
Abstract
We report two children who developed hemiparesis secondary to cerebral infarcts complicating Lemierre syndrome. The first case is a one-year-old patient who presented a left internal jugular vein thrombosis and a left carotid compression due to retropharyngeal cellulitis. The second case is a five-year-old girl who presented a left internal jugular vein and a right carotid artery thrombosis associated with an oropharyngeal cellulitis. Etiologic agents involved were Staphylococus aureus in the first case and Fusobacterium necrophorum in the second case.
These cases call for vigilance among physicians for this rare syndrome, its unusual presentation and its associated severe complications.
Introduction
Lemierre syndrome is classically described as a septic thrombophlebitis of the internal jugular vein and is frequently associated with sepsis and metastatic infections, usually to the lungs and joints.(1,2) This syndrome usually follows an acute oropharyngeal infection. The etiologic pathogen of Lemierre syndrome is Fusobacterium necrophorum in over 80% of cases.(2) However, several other organisms have also been associated, with a much lower prevalence: Bacteroides, Streptococcus, Lactobacillus spp. and other Fusobacterium species.(1) This syndrome usually affects healthy adolescents or young adults but few cases involving young children have been described.(1,3,4) Although venous thrombophlebitis is a frequent clinical finding, involvement of the carotid artery leading to cerebral infarcts is rare.(4–8)
We describe two preschool children, who suffered ischemic stroke caused by carotid artery compression or thrombosis, an unusual complication of Lemierre syndrome.
Case #1
A healthy twelve-month-old boy presented to the emergency room with a week history of fever, cough and rhinorrhea. A left cervical mass had appeared on the day of presentation. On evaluation, he was febrile, non toxic and had no respiratory distress or hypersalivation. His laboratory results revealed a WBC count of 20.6 × 10 9 /L. The initial diagnosis was cervical adenitis. He was admitted and started on IV Cefotaxime. In the hours following admission, he developed a respiratory distress caused by an upper respiratory tract obstruction. A lateral X-ray of the neck revealed a retropharyngeal mass. The patient was intubated and the retropharyngeal mass was drained. He was transferred to the Pediatric Intensive Care Unit (PICU) where he developed a right hemiparesis.
A CT-Scan done on the same day revealed an extensive retropharyngeal cellulitis with obliteration of the left internal jugular vein and carotid artery from the mandibular angle. An angiography revealed a thrombosis of the left internal jugular vein up to the foramen, confirming Lemierre syndrome (Fig. 1). The left carotid artery was compressed by the inflammatory process, although no thrombus or pseudoaneurysm was identified (Fig. 2). A cerebral CT scan showed a hypodensity zone in the left parietal lobe compatible with an arterial ischemic event. No intracranial hemorrhage was identified, and the patient was put on low molecular weight heparin for 3 months.

Case 1. Late venous opacification during cerebral angiography showing the absence of opacification on the left side (L) due to internal jugular vein thrombosis, compared to normal flow through the right side (R).

Case 1. Arterial angiogram (aortic arch injection) showing obstruction of the internal carotid artery on the left side (L) compared to normal vascularisation on the right side (R).
Cultures from the retropharynx grew Staphylococcus Aureus; blood cultures remained negative. The patient never developed a clinical picture of sepsis, metastatic lung infection or joint infections. He was treated with IV antibiotics for 6 weeks. He completely recovered form his right hemiparesis within 3 months.
Case #2
A five year old girl travelling from Asia, with no past medical history, presented at the emergency room with a five day history of fever and neck pain. She had difficulties eating, refused to walk and showed increased drowsiness. She presented with shock, initially necessitating fluids and vasopressors. She had no respiratory distress. The rest of her physical exam was significant for nuchal rigidity and tender neck muscles. A lumbar puncture was deferred because of thrombocytopenia and disseminated intravascular coagulation (DIC). A CT-Scan of the neck revealed a retropharygeal cellulitis (Fig. 3); the cerebral CT-Scan was normal. She was started on IV cefotaxime, vancomycin and penicillin.

Case 2. Neck CT-Scan displaying the extension of cellulitis in the retropharyngeal area (dotted line).
The patient's hemodynamic state and DIC improved within 24 hours. However, on day 2 of her hospital stay, she developed stridor and respiratory distress secondary to upper airway obstruction, for which intubation was required. She was brought to the operating room, where surgeons noted a progression of her retropharyngeal cellulitis, but no drainable abscess. Myringotomy tubes were put in place and cultures of her associated middle ear effusions were taken. These effusions eventually grew Fusobacterium necrophorum. Another neck CT-Scan done on day 2 showed a left internal jugular vein thrombosis, compatible with Lemierre syndrome (Fig. 4). The patient was started on IV heparin.

Case 2. Neck CT-Scan displaying the jugular venous thrombosis on the left side (white arrow).
Over the following days she developed a left hemiparesis and worsening of her facial swelling. An MRI done on day 4 showed ischemic lesions in the right carotid artery territory (right frontal lobe, periventricular region of the right ventricle, head of the right caudate nucleus) as well as in the right vertebral artery territory (right cerebellar hemisphere and right occipital lobe). (Fig. 5) The MRI also showed increased inflammation and infection in the retropharyngeal and neck tissues as well as atlanto-axial subluxation and suspicion of a cervical C1–C2 osteomyelitis. A cerebral angiography revealed an important narrowing of the intra-petrous portion of the right carotid and a partial occlusion of the distal internal right carotid. The left internal carotid artery was also narrowed, but the intracerebral vessels on that side were normal. The angiography also confirmed a thrombosis of the left transverse and sigmoid sinuses and the left internal jugular vein.
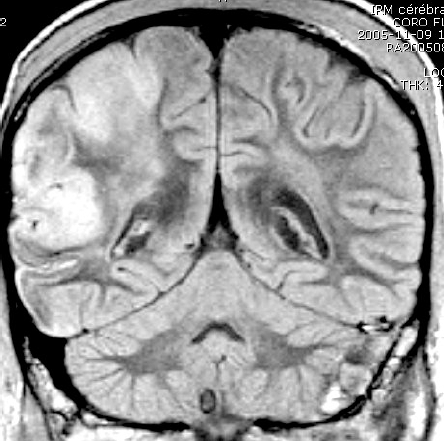
Case 2. Cerebral MRI displaying the extensive involvement of the right hemisphere.
On day 7, the patient was brought back to the operating room for drainage of the infectious process, since fever reappeared and her general as well as neurologic status deteriorated under maximal medical treatment. The surgery included a left mastoidectomy, drainage of retropharyngeal and peri-tonsillar abscesses, a bilateral maxillary sinusotomy, an ethmoidal sinusotomy and sphenoidotomy, a cervical dissection of infected tissue and a ligature and removal of the left internal jugular vein with anastomosis at the level of the jugular foramen.
The patient's general condition improved gradually and she was extubated on day 25. She received a total of 8 weeks of IV antibiotics. A complete thrombotic workup was done and results were negative. Heparin was stopped before the surgery, and the patient was put on Aspirin. After 3 months of intensive treatment and rehabilitation, the patient was flown back to a rehabilitation center in her home country. Six months after the events she had improved enough to be able to walk and to start using her left arm. She still needed a cervical collar to assure stability of her cervical spine.
Discussion
These two cases presented an unusual complication of Lemierre syndrome: hemiparesis caused by a cerebral infarct. The first patient had a compression of the left carotid artery by the localized inflammation. The second patient presented an extensive carotid thrombosis. Interestingly, the arterial thrombosis was on the opposite side of the jugular thrombophlebitis. Only one case of carotid artery involvement leading to a cerebral infarct in Lemierre syndrome has been reported in the pediatric literature and the patient was 15 years old.(5) Another pediatric patient presenting a carotid artery pseudoaneurysm secondary to an oropharyngeal infection has been reported; fortunately this patient did not develop a cerebral infarct.(9) There are also some reports of adult patients presenting a cerebral infarct in association with Lemierre syndrome but none of these presented a carotid compression or thrombosis as the pathophysiological explication.(4,6–8) The two cases of Lemierre syndrome described here are unique in different ways: 1) the patients are younger than the vast majority of cases reported in the literature; 2) cerebral infarct due to carotid involvement constitute a rare complication that has never been reported in patients that young; 3) the youngest case was infected with Staphylococcus aureus, an unusual pathogen seen in this syndrome.
Classically, Lemierre syndrome progresses in an orderly fashion. Patients first get a primary infection, usually pharyngitis, which is followed by local invasion of the lateral pharyngeal space and an internal jugular vein septic thrombophlebitis. This thrombophlebitis then causes metastatic complications, mainly septic emboli to the lungs and joints.(2) The exact mechanism of the unusual arterial involvement described in our two patients is unclear. It is possible that the low pressure venous flow in the internal jugular vein generally favours venous thrombosis formation while the high pressure arterial flow prevents thrombosis of this vessel. Nevertheless, it is also possible that young children may have a higher predisposition to arterial involvement due to the smaller diameter of their vessels.
Why this complication has been rarely reported in the past is also unclear. It is possible that some patients present only partial occlusion of their carotid artery without being symptomatic and therefore are not diagnosed. Furthermore, the historical less intensive use of radiological imaging to reveal involvement of vascular structures can be a plausible reason. Nowadays, the more frequent and early use of CT-Scan and MRI in the clinical course of patients with oropharyngeal cellultis can help diagnose these complications more accurately.
Cerebral infarct may be rare but emphasizes the need for early diagnosis and a high index of suspicion for carotid artery involvement in patients with oro-pharyngeal infections. Too few cases have been reported to demonstrate that early antibiotic treatment could prevent carotid artery involvement; neither can we recommend an early surgical exploration strategy. However, although no controlled study to assess the value of anticoagulation in septic thrombophlebitis of the neck is available(2) and even if the role of anticoagulant therapy in the management of jugular thrombophlebitis remains controversial, a combination of antibiotic and anticoagulant therapy is generally considered the mainstay of therapy(10) and may help avoid surgery.(1) The latter is reserved for disease unresponsive to medical therapy. Sino-venous thrombosis is an indication for anticoagulant therapy, whether in the context of infection or not.(10–12)
Lemierre syndrome seems to have a predilection for teenagers and young adults. Seventy-three percent (73%) of the cases of Lemierre syndrome have been described in patients aged 16–25 years.(2) A review of the literature published by Alvarez et al. in 1995 reported 14 pediatric cases (children under the age of 18) since 1945. The youngest was 11 years old.(13) The cases reported here are one of the few cases of Lemierre syndrome involving young children.(1,3,4)
The etiologic agent identified in Lemierre syndrome is Fusobacterium necrophorum in 81% of cases.(2) However, several other anaerobic bacteria as well as Streptococcus species and Staphylococcus epidermidis have been reported to be associated with Lemierre syndrome.(2) We found only one case of Lemierre syndrome associated with Stahylococcus Aureus(3), this was in a 7-month-old patient. This finding leads us to think that Lemierre syndrome may be caused by different bacteria in the very young child.
In conclusion, Lemierre syndrome is a rare disease. However, its epidemiology and pathophysiology in pediatric patients is only starting to be characterized. We believe that physicians need to have a high index of suspicion in patients presenting an unusual evolution of oropharyngeal infection, even in young patients and in the absence of identification of Fusobacterium necrophorum. Cerebral infarct can be associated with Lemierre syndrome and can cause important complications like hemiparesis. Compression or thrombosis of the carotid artery should be evaluated promptly when this complication is suspected, particularly in preschool children with Lemierre syndrome. Even though the best therapy to limit the extent of the complications associated with Lemierre syndrome still needs to be defined, early recognition and initiation of therapy is desirable.