phase advances was postulated. 9 In patients with unipolar and bipolar depression, evidence has been provided for a phase advance of the temperature-REM sleep cycle in relation to the rest/activity cycle. 10 Phase advances in the rhythm of melatonin secretion have now been documented in numerous studies of patients with MDD.11–15 However, in some studies MDD patients show a phase delay in melatonin secretion.16–18 Delays in the onset of urinary 6-sulfatoxymelatonin (a6MTs) excretion were reported in a study of 382 postmenopausal women with MDD. 19 In that study a close association between depressive symptoms and delayed offset of a6MTs excretion was found, suggesting that the timing of melatonin secretion is important for the regulation of mood.
A number of studies have shown that the phase of melatonin secretion also varies systematically with mood changes in bipolar affective disorders. Phase advances of at least 1 hour were observed in the nocturnal melatonin peak during the manic phase as compared to the euthymic or depressed phase. 20 Phase delays in circulating melatonin have also been documented in bipolar type 1 patients. 21
In contrast to bipolar patients, patients suffering from SAD exhibit delayed circadian rhythms, 22 with delayed offset of melatonin secretion of about 2 hours being reported.23,24 Clinical studies involving chronobiological manipulations such as exposure to bright light in the morning and/or melatonin administration in the evening have been found useful for reducing phase abnormalities and depressive symptomatology in SAD patients. 25
Organization of the Circadian System
In mammals, the circadian timing system is composed of many individual, tissue-specific cellular clocks. 26 At a molecular level, these circadian clocks are based on clock genes, some of which encode proteins able to feedback and inhibit their own transcription. To generate coherent physiological and behavioral responses, the phases of this multitude of cellular clocks are orchestrated by a master circadian pacemaker residing in the suprachiasmatic nucleus (SCN) of the anterior hypothalamus. 27 The central clock is a key regulator of many bodily functions that follow a circadian rhythm such as sleep and wakefulness, thermoregulation, and glucose homeostasis and fat metabolism.
A number of studies have tested variants of genes that control the circadian system for their association with mood disorder and circadian-related polymorphisms have also been reported in depressive illness. Single-nucleotide polymorphisms (SNP) of the circadian genes Clock, NR1D1, Bmal1, Per3, Rorα, Rorβ and Cry2 have been associated with bipolar disorder.28–32 Notably, Npas2 deficient mice 33 and Clock mutant mice 34 display behavior patterns resembling the manic state associated with bipolar disorder. In the case of SAD, the SNP examined for each of three circadian genes Per2, Bmal1, and Npas2, indicated an increased risk for developing depression.35,36 It must be noted, however, that most findings await replication in larger samples and populations.
The pineal methoxyindole melatonin is a synchronizer of the SCN clockwork. In mammals, melatonin is synthesized in the pineal gland in a rhythmic manner, with high levels during nighttime and low levels during daytime. 37 Melatonin phase-shifts circadian rhythms in the SCN by acting on the MT1 and MT2 melatonin receptors expressed by SCN neurons, thus creating a reciprocal interaction between the SCN and the pineal gland. 38 Melatonin's phase-altering effect is caused by its direct influence on the electrical and metabolic activity of the SCN. The circadian rhythm in the secretion of melatonin has been shown to be responsible for the sleep/wake rhythm in both normal and blind subjects (ie, in the absence of the synchronizing effect of light). 39
Since melatonin is involved in the regulation of both circadian rhythms and sleep, any antidepressant drug with effects on melatonin receptors could be an advantage in treatment. Melatonin treatment has been found to be effective in treating circadian rhythm disorders as well as insomnia.40,41 As far as its antidepressant activity, melatonin (10 mg/day) was inactive in affecting bipolar affective disorder 42 and improved sleep with no effect on symptoms of depression in MDD.43,44 In SAD, melatonin (5 mg/day) was ineffective, 45 while in patients with delayed sleep phase syndrome and comorbid depression, melatonin administration improved the circadian profile scores of sleepiness, fatigue, and alertness, thus having antidepressant properties. 46
To improve the efficacy of melatonin's sleep promoting effects, several analogs of melatonin have been developed for treating circadian rhythm sleep disorders or insomnia. Among these, agomelatine (Valdoxan®, Servier, France) has been licensed by the European Medicines Agency (EMEA) for the treatment of MDD in adults. Agomelatine has a unique pharmacological profile as it is both a MT1/MT2 melatonin receptor agonist and an antagonist of 5-HT2C receptors. As the first melatonergic antidepressant, agomelatine displays a non- monoaminergic mechanism. 47 As agomelatine addresses sleep disturbances as well as depressive symptoms and has early onset of action, even in severely depressed patients, it stands alone among the antidepressants for effective management of MDD. 48
Agomelatine: The First Melatonergic Antidepressant
Chemistry, Pharmacokinetics and Metabolism
Agomelatine has a molecular formula of C15H17NO2 and a molecular weight of 243.30. It is a napthalenic compound chemically designated as N-[2-(7-methoxynaphth-1-yl)ethyl] acetamide (Fig. 1). Agomelatine has a high agonist affinity at MT1 and MT2 receptors. 49 Agomelatine is also an antagonist of 5-HT2C and 5-HT2B serotonin receptors. 50 Agomelatine displays an overall selectivity (> 100-fold) for MT1 and MT2 receptors as compared to other receptor sites. The affinity of agomelatine for melatonin receptors is comparable to that of melatonin (K = 8.52 × 10–11 mol/L and 2.63 × 10–10 mol/L respectively). Agomelatine has no significant affinity for muscarinic, histaminergic, adrenergic or dopaminergic receptor subtypes, 51 but it exhibits a high affinity as an antagonist of the human 5-HT2C receptor (IC50 = 0.270 μmol/L). Agomelatine binds only moderately to 5-HT2B and shows negligible affinity for 5-HT2A and 5-HT1A receptors.
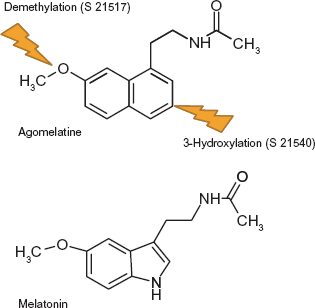
Chemical structure of agomelatine and melatonin. The major metabolites of agomelatine (S 21517) and S 21540 are shown.
Pharmacokinetic modeling of the metabolism of agomelatine indicated that its uptake from the gastrointestinal tract follows a first order process and that it is immediately transported into the liver compartment. 52 In the liver, three P 450 cytochromes are involved in agomelatine metabolism, namely CYPA1, CYPA2 and CYP2C9. The major metabolites have been identified as N-[2-(7-hydroxynaphth-1-yl) ethyl] acetamide (S 21517) and N-[2-(3-hydroxy-7-methoxynaphth-1-yl)ethyl] acetamide (S 21540) (Fig. 1). The hydroxylated, serotonin-like, S 21517 also showed affinity to 5-HT2C receptors, whereas binding of S 21540 was considerably weaker.
Mechanism of Action
Agomelatine is a high affinity ligand of MT1 and MT2 melatonergic receptors. Hence any discussion of its mechanism of action must consider first MT1 and MT2 receptor distribution in the brain.
In the mammalian brain, MT1 and MT2 receptors have been found in the SCN, prefrontal cortex, cerebellar cortex, hippocampus, basal ganglia, substantia nigra, ventral tegmental area, nucleus accumbens and in retinal horizontal, amacrine and ganglion cells 53 and choroid plexus. 54 The MT1 receptor is highly expressed in the human SCN 55 and mainly in vaso-pressinergic neurons,56,57 a finding that can be critical since the release of vasopressin is one of the important components of the SCN circadian output.
MT2 was not detected in an earlier investigation of the human SCN. 55 This receptor subtype is expressed in the SCN of numerous mammals and is particularly important for circadian phase shifting.58–61 Since circadian clock reset does occur in humans after the administration of melatonin or agomelatine,62–65 these changes must be induced by MT1 signaling. Relatedly, the binding of melatonin to transcription factors of the retinoic acid receptor superfamily, including RORα isoforms a, b and d (formerly called RZRα) and the product of another gene, RORβ or RZRβ, are increasingly considered as physiologically important. Some of these transcription factors interact with the circadian core oscillators, thereby influencing phasing, resetting, and period lengths of circadian rhythms. In the mammalian brain, expression of RORoc subforms and RORβ is detectable in the SCN and other parts of the hypothalamus, the thalamus, pineal gland, retina, spinal cord, and pars tuberalis. 66 Remarkably, RORβ signal is highest in areas of highest MT1 receptor density, suggesting the possibility that some sort of cooperation may exist between the membrane and nuclear receptors, especially in areas containing circadian oscillators. RORβ knockout mice exhibited significant circadian changes, including for example a larger phase advance and slower resynchronization than wild type mice.67,68 To what extent agomelatine share the properties of melatonin in binding to the transcription factors of the retinoic acid receptor superfamily remains to be defined.
The SCN is composed of neuronal oscillatory subsets, which differ in their recovery time after photic and non-photic signals. Differential phased ventrolateral and dorsomedial zones have been observed in rats subjected to a forced desynchronization protocol, and the oscillators are operating with alternate or parallel rhythms in gene expression of the cellular circadian oscillator. The coordinating effect of melatonin was demonstrated in pinealectomized rats, in which methoxyindole injection almost normalized the phase relationship of Per1 and Per2 genes in SCN. 69 In a recent study we reported that treatment with melatonin phase-delayed the expression of Per1, Per2 and Cry1 in rat anterior pituitary by approximately 6 to 10 hours, the changes fitting well with the phase-delayed gene expression of anterior pituitary redox enzymes as well as with the phase-delay found in plasma corticosterone rhythm. 70 Interestingly, agomelatine has a significant effect on the SCN expression of Per1 and Per2 as assessed in a model of post-traumatic disorder in rats in which the administration of agomelatine normalized the SCN expression of Per1 and Per2, as compared to controls. 71 Collectively the findings suggest that the chronobiological effects of melatonin agonists are probably much more complex than commonly thought and that the multioscillator organization of the circadian system must be taken in consideration.
Another feasible effect of agomelatine on the SCN is related to sleep. MT1-mediated effects in the SCN favor sleep initiation via the hypothalamic sleep switch, a mechanism characterized by typical on-off responses. This switch is thought to alternately activate either wake-related neuronal downstream pathways or promote sleep-related pathways. 72 Actions via the sleep switch do not seem to represent the exclusive route of melatonin-induced sleep onset. This is not surprising since sleep and sleep initiation are complex phenomena in which various brain areas are involved. The thalamus in particular contributes to the soporific effects of melatonin by promoting spindle formation, a characteristic feature of the transition from stage 2 sleep to deeper sleep stages. 73 This requires an additional thalamocortical interplay known to occur under these conditions. Moreover, the thalamus and other brain areas feedback to SCN.
In addition to sleep promotion, MT1 and MT2 receptors appear to be involved in the sedating and antiexcitatory effects of melatonergic drugs. This has been studied mainly in relation to anticonvulsant actions,74–79 which have been linked to a facilitatory role of melatonin on γ-aminobutyric acid (GABA) transmission. 80 The anticonvulsant activity of melatonergic agents seems to be mediated by MT1 and/or MT2 membrane receptors since similar effects were observed with the melatonergic agonist ramelteon. 81 In mammals, the antiexcitatory actions may also be related to additional anxiolytic, antihyperalgesic, and antinociceptive effects of melatonergic agents.82–88
A recent study indicates that agomelatine has anticonvulsant action in murine seizure models induced by pentylenetetrazole (PTZ) and pilocarpine. PTZ binds to the picrotoxin site of the GABA receptor complex and blocks GABA-mediated inhibition. 89 The agomelatine's main anticonvulsant effect is presumably mediated by GABA receptors and not via 5-HT2C receptor inhibition, since 5-HT2C antagonism was shown to enhance rather than to inhibit PTZ convulsions. In the case of pilocarpine (an agonist of muscarinic receptors) agomelatine's anticonvulsant effect at a high dose could be related to the demonstrated melatonergic action on the cholinergic system. 90
As in the retina, 91 an antagonistic relationship between melatonergic receptors and the dopaminergic system may exist in the central dopaminergic system.92–94 This antagonism was detected in preclinical studies which looked at agomelatine's effects as an inhibitor of the apomorphine-induced turning in 6-hydroxydopamine-lesioned rats. 95
It has been hypothesized that agomelatine has a unique mechanism of action because its effects are mediated though MT1/MT2 melatonergic receptors and 5-HT2C serotonergic receptors, acting differently at different circadian phases of the day/night cycle. 96 Through this dual action agomelatine may promote and maintain sleep at night and helps to maintain alertness during daytime. Agomelatine given before sleep would have an immediate sleep promoting melatonergic effect that would prevail over its potentially anti-hypnotic 5HT2C antagonism. 96 In contrast, during the day, the drug's 5-HT2C antagonism would predominate on melatonergic action, thus having an alerting action. 5-HT2C receptors are concentrated in frontal cortex, amygdala, hippocampus and corticolimbic structures that are involved in the regulation of mood and cognition. 97 They are also present in SCN, 98 and antidepressants decrease the number of 5-HT2C receptors. 99
One criticism to this dual interpretation of agomelatine action is the large differences in affinity for the putative action on serotonergic receptors as compared to the melatonergic one; about 3 orders of magnitude greater concentration are needed to exert 5-HT2C antagonism. 50 Moreover, both melatonin and ramelteon have been shown to display antidepressant-like effects even though they are not reportedly known to affect serotonergic receptors significantly.100–102
Agomelatine has been classified as a neutral antagonist of 5-HT2C, without inverse agonist properties. 103 This inhibition of 5-HT2C receptor has been interpreted as grounds for direct action of drug antidepressants (Table 1). These have to be distinguished from indirect actions related to melatonergic adjustments of circadian rhythms, which are effective in subtypes of depression with an etiology of circadian dysfunction. More recently, a synergistic interaction of the signaling mechanisms between melatonergic and 5-HT2C receptors has been assumed to explain the direct action of antidepressant agomelatine. 104 However, the precise nature of this type of synergy remains to be elucidated. Agomelatine has also been demonstrated to show robust anxiolytic properties, which appear to be higher than those of melatonin and can again be explained by a concerted action of melatonergic stimulation and 5-HT2C inhibition (Table 1).
Preclinical investigations on agomelatine.
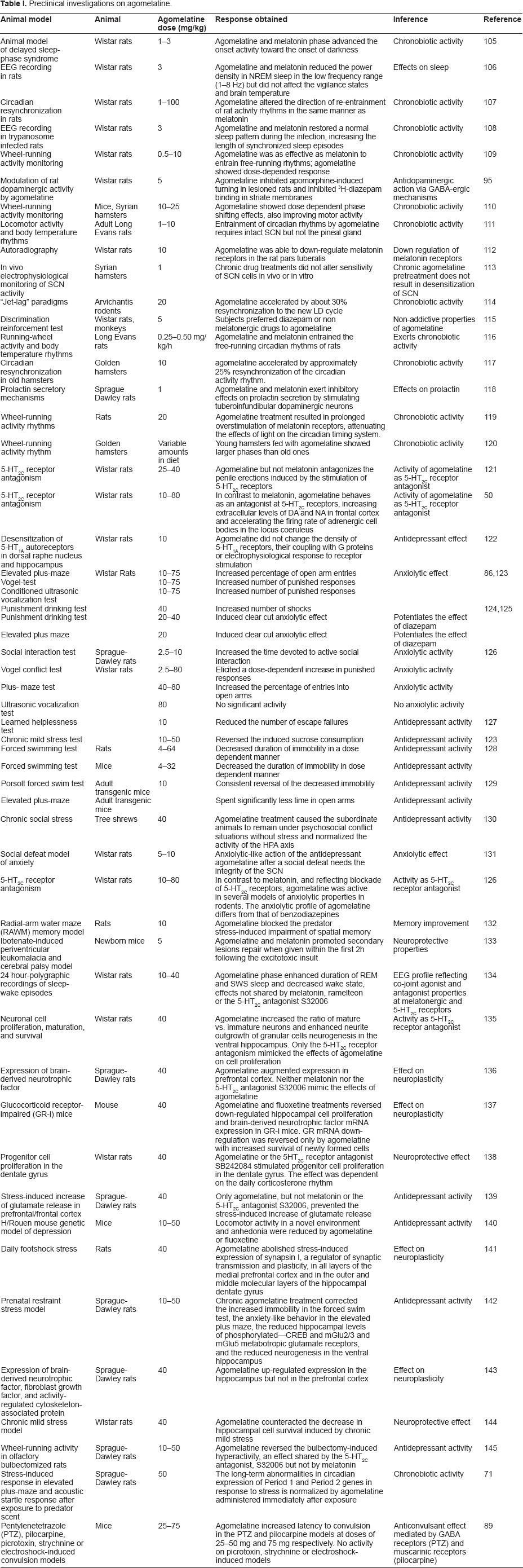
Preclinical Pharmacology
Table 1 summarizes published preclinical information on agomelatine activity. Agomelatine was found effective in several animal models of depression including learned helplessness, chronic mild stress, forced swimming, transgenic mice with decreased glucocorticoid receptor (GR) expression, H/Rouen mouse model of depression, footshock stress, prenatal restraint stress, psychosocial stress, olfactory bulbectomy and stress-induced increase of glutamate release in prefrontal/frontal cortex (Table 1). In some cases, for example stress-induced increase of cortical glutamate release, only agomelatine but not melatonin or 5-HT2C antagonists prevented antidepressant activity, 139 supporting the conjoint action on both effects ascribed to agomelatine. In other cases, for example wheel-running activity in olfactory bulbectomized rats, agomelatine effect was shared by 5-HT2C antagonists but not by melatonin, indicating an antidepressant action mediated exclusively by 5-HT2C receptor antagonism. 145
An interesting animal model of depression is the transgenic mouse with decreased GR expression, called GR-i mouse. It is based on the evidence indicating that malfunction of GR system can be instrumental in depression. The antidepressant activity of agomelatine was assessed in this transgenic mouse model by using a forced swimming test. 129 In the same model, agomelatine was investigated for anxiolytic properties in the elevated plus maze. The effects of agomelatine were compared to those of desipramine or melatonin. Treatment with agomelatine reversed the decreased immobility in forced swimming test seen in transgenic mice, the effect being comparable to that of melatonin or desipramine. Both the number of open arm entries and the total time spent in open arms of the elevated plus maze were greatly increased in transgenic mice and agomelatine was effective in reversing the GR-i behavioral changes noted in the elevated plus maze. 129 In the same study, agomelatine accelerated readjustment of circadian cycles of temperature and activity of transgenic mice following an induced phase-shift, the effect of agomelatine being more potent than that of melatonin. 129 This resynchronizing effect of agomelatine is of therapeutic value since the internal desynchronization of circadian rhythms is presumably implicated in the pathophysiology of depressive disorders. 146 Therefore, the antidepressant action of agomelatine can depend partly on its chronobiotic properties. In the same GR-i mouse model, both agomelatine and fluoxetine reversed down-regulated hippocampal cell proliferation and brain-derived neurotrophic factor (BDNF) mRNA expression. GR mRNA down-regulation was reversed only by agomelatine with increased survival of newly formed cells. 137
The anxiolytic properties of agomelatine have been explained through its antagonist action on 5-HT2C receptors,126,147,148 which are highly concentrated in frontal cortex, hippocampus, and basal ganglia, all associated with mood, motor, and cognitive functions.149,150 In the case of melatonin, its anxiolytic action can be demonstrated in animal models involving exploratory behavior.151–153 Melatonin's anxiolytic action involves GABA-related mechanisms. Although melatonin reduces the use of benzodiazepines in human beings for induction of sleep, it may not act via expression of its anxiolytic properties. 154
By using a combined neurochemical and behavioral approach, the anxiolytic action of agomelatine was compared to that of melatonin, the selective 5-HT2C receptor antagonist (SB243.213), and the benzodiazepine agonist clorazepate. 126 In the social interaction test model, agomelatine increased the time spent in social interaction by pairs of unfamiliar rats introduced into a novel environment. This action was mimicked by clorazepate and by SB243.213. In the Vogel conflict procedure, agomelatine exerted an anxiolytic activity with a maximal effect comparable to that of clorazepate and SB243.213. In the plus-maze test, agomelatine only moderately augmented the percent of entries into the open arm when compared to clorazepate, while SB243.213 was inactive. The anxiolytic action of agomelatine differed from that of benzodiazepines by its lack of inhibitory influence on the corticolimbic release of serotonin and norepinephrine, a finding that may explain the therapeutic efficacy of agomelatine in the treatment of depressive and anxious states. 155
In another study, agomelatine (40 mg/kg) was more effective than melatonin (20 or 40 mg/kg) in the punished drinking test in rats, but was as effective as melatonin (80 mg/kg), the finding being interpreted as an indication of a major 5HT2C antagonist activity property of agomelatine. 124 However, neither melatonin (40–80 mg/kg) nor agomelatine (20–40 mg/kg) counteracted response suppression during the period associated with the safety signal withdrawal, nor did they affect rats' behavior in the elevated-plus-maze. Co-administration of melatonin or agomelatine with diazepam, at a dose inactive on its own (0.25 mg/kg), induced anxiolytic effect in the punished drinking test and the elevated-plus-maze. 124 It was thus concluded that although melatonin or agomelatine were devoid of anxiolytic action per se, they potentiated the anxiolytic effect of diazepam. 124 The anxiolytic effect of melatonin or agomelatine depended upon the experimental procedures and time of administration.151–153
The anxiolytic activity of agomelatine was compared to that of melatonin and two anxiolytics, diazepam and buspirone. 86 The drugs were tested 2 hours before and 2 hours after the dark phase of the diurnal cycle. Morning and evening agomelatine administration increased animals' responses in the elevated plus maze and Vogel tests. Melatonin (10–75 mg/kg) enhanced open arms exploration in the evening experiment. The melatonin antagonist S22153 enhanced the action of morning and evening agomelatine administration in the Vogel and conditioned ultrasonic vocalization tests, while in the elevated plus maze test, S22153 inhibited effects of evening but not morning melatonin or agomelatine administration. The results indicate the involvement of both the melatonin and the 5-HT2C receptors in the mechanism of anxiolytic-like action of agomelatine. 86
It must be noted that the doses of agomelatine effective in underscorin the involvement of 5-HT2C receptor antagonist properties in preclinical pharmacology studies were 10–40 mg/kg in rats (Table 1). Calculation of the equivalent dose in humans made on the basis of the body surface area normalization method 156 yields a human equivalent dose of 114–456 mg/day for a 70 kg person, which is greater than those used clinically. It is therefore important to find out whether agomelatine causes functional blockade of 5-HT2C receptors in the human brain at standard clinical doses.
A recent paper does not support such a conclusion. 157 The acute administration of agomelatine to normal human volunteers did not reproduce the increase in slow wave sleep (SWS) reported for drugs with 5-HT2C receptor antagonist properties, 158 thus suggesting that, at clinical doses, agomelatine does not cause any functional blockade of brain 5-HT2C receptors in humans.
Neuronal plasticity is associated with depression, probably as a result of modified expression of proteins important for cellular resiliency. It is therefore important to establish whether antidepressant drugs are able to regulate these mechanisms in order to achieve relevant clinical effects. Clinical studies have shown that stress-related depressed patients have a reduced hippocampal volume.159–161 This reduction in hippocampal size was attributed to a decrease in granule cell neurogenesis and to neuronal atrophy due to increased exposure to corticosteroids via excitatory amino acids. 130 The dentate gyrus of the hippocampal formation is a site of continuous neurogenesis during adult life in mammals, including humans. 162 Treatment of animals with antidepressants and mood-stabilizing drugs increased the formation of neurons in the dentate gyrus. Indeed, the antidepressant effect on neurogenesis gives the basis for the neuroplasticity hypothesis of major depression.163,164 This effect was shared by agomelatine.165,166 The effect of agomelatine was selective since it only induced cell proliferation and neurogenesis in the ventral part of dentate gyrus, a region implicated in the response to emotion and anxiety, therefore providing the basis for explaining both the antidepressant and anxiolytic properties of the drug. More recently, a number of preclinical studies have reported that agomelatine increases expression of several neuroplasticity-associated molecules in the same regions (Table 1).136,138,141–144 Although these effects have generally been attributed to 5HT2C receptor antagonism, BDNF expression was found to be stimulated by the pure MT1/MT2 agonist ramelteon in cerebellar granule cells of wild-type, MT1, or MT2 knockout mice. 167 This was also seen with melatonin, but rather surprisingly only in MT2 knockouts. 167
Clinical Pharmacology
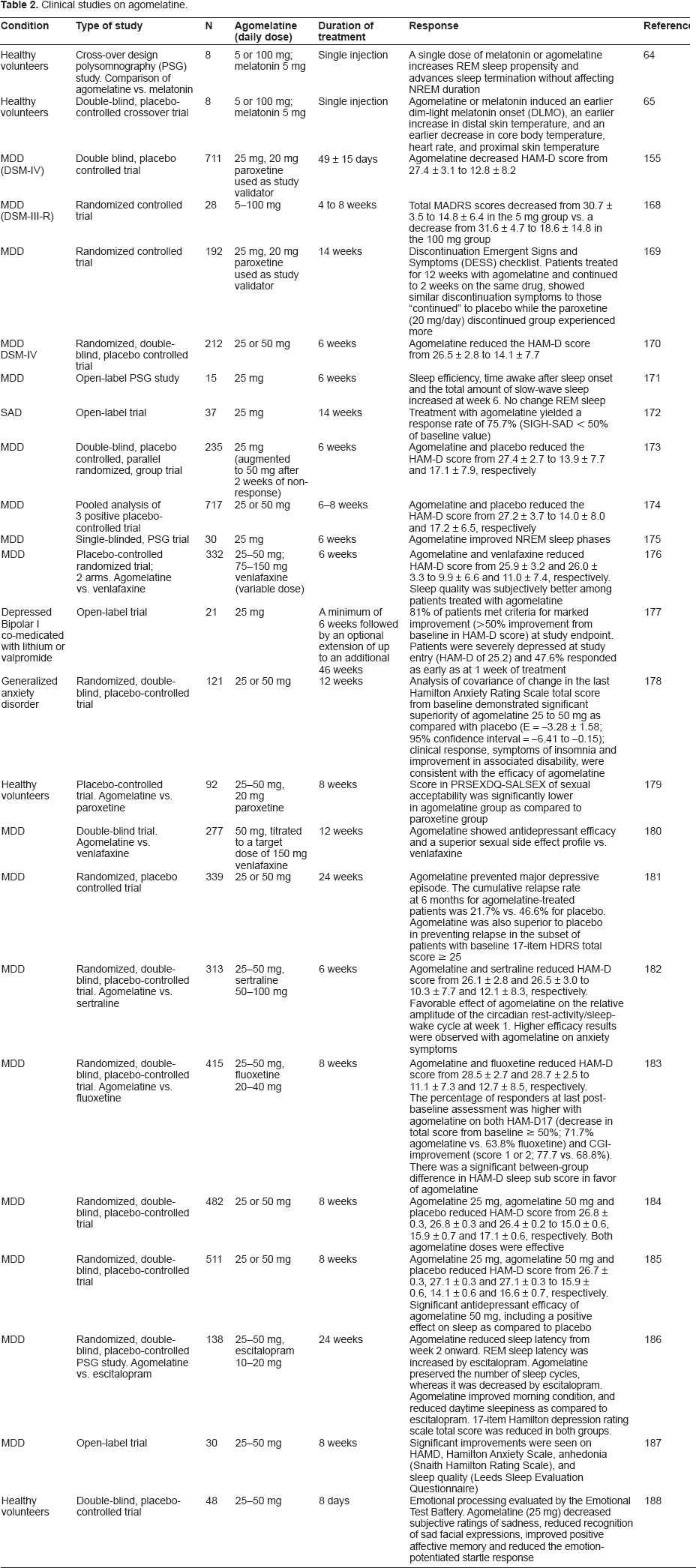
Starting from a double blind, multinational, placebo controlled trial of agomelatine conducted in 711 MDD patients, 155 ten similar studies have been published thus far (N = 3827, Table 2). Collectively, these studies indicate that agomelatine at doses of 25–50 mg/day is effective in reducing the depressive symptoms in patients with MDD. The effectiveness of agomelatine in severely depressed patients is particularly significant inasmuch as this patient group tend to be resistant to classical antidepressants. 155 Agomelatine has few adverse effects and is associated with early resolution of depressive symptoms. 189 The superior efficacy of agomelatine over other antidepressants, including paroxetine,155,169 venlafaxine, 176 fluoxetine, 183 and sertraline 182 is supported by several investigations (Table 2).
Clinical studies on agomelatine.
Agomelatine is unique because it has a chronobiological basis for its action and acts differentially at different circadian phases of the sleep/wake cycle. 96 While it promotes and maintains sleep at night, it also maintains alertness during the day. These effects are in contrast to traditional antidepressants which elevate the mood of depressed patients during daytime, an effect that is sustained at night and which causes impairment in sleep quality. 190
Agomelatine has been used in the treatment of bipolar affective disorder I and has been administered as an adjunctive to either lithium or valpromide for 46 weeks. 177 In this open label study, patients with severe Hamilton Anxiety Rating Scale (HAM-D) score higher than 25 showed clinical responses as early as one week after starting agomelatine therapy; 19 patients opted for an extension period up to 211 days (6–325 days) and 11 patients completed a one year extension period of treatment. There was no dropout from the study due to adverse events. 177
Interestingly a randomized, placebo-controlled study suggested that the pure MT1/MT2 melatonergic agonist ramelteon (8 mg/day) can also be beneficial for treatment of ambulatory bipolar I disorder patients. 101 Although ramelteon and placebo had similar rates of reduction in rating symptoms of insomnia, mania, and global severity of illness, ramelteon treatment was associated with an improvement in a global rating of depressive symptoms. These findings underline the interpretation that activation of MT1/MT2 receptors alone may be sufficient to induce antidepressant activity.100–102
Agomelatine has a low relapse rate (21.7%) when compared to placebo (46.6%), 6 months after continuous treatment. 191 This may well be because agomelatine targets residual symptoms such as anxiety or sleep disturbances. The early clinical response to agomelatine therapy was confirmed in another open-label study in which 24 patients suffering from MDD received agomelatine 25–50 mg for 8 weeks. 187 Agomelatine was found effective in reducing HAM-D scores and improving anhedonia seen in depression. Agomelatine not only has an early onset of action but also exhibits excellent safety and tolerability.192–194
In a randomized, double-blind, placebo-controlled trial in 121 patients with generalized anxiety disorder, the analysis of covariance of change in the last Hamilton Anxiety Rating Scale total score from baseline demonstrated significant superiority of agomelatine 25 to 50 mg as compared with placebo. 178 As discussed above, together with a 5-HT2C action, a GABAergic modulating action may account for the reported anxiolytic effects of agomelatine. While melatonin-like drugs have been reported to overlap the activity of GABA agonists (such as diazepam), neither agomelatine nor melatonin substituted benzodiazepines in anxiety-stressed rats trained to discriminate the different drugs. This suggests that the melatonergic anti-anxiety effect may be not addictive as compared to the diazepam's effect, therefore becoming a core feature when it comes to choosing the correct drug for substance abusers and other addictive-behavior populations.
One remarkable effect of agomelatine is to reduce sleep complaints in depressed patients. As already stated, sleep disturbances constitute one of the prominent features of depressive illness and are among the diagnostic criteria of DSM-IV for MDD. 195 Patients suffering from MDD or bipolar disorder exhibit marked difficulties in initiation and maintenance of sleep, poor quality of sleep, and frequent nocturnal and early morning wakening. 196 The NIMH Epidemiological Catchment Area study of sleep disturbances and psychiatric disorders identified sleep disturbances as a highly significant risk factor for subsequent development of depression. 197
Hence an ideal antidepressant should be able to decrease sleep onset latency (SOL) and wake-time after sleep onset (WASO), and should promote a feeling of well-being and alertness during the daytime. Sleep promoting effects of most antidepressants have been found to be either limited or non-existent. The effectiveness of agomelatine in reducing the sleep complaints of depressed patients has been ascertained. Altered intra-night temporal distribution of REM sleep with increased amounts of early REM sleep and reduction in SOL to REM sleep are the specific EEG sleep patterns that are associated with depression. 5 Hence prevention of sleep disturbances would help to reduce the risk of relapse or recurrence of depressive disorders. The treatment of depressive patients with agomelatine for 6 weeks increased the duration of non-REM (NREM) sleep without affecting REM sleep, thereby causing improvements in both sleep quality and continuity. 171 In a study that compared the effect of agomelatine (25 mg) with the antidepressant venlafaxine, agomelatine promoted sleep earlier and scored higher on the “criteria of getting into sleep”, as assessed by the Leeds Sleep Evaluation Questionnaire. 198 The improvement in sleep quality was evident from the first week of treatment with agomelatine, whereas venlafaxine did not produce any beneficial effect. This is important clinically inasmuch as improvement in sleep disturbances often precede that of depressive symptoms.175,199 Agomelatine has also been shown to be effective in reducing circadian rhythm disturbances in patients with MDD. 182
Agomelatine is thus a dual action drug that can produce rapid antidepressant effects while also improving sleep quality. This is important clinically inasmuch as improvements in sleep among depressed patients are associated with a reduced rate of recurrence of depressive symptoms and, conversely, complaints of poor sleep in depressed patients are associated with a poor response to subsequent antidepressant treatment.198,200 Another study provides strong support for the superior chronobiological effects of agomelatine in patients with MDD. 182 As compared to sertraline, agomelatine increased the relative amplitude of the circadian rest-activity cycle by the end of week one and in parallel there were improvements in sleep efficiency and in sleep latency from weeks one to six. Over a six week treatment period, depression and anxiety symptoms improved more with agomelatine than with sertraline.
Despite the foregoing, the relationship of sleep symptoms to depression and agomelatine treatment needs to be further examined. In particular, are those patients with a specific sleep pattern such as early morning waking or difficulty with sleep initiation more likely to respond to agomelatine than those without that pattern? If so, would it be possible to use the sleep pattern of depressed patients to predict the likelihood of response? The answer to these questions does not appear to have been addressed in any of the published papers to date. A second issue that has not been considered is that existing depression rating scales include sleep symptoms as part of the scale. For instance, the 17 item Hamilton Rating Scale for depression includes three items related to insomnia and later expanded versions added diurnal variation. Analysis of depression ratings separate from sleep symptoms is warranted to determine what part of the change is simply an improvement in sleep.
Safety
Agomelatine has an excellent safety and tolerability record, showing no difference from placebo except for dizziness (5.9% vs. 3.5%; P < 0.05). 201 Emergent adverse events, including gastrointestinal, cardiovascular, and body weight effects, were generally lower than sertraline or venlafaxine in active comparative trials. Moreover, antidepressant-induced sexual dysfunction was significantly lower than the specific serotonin reuptake inhibitors (paroxetine, sertraline and fluoxetine) or venlafaxine in both spontaneous reports and using structured instruments. 201 There were transient increases in transaminases, with an incidence similar to that of venlafaxine primarily when administered a higher dose of 50 mg per day. These were isolated, occurred mainly in the first month, and without clinical signs, and were reversible. In a study with the active comparator paroxetine, there was no evidence of discontinuation symptoms as compared to placebo. 169
A most notable effect of agomelatine is its almost absent effect on sexual function. Many antidepressants that are currently in use cause increased impairment of sexual function and a negative impact on quality of life. Most antidepressants have been shown to affect all phases of sexual activity, including desire, arousal, orgasm, and ejaculation. However, patients treated with agomelatine experienced significantly less sexual dysfunction than those treated with the placebo. 180
Because it is chiefly metabolized in the liver it should not be administered to patients with liver disease. 202 Agomelatine is contraindicated in patients receiving concomitant potent CYP1A2 inhibitors such as fluvoxamine or ciprofloxacin. However, paroxetine and fluconazole, which are moderate 1A2 and potent 2C9 inhibitors respectively, have little effect on agomelatine levels. 202
Increases in alanine aminotransferase and/or aspartate aminotransferase (3 times the upper limit of normal) have been noted in 1.1% of patients treated with agomelatine vs. 0.7% of patients treated with placebo. These increases were isolated and reversible and occurred without any clinical signs of liver damage. 201 In two recent studies,184,185 newly occurring, clinically notable aminotransferase elevations were respectively seen in 2.4% and 4.5% of patients in the agomelatine 50 mg group, but not in the agomelatine 25 mg or placebo groups. These transaminase elevations were not associated with clinical signs of liver damage and one of the incidental reasons for the transient elevation of aminotransferases could be the higher prevalence of hepatobiliary disorders at baseline in the agomelatine 50 mg group (3.1%) compared with the agomelatine 25 mg and placebo groups (0.6% each). In any event, it is recommended that liver function tests should be performed in all patients at initiation of treatment and then periodically after around 6, 12, and 24 weeks, and thereafter when clinically indicated. Any patient who develops increased serum transaminases should have their liver function tests repeated within 48 hours. Therapy should be discontinued if the increase in serum transaminases exceeds 3 times the upper limit of normal and liver function tests should be performed regularly until serum transaminases return to normal.
Place in Therapy
The ultimate goal of antidepressant therapy is the symptomatic and functional recovery that helps a return to normal everyday life. However, a large proportion of patients fail to achieve a complete and sustained recovery from depression and are left with residual symptoms and/or psychosocial impairments that make relapse or recurrence more likely, making poorer quality of life a reality.203,204
Most treatment guidelines recognize a symptom-free state as the best definition of disease remission, despite the fact that functional recovery often lags behind symptomatic improvement. Results from one large, prospective study of more than 7000 patients with at least one axis I disorder found that impairment in psychosocial functioning was apparent even in patients whose last episode occurred more than one year prior. 205 In another study, which investigated the association between psychosocial impairment and recurrence of depression, it was demonstrated that for each 1-point increase in functional impairment score, the risk of disease recurrence increased by approximately 12%. 206
Given the importance of all three dimensions of functioning (emotional, cognitive and social) in everyday activities such as work, and the impact that impaired functioning may have on a patient's life, it is clear that more attention should be paid to functioning when assessing treatment's response. Social functioning, a central component to a patient's quality of life, is defined as an individual's ability to carry out normal social roles. 206 In depression, loss of interest in activities, loss of self-esteem, loss of energy, and depressed mood compromises social functioning and affects the patient's ability to maintain relationships and to remain in employment. 207 Relationships at home are affected, with spouses and relatives reporting strains in their relationship with the patient, and feelings of burden and distress are common. In turn, less family support for the patient with depression may be associated with a greater risk of the patient drinking alcohol to cope.
In community-based studies, patients with depression reported less enjoyable and less intimate day-today social interactions than non-depressed controls. Indeed, in a long-term study of 371 patients with major depression that examined their relationships with spouse/partner, functional disability related to work/employment, and overall psychosocial function, psychosocial impairment increased as the severity of depressive symptoms increased. 205 Even a low-level of symptomatology was associated with a significant increase in psychosocial impairment.
Agomelatine rapidly improves social functioning. When the results from three published trials of agomelatine vs. placebo in patients with depression (agomelatine, N = 358; placebo, N = 363) were pooled, 208 item-by-item Hamilton Depression Rating Scale analysis showed significant benefit with agomelatine over placebo for 10 of 17 items, including the ‘work and activities’ item (difference in item score: 0.32; P < 0.001, vs. placebo at weeks 6 to 8), thus highlighting agomelatine's capacity to improve social functioning.
In addition, agomelatine efficacy has been shown to correlate with recovery in personal, social, and professional functioning in the 8 week VALID trial in patients (N = 111) with depression. 209 As early as the end of the first week, significant improvements from baseline were observed in Montgomery-Asberg Depression Scale scores and the work/school, social life, and family life sub-scores of the Sheehan Disability Scale. These significant improvements were maintained throughout the entire 8 week study period, with a return to normal levels of social functioning by the end of the study 209
The effects of agomelatine have been recently confirmed in results from the largest observational trial of the agent conducted to date, the CHRONOS program. 210 This “real world” trial included 6276 patients with moderate or severe depression who were given agomelatine monotherapy (25–50 mg/day) for 8 weeks. As early as the first week of treatment, a significant reduction from baseline in HAM-D17 total score was apparent; this continued improvement was seen throughout the remainder of the trial. Crucially, rapid and continual improvement in social function (items 7 and 8 of the HAM-D17 scale: work/activities and retardation [psychomotor activity]) was also seen in this population, from week 1 through to the end of week 8. By week 8, 81% of patients had responded to treatment with agomelatine and 59% were considered to be in remission. According to the CGI—Severity scale, there was a consistent decrease in the proportion of patients with moderate, severe, or very severe depression during the study, from 100% of patients at baseline to 75% at week 1 and 7% at week 8. 210
Conclusions
The novel antidepressant drug agomelatine is an agonist of MT1 and MT2 melatonin receptors and an antagonist of 5-HT2C receptors. Pre-clinical studies demonstrated that agomelatine may exert its antidepressant activity via its interaction with both types of receptors. Agomelatine's mechanism of action differs from all other antidepressants on the market since it is a chronobiotic improving the extent of the sleep/wake cycle, which in turn improves sleep and quality of everyday performance. Agomelatine's efficacy in improving sleep and in resynchronizing the disturbed circadian rhythms makes it a very useful antidepressant. In clinical trials, patients experience improvements in social functioning and relief of symptoms at the first week of treatment, and these effects are maintained and even improved during the treatment period. Agomelatine improves the three functional dimensions of depression—emotional, cognitive, and social—hence it can be a ready to use drug for our anxiety-disturbed society.
Author Contributions
Analysed the data: DPC. MFV, DEV. Wrote the first draft of the manuscript: DPC. Contributed to the writing of the manuscript: MFV, DEV. Agree with manuscript results and conclusions: DPC, MFV, DEV. Jointly developed the structure and arguments for the paper: DPC, MFV, DEV. Made critical revisions and approved final version: DPC, MFV, DEV. All authors reviewed and approved of the final manuscript.
Funding
Studies in authors' laboratory were supported by grants from Agencia Nacional de Promoció Científica y Tecnológica, Argentina (PICT 2007-01045 and PICT 2010-1465) and Universidad de Buenos Aires (M048). DPC and DEV are Research Career Awardees from the Argentine Research Council (CONICET). MFV is a doctoral fellow from CONICET.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.