
Abstract
Introduction
Clozapine, a second generation medication, has become the atypical antipsychotic drug of choice for refractory or treatment-resistant schizophrenia. In addition to the high risk of agranulocytosis and seizures, clozapine treatment is increasingly associated with significant metabolic effects, such as hyperglycemia, central weight gain and adiposity, hypertriglyceridemia, and elevated low-density lipoprotein cholesterol. A potentially life-threatening complication of altered metabolism is diabetic ketoacidosis (DKA). This report details a case of fatal DKA in a schizophrenic patient undergoing treatment with clozapine.
Case Description
An African–American male in his 20s with a medical history significant for schizophrenia was presented to the psychiatric inpatient ward with severe paranoid thoughts and aggressive behavior. After trials of risperidone, olanzapine, and haloperidol—all of which failed to adequately control his psychotic symptoms—clozapine titration was initiated and he showed significant improvement. Weight gain was observed throughout hospitalization, but all blood and urine test results showed no metabolic or hematological abnormalities. The patient was discharged for outpatient treatment on clozapine (125 mg morning and 325 mg evening) along with divalproex sodium and metoprolol. Six days post-discharge, the patient died. A medical autopsy later ruled that the death was due to DKA without any evidence of contributory injuries or natural disease.
Results and Conclusion
Significant increase in body mass index from 28.7 to 33.5 was observed during hospitalization. The blood glucose level, measured after his death, was found to be 500 mg/dL. Altered metabolism due to clozapine can lead to dyslipidemia-mediated-pancreatic-beta-cell damage, decreased insulin secretion as well as insulin resistance. In DKA, low levels of insulin lead to an increased release of free fatty acids from adipose tissue. Acetyl coenzyme A (CoA), derived from the breakdown of free fatty acids, is metabolized by the Kreb's cycle. In hepatocytes, excess acetyl-CoA is converted into ketone bodies (acetoacetate and β-hydroxybutyrate) and released into circulation. Ketone bodies have a low pKa value and their high serum concentrations lead to DKA. In this patient, DKA was most probably clozapine induced and had fatal consequences. Thus, recognizing potential risk factors, providing patient education, and increasing monitoring of patients on clozapine and other atypical antipsychotics are critical to prevent the life-threatening effects of DKA.
Introduction
Atypical or second-generation antipsychotic medications have become drugs of choice for treating schizophrenia, 1 due to their greater efficacy and safety as compared to first-generation antipsychotic medications.1–4 First-generation antipsychotic medications cause higher rates of extrapyramidal side effects (tremors, akathisia, muscle rigidity, etc) as well as tardive dyskinesia (hyperkinetic, involuntary face, and arm movements).1–6 However, atypical antipsychotics, specifically clozapine, used to treat refractory or treatment-resistant schizophrenia1,4,7–9 are associated with a significant increase of agranulocytosis and seizures when compared with first-generation antipsychotics.10,11 To prevent severe hematologic side effects, weekly complete blood counts with a differential count must be performed to detect any changes in white blood cell or absolute neutrophil count. 4 Consequently, many clinicians are reluctant to prescribe clozapine even when indicated, after failing trials of two atypical antipsychotics. 4 Seizures have occurred but are dose related and are managed with proper gradual dose titration or dose reduction in most patients. 12 Other notable side effects of clozapine and other atypical antipsychotic medications include significant weight gain, related metabolic problems, such as type 2 diabetes mellitus and the resulting lipid abnormalities, and disturbance of glucose regulation.6,13,14 In this report, we document a clinical case of apparent clozapine-induced fatal diabetic ketoacidosis (DKA).
History of Presenting Illness
An African–American male in his 20s with a medical history significant for schizophrenia, undifferentiated type, and aggressive behavior was presented to the psychiatric inpatient ward. He had been discharged from the psychiatric ward 15 months prior to this admission. During the previous admission, he was treated with fluphenazine (Prolixin®) for 2 months during which his symptoms, such as delusion, aggressive behavior, paranoia, and poor personal hygiene, had somewhat improved and he was discharged to a 24-hour residential care facility with court-ordered therapy. No reported medical problems were observed at that point of time. Later, the patient was petitioned for inpatient psychiatric care by his family members for the following reasons: disappearing for 8 days, physical assault, and stating that he was a demon while threatening to kill them. Furthermore, they reported cocaine and/or methamphetamine abuse.
Hospital Course
During his initial evaluation, the patient clearly met the criteria for schizophrenia as he had delusions, paranoia, bizarre disorganization of his thinking process, and auditory hallucinations. For example, when told his mother had petitioned him, he responded “I've got hundreds of moms, she's not even the right one. One will be mad if I don't pick her”. Moreover, the patient had poor hygiene, was very paranoid, and refused all voluntary medications and laboratory tests. Overall, he seemed to be in good physical health, otherwise with some mild tachycardia for which he was later prescribed metoprolol. Since the patient completely refused all medical interventions, antipsychotic medications were begun after obtaining a court order to administer therapy. Initially, 6 mg of risperidone per day (Risperdal®) showed no improvement (Fig. 1). After one week, divalproex sodium (Depakote®) was added in attempt to augment his antipsychotic symptoms (Fig. 2) without much success. On the second week, risperidone was discontinued (Fig. 1) and haloperidol (Haldol®) was added and titrated to 20 mg (10 mg twice a day) without improvement (Fig. 2). During the fourth week, olanzapine (Zyprexa®) was added and titrated up to 20 mg, which also did not induce improvement (Fig. 2). At that point, he remained paranoid, delusional, and isolated with poor hygiene.
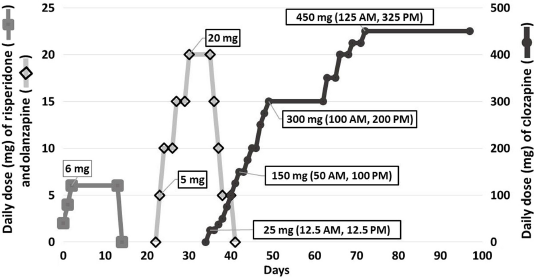
Atypical antipsychotics administered during the second hospitalization of the patient. First, risperidone was titrated to a therapeutic dose of 6 mg daily. The second medication administered was olanzapine titrated to 20 mg. After the patient failed to improve, he was started on a slow 40-day titration of clozapine.
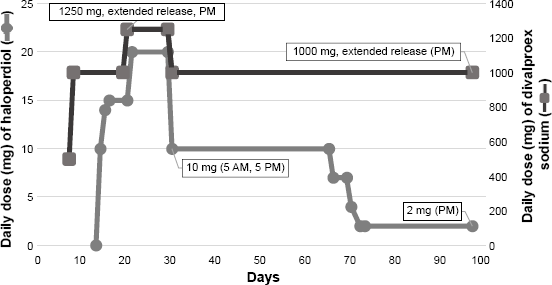
Concurrent haloperidol and divalproex sodium titration during the second hospitalization of the patient. Both medications were added as an adjunct therapy to control the patient's psychotic symptoms. After clozapine reached therapeutic levels, the haloperidol dose was significantly decreased from 10 mg to 2 mg with plans to be discontinued after being discharged.
After 1 month, a decision was made that, after having failed with two atypical antipsychotic (risperidone and olanzapine) without significant improvement in his clinical symptoms, the patient would be started on clozapine (Clozaril®). Consequently, the haloperidol dose was tapered down (Fig. 2), olanzapine dose was also tapered down and then discontinued, and clozapine titration was started during the fifth week of hospitalization (Fig. 1). As the clozapine dose increased, the patient finally showed some improvement in schizophrenic symptoms. He began tending to his hygiene with prompting and started leaving the psychiatric unit for meals and activities. He continued to show paranoia concerning blood draws, but agreed to accept them to be put on the discharge-ready list. On day 97 of his second hospital admission, the patient was discharged to the Assertive Community Treatment team for housing and continued monitoring of medication twice daily. His discharge medications included clozapine (125 mg AM, 325 mg PM), haloperidol (2 mg PM) with plans to be discontinued during outpatient treatment, divalproex sodium (extended release [ER] 1,000 mg PM), and metoprolol (50 mg AM, 100 mg PM). He was also given polyethylene glycol 3350 (Miralax™) for constipation.
Throughout the course of his hospital stay, no significant changes were observed in the patient's overall heath other than weight gain, early during his hospital stay (Fig. 3). This could be attributed to an improved dietary intake, as a result of eating regular meals at the psychiatric ward versus being semi-homeless, and/or more likely to olanzapine and clozapine administration as both medications can cause significant weight gain in some individuals.13,14 The hemoglobin A1c value during the first week was 5.1, fasting blood glucose level was 76, and the lipid panel indicated an low-density lipoprotein (LDL) level of 122. Urinalysis that was performed 6 weeks prior to discharge showed no glycosuria or ketones.
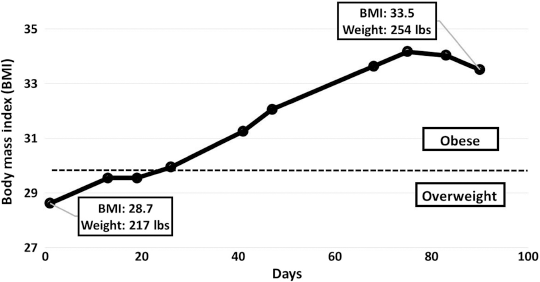
The patient's weight was checked throughout his care and his BMI increased significantly, while consuming olanzapine and clozapine, from 28.7 to 33.5. Fasting blood glucose from day 8 and multiple urinalyses showed no abnormalities suggestive of developing insulin resistance (data not shown).
Death and Toxicology
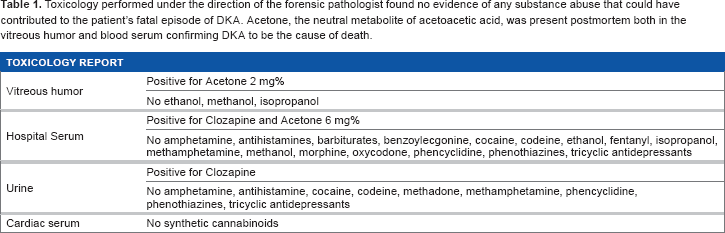
Six days post-discharge, the patient was found by a bystander unresponsive outside of his residence. While the precise duration for which the patient was unresponsive is unknown, Emergency Medical Services were called and attempts to resuscitate him were unsuccessful. Detailed notes concerning resuscitation efforts could not be obtained. While en route to the emergency department, his blood glucose level was checked and was found to be approximately 500 mg/dL. On medical autopsy, the forensic pathologist ruled that the cause of death was due to DKA without any evidence of significant contributory injuries or any other natural disease processes. The toxicology report was negative for all substances of abuse and common medications with the exception of clozapine and acetone, a known byproduct of the ketone bodies created during DKA (Table 1). 15 Notably, haloperidol, divalproex sodium, or metoprolol were not tested in the toxicology report. It is assumed that the patient was most likely taking his medications as prescribed due to twice-daily medication monitoring by his Assertive Community Treatment team case managers and stated desire to comply with his court-ordered therapy.
Toxicology performed under the direction of the forensic pathologist found no evidence of any substance abuse that could have contributed to the patient's fatal episode of DKA. Acetone, the neutral metabolite of acetoacetic acid, was present postmortem both in the vitreous humor and blood serum confirming DKA to be the cause of death.
Discussion
Clozapine treatment was initiated in an African–American schizophrenic male in his 20s after risperidone, olanzapine, and haloperidol failed to adequately control his psychotic symptoms. Clozapine treatment resulted in significant improvement in the patient's symptoms and also resulted in an increase in his body mass index (BMI). In this patient, both clozapine and olanzapine treatment resulted in significant weight gain and in an increase in BMI from 28.3 to 33.5. He was discharged for outpatient treatment on clozapine (125 mg AM, 325 mg PM) and haloperidol (2 mg PM) along with divalproex sodium and metoprolol dosages. The patient died unexpectedly six days after discharge, which was later found to be due to DKA.
After his death, it was found that the patient was severely hyperglycemic with a blood glucose level of 500 mg/dL. In normal physiology, glucose homeostasis is maintained by the regulatory effects of insulin and glucagon. Dietary glucose induces pancreatic beta cells to secrete insulin, which tips the metabolic scale toward lowering serum glucose levels via uptake by peripheral tissues. Although not completely understood, an altered metabolism due to clozapine can lead to dyslipidemia-mediated-pancreatic-beta-cell damage, decreased insulin secretion, and insulin resistance in some individuals.16–18 This process can significantly lower serum glucose clearing while promoting gluconeogenesis and lead to hyperglycemia. Another possible mechanism for insulin dysregulation could be related to the direct effects of the antipsychotic medications at the level of the glucose transporter proteins. 19 A study performed on rat muscle cells found that clozapine and other antipsychotic medications can act as non-competitive inhibitors of glucose transport. 19
Clozapine-induced aberrant insulin to glucagon ratio also stimulates lipolysis from adipose tissue. Excess acetyl-CoA, which is derived from the breakdown of free fatty acids, is converted into ketone bodies (acetoacetic acid and beta-hydroxybutyric acid) in hepatocytes and released into circulation. These ketone bodies are relatively strong acids and their high serum concentrations lead to ketoacidosis. High concentrations of blood glucose as well as ketone bodies cause osmotic diuresis and dehydration leading to hyperosmolar hyperglycemia and severe DKA. Clinically, patients present with an insidious onset of polyuria, polydipsia, tachypnea, and non-specific symptoms, such as nausea, vomiting, and abdominal pain. Later symptoms, include neurologic symptoms, such as lethargy, obtundation, seizure, focal deficits, coma, and ultimately death. In this patient, it is possible that the beta-blocker could have masked his initial presenting symptoms of hyperglycemia by blocking his body's sympathetic response to the acidosis.
Reports of DKA in patients consuming clozapine and other atypical antipsychotics are only recently being recognized as a preventable side effect of the medication.3,7,16,20 DKA is a serious and potentially fatal metabolic problem and a true endocrine emergency. In the patient described in this report, apparent clozapine-induced DKA had fatal consequences. Thus, recognizing potential risk factors, careful monitoring by clinicians of patients starting clozapine, and combining other atypical antipsychotics with proper education of patients are critical to prevent the life-threatening effects of DKA. For clinicians, current guidelines for all antipsychotics are to screen for diabetes mellitus risk factors (hemoglobin A1c and fasting blood glucose levels) 4 months after treatment. 21 Guidelines for clozapine administration, include monitoring for weight gain, glucose abnormalities, and hyperlipidemias. 21 We propose that in addition to obtaining a complete blood count with a differential count, fasting blood glucose level, and urinalysis (monitoring ketones) should be performed two to four times per month on all patients after initiating clozapine dosage. Clinicians should also identify patients with known risk factors (Table 2) before initiating any atypical antipsychotic and adjusting the testing schedule accordingly. Lastly, educating the patient on the signs and symptoms of DKA, namely acute onset polyuria, polydipsia, and tachypnea, is essential to detect DKA sufficiently early for proper life-saving medical intervention.
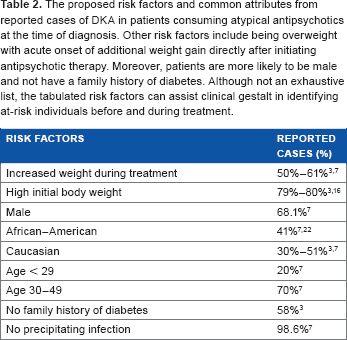
The proposed risk factors and common attributes from reported cases of DKA in patients consuming atypical antipsychotics at the time of diagnosis. Other risk factors include being overweight with acute onset of additional weight gain directly after initiating antipsychotic therapy. Moreover, patients are more likely to be male and not have a family history of diabetes. Although not an exhaustive list, the tabulated risk factors can assist clinical gestalt in identifying at-risk individuals before and during treatment.
Author Contributions
Conceived and designed the experiments: ER. Analyzed the data: ER, VJN and AK. Wrote the first draft of the manuscript: ER. Contributed to the writing of the manuscript: VJN and AK. Agree with manuscript results and conclusions: ER, VJN and AK. Jointly developed the structure and arguments for the paper: ER, VJN and AK. Made critical revisions and approved final version: ER, VJN and AK. All authors reviewed and approved of the final manuscript.