
Abstract
Caspofungin is the first member of the echinocandin class of antifungals to receive an indication for the use in infants, children, and adolescents from the United States Food and Drug Administration. Daily doses of 50 mg/m2 result in pharmacokinetic parameters that are similar to those observed in adults. Although fewer data are available, the response rates in pediatric patients who received caspofungin either as treatment or empiric therapy in clinical trials are similar to those reported in adults. In addition, caspofungin appears to be generally safe and well tolerated in this population. This represents a significant step forward in the treatment of invasive fungal infections within this population, as caspofungin is associated with few clinically significant drug-interactions and toxicities compared to other antifungals, such as the azoles and amphotericin B.
Keywords
Introduction
Invasive fungal infections are a growing complication in preterm neonates and immunocompromised pediatric patients. In the adult population, the incidence and treatment of these infections have been well documented and treatment guidelines are available for many invasive mycoses. 1 However, this has not been the case in the pediatric area where there are currently no treatment guidelines that specifically address this population with regards to invasive fungal infections. 2 Indeed, most therapeutic recommendations for pediatric patients are extrapolated from clinical trials conducted in adults. 3 In addition, there is a wide variation in the diagnostic methods used to establish the presence of invasive fungal infections in pediatric patients. Blood cultures are considered the gold standard for diagnosis of candidiasis, but have low sensitivity and are subject to delays in reporting. 4 Delays in the diagnosis of these infections may result in long-term consequences as early detection and initiation of appropriate antifungal therapy contribute to the successful management of invasive mycoses. Indeed, neurodevelopmental outcomes have been related to the initiation of antifungal therapy in pediatric patients as improved outcomes have been observed when treatment was started early.4–6 The response to antifungal therapy in children can vary depending on the age of patients. In preterm neonates, responses to treatment and favorable outcomes may be hindered by both impaired neutrophil Chemotaxis and bactericidal activity, while children undergoing high dose chemotherapy can have variable T-cell recovery depending on their age. 7
In the United States Candida species are the fourth most common cause of nosocomial bloodstream infections and are associated with significant mortality.8,9 Compared to hospitalized adults, children have a higher incidence of nosocomial candidemia, but an overall lower mortality rate. 10 However, these infections in pediatric patients are associated with significant increases in both the length of stay as well as per patient hospital charges compared to adults. 10 The most commonly isolated pathogen in both children and adults is Candida albicans. In pediatric patients, especially those less than 2 years of age, this is followed by C parapsilosis. As they become older and move into adolescence the causative agents of candidiasis change, and the incidence of infections caused by C. glabrata increases and this species becomes the second most commonly isolated pathogen.10,11 Highly immunocompromised pediatric patients are at risk for invasive aspergillosis, including those receiving chemotherapy for hematologic malignancies, patients receiving high doses of corticosteroids, neutropenic patients, and recipients of hematopoietic stem cell transplants. Currently, very little is known about the incidence of other invasive fungal such as mucormycosis and cryptococcosis within this population. 11
In the United States fewer medications are approved by the Food and Drug Administration (FDA) for use in children than in adults. Due to the difficulty in conducting pediatric clinic trials and the lack of return on investment, most medications lack sufficient pediatric pharmacokinetic/pharmacodynamic data as well as safety and efficacy studies. To encourage manufacturers to undertake clinical studies, the FDA has granted a 6-month market exclusivity to the first company that conducts the required clinical studies and obtains approval for the pediatric indication. A provision in the law allows if the disease and the effect of the drug are similar in adults and pediatric patients, the pediatric effectiveness can be extrapolated from “adequate and well-controlled studies in adults” with supplementation of other information (pharmacokinetic data) obtained in pediatric patients. 12 Also, a study in each age group may not be needed if data from one group can be extrapolated to another. These provisions allow for faster time to approval. In the United States antifungals that have a pediatric indication for the treatment of invasive fungal infections include the azoles fluconazole and voriconazole, and the pyrimidine 5-flucytosine. Other agents that are frequently used in this population include the polyene amphotericin B deoxycholate and the lipid formulations of this agent. These antifungals are often associated with significant toxicities and drug-interactions due to non-specific interactions with mammalian cell membranes and cytochrome P450 enzymes. The echinocandins, which include anidulafungin, caspofungin, and micafungin, have been a welcome addition to the antifungal armamentarium. Currently, caspofungin is the only enchinocandin with a pediatric indication in the United States. The purpose of this review is to discuss the pharmacology and spectrum of activity caspofungin as well as the pharmacokinetics, clinical efficacy, and safety profile of this echinocandin in pediatric patients.
Pharmacology
Mechanism of action
The fungal cell wall of Candida and Aspergillus species are composed of mannoproteins on the exterior surface, β-glucans, and chitin, which serves as an anchor to the cell membrane. The polysaccharide (1,3)-β-D-glucan, which is synthesized by the glucan synthase complex anchored to the cell membrane, is found in abundance within the cell wall and helps to provide shape and integrity. The echinocandins non-competitively inhibit the synthesis of these polymers leading to osmotic instability and eventually cell lysis.13,14 Inhibition of the glucan synthase complex is an attractive target due to the lack of homologous enzymes in human cells, thus affording a high degree of selectivity for fungi with few toxicities and clinically relevant drug interactions that are associated with amphotericin B formulations and the azoles. As the glucan synthase complex is located at the growing apical tips and branch points of hyphae in Aspergillus species, exposure to caspofungin results in the inhibition of (1,3)-β-D-glucan synthesis at these sites.13,15,16 Morphologically, this leads to swollen apical tips and abnormally branched, stubby hyphae.
Spectrum of activity
Caspofungin, like each member of this class, is a relatively broad-spectrum antifungal agent with activity against Candida species, Aspergillus, and mycelial forms of endemic fungi.17–25 Caspofungin has also been shown to maintain activity against azole-resistant Candida isolates. 26 However, concerns regarding the development of co-resistance between the azoles and the echinocandins in C glabrata isolates have arisen.27,28 Reduced in vitro potency has been reported for each member of this class against Candida parapsilosis and Candida guillermondii. However, there are notable holes in the spectrum of activity of the echinocandins, and this includes Cryptococcus species, Fusarium species, and the causative agents of mucormycosis (eg, Rhizopus, Rhizomucor, Mucorales, and Cunninghamella).
Mechanism of resistance
Numerous case reports have been published describing clinical failures with the echinocandins that are associated with elevated MIC values in patients with invasive infections caused by C albicans, C glabrata, C parapsilosis, C tropicalis, and C krusei.29–35 This rise in echinocandin MIC values has been linked to mutations in the FKS1 and FKS2 genes, which encode portions of the β-glucan synthase enzyme,32,33 and this is consistent with in vitro studies that have also reported reduced echinocandin activity with point mutations in these genes.36,37 In C albicans and C glabrata the majority of the mutations reported resulted in an amino acid change from serine at positions 645 and 663, respectively, of the glucan synthase enzyme.36,38 In C parapsilosis a naturally occurring amino acid change is present within the glucan synthase enzyme, which explains the reduced potency of this class of antifungal against this Candida species. 39 Many of the case reports of caspofungin clinical failures have described progressive increases in MIC values for each echinocandin after an extended period therapy in patients with multiple comorbidities.29,34 Thus, mutations in FKS1 and FKS2 appear to confer resistance for each echinocandin and are not specific for a particular member of this class. It is unknown if other mechanisms that have been reported to cause reduced echinocandin in vitro activity, such as over-expression of the Golgi protein Sbe2p involved in cell wall component transport, 40 upregulation of the cell wall integrity pathway, 41 or increases in chitin concentrations in the cell wall, 42 may also be of clinical significance as mutations in FKS1 and FKS2 have not always been reported with elevated echinocandin MICs.29,30 Despite increases in the number of case reports of echinocandin clinical failure associated with elevations in MIC values, surveillance studies have not revealed a significant change in the activity of the echinocandins against Candida species, and the incidence of clinical failure associated with microbiological resistance is very low.43–46
Pharmacodynamics
The echinocandins demonstrate concentration dependent activity. Against Candida species, this activity is fungicidal in vitro, and time-kill studies against different species have reported a >3 log10 reduction in colony-forming units per mL from the starting inoculum following exposure to the echinocandins. 47 However, this has not been consistently demonstrated in all studies as static activity has been reported against some Candida clinical isolates. 48 In the presence of serum or albumin the activity of the echinocandins is reduced, and this reduction in potency has been demonstrated using different in vitro assays, including microbroth susceptibility testing, the XTT colorimetric viability assay, and time-kill studies.49–51 This is likely due to the high protein binding of these agents leading to a reduction in the free fraction that is able to inhibit (1,3)-β-D-glucan synthase activity. 52 Animal studies have also reported concentration-dependent activity for the echinocandins against infections caused by Candida and Aspergillus species. In a murine model of disseminated candidiasis caused by C glabrata, the pharmacokinetic/pharmacodynamics (PK/PD) parameter most closely associated with reductions in tissue fungal burden for caspofungin was the area under the concentration curve to minimum inhibitory concentration (AUC/MIC) ratio, followed closely by peak to MIC (Cmax/MIC) ratio. 53 Concentration-dependent activity has also been observed with caspofungin in a murine model of invasive pulmonary aspergillosis where the Cmax/MEC ratio was associated with significant reductions in pulmonary fungal burden. 54
Pharmacokinetics
The pharmacokinetic profile of caspofungin in children and adolescents has been extensively evaluated. This was accomplished using a staged approach with the first study evaluating the pharmacokinetics and safety of this echinocandin in children and adolescents 2 through 17 years of age. 55 In this multi-center, open-label, sequential-dose escalation study, 39 clinically stable pediatric patients with a history of underlying hematological or solid-organ malignancy, hematopoietic stem cell transplantation, or aplastic anemia received caspofungin with the primary goal of identifying a dosing regimen that yielded plasma concentrations similar to those observed in adults. The pharmacokinetic values measured in children and adolescents were then compared to those obtained in adult patients with mucosal candidiasis at doses of 50 or 70 mg/day56–58 Initially, patients were enrolled into a weight based (1 mg/kg/day) regimen, and weight based strategies are currently used for micafungin and anidulafungin in pediatric patients. 59 However, the overall caspofungin exposure with the weight-based strategy, as measured by the area under the concentration curve from 0 to 24 hours (AUC0–24), was found to be substantially lower than that obtained in adults at a daily dose of 50 mg (56.3 μg × hr/mL versus 103 μg × hr/mL). Based of this finding, the study was amended to evaluate dosing based on body surface area (BSA) at doses of 50 and 70 mg/m2/day up to a maximum of 70 mg/day. In children the AUC0–24 obtained with multiple 50 mg/m2 doses was similar to that observed in adults. However, the plasma concentration of caspofungin obtained 1 hour after the end of the infusion (C1 hr) was higher in children compared to adults while he trough level obtained 24 hours after the dose (C24 hr) was lower. These findings were explained by the faster rate of decline in the plasma concentration-time profile in children as evident by the shorter β-phase half-life (8.2 hours) compared to adults (13 hours). In adolescents, each of the pharmacokinetic parameters (AUC0–24, C1 hr, C24 hr, and β-phase half-life) was similar to those in adults who received doses of 50 mg/day. Most of the adolescent patients (6 of 8) received the maximum dose of 70 mg/day and all received doses of >50 mg/day.
Following this study in children and adolescents, a second study was conducted to assess the pharmacokinetics of caspofungin in infants and toddlers. 60 In this multicenter, open-label study, infants and toddlers between the ages of 3 and 24 months with leukemia, lymphoma or other cancers, bone marrow or peripheral stem cell transplantation, high-dose chemotherapy, or aplastic anemia were eligible if they were neutropenic (absolute neutrophil count < 500/mm3) and had at least one fever > 38 °C. Nine patients were enrolled and each received caspofungin at a dose of 50 mg/m2/day The pharmacokinetic parameters measured in these younger patients were then compared to those obtained in older children (2–11 years) and adolescents (12–17 years) who received doses of 50 mg/m2/day from the trial described above, 55 as well as adults with mucosal candidiasis who received caspofungin at doses of 50 or 70 mg/day.56,57,61 Following multiple doses, the plasma concentration profile of caspofungin in infants/toddlers was similar to that observed in children and adolescents. Similar to what was observed in children age 2–11 years, higher C1 hr plasma concentrations were measured in these younger children (17.21 μg/mL) compared to adults (9.39 μg/mL) while the C24 hr concentration (1.64 μg/mL) was lower (2.01 μg/mL), although this difference was not statistically significant. These observations of higher C1 hr and lower C24 hr concentrations are consistent with the shorter β-phase half-life observed in these younger patients (8.80 hours). Interestingly, the AUC0–24 was statistically higher in infants/toddlers (130.39 μg × hr/mL) than in adults (103.38 μg × hr/mL). The exact reason for the differences in C1 hr, C24 hr and β-phase half-life pharmacokinetic parameters observed between children and adults in these two studies is unclear. The authors speculated that these differences may be due to changes in expression levels of uptake transporters during the course of developmental maturity, such as the OATP1B1 transporter that may be involved in the hepatic uptake of caspofungin, 62 as well as differences in physiological factors such as blood flow rates and organ sizes that may change caspofungin clearance with age. However, it is unlikely that these differences are clinically significant as the steady-state exposures of caspofungin (ie, AUC0–24) are similar among the different age groups. The pharmacokinetic parameters found in children and adolescents from these two studies, as well as those from adults are shown in Table 1.
Pharmacokinetic parameters (arithmetic mean ± standard deviation) of caspofungin in patients 3 months-17 years of age and adults.

It should be noted that in these two pharmacokinetic studies in infants/toddlers and children and adolescents a loading dose was not administered. However, the administration of a loading dose of 70 mg/m2 on the first day of therapy is recommended in the package insert. 63 In the clinical trials that evaluated the efficacy of caspofungin for the treatment of invasive fungal infections or as empiric therapy in the setting of febrile neutropenia children and adolescents did receive a loading dose followed by daily maintenance therapy.64,65 Although these published studies did not report plasma concentration data, the pharmacokinetic parameters from these studies were reviewed by the US FDA when approval of caspofungin was sought in pediatric patients. 66 As also shown in Table 1, each of the three pharmacokinetic parameters was elevated in children and adolescents who received a loading dose of this echinocandin. The reasons for this remain unclear as the administration of a loading dose should not influence plasma concentrations once steady-state is achieved. It was noted that this difference in steady-state pharmacokinetic parameters between pediatric patients who did and did not received loading doses of caspofungin was not expected to be clinically important as the rates of adverse events reported in the studies that used a loading dose in pediatric patients were similar to those previously observed in adults.64–66
Following the completion of these studies in which plasma concentrations of caspofungin were measured in pediatric patients, a retrospective review was conducted to determine if there was a correlation between treatment outcomes and pharmacokinetic parameters. 67 In this study, the pooled clinical response data from the 125 pediatric patients who were enrolled in the two phase I studies and two efficacy trials were evaluated in relation to caspofungin pharmacokinetic parameters and the incidence of adverse effects.55,60,65,68 This included 32 patients with invasive candidiasis, 10 with invasive aspergillosis, and 82 who received empiric therapy in the setting of febrile neutropenia. The effects of patient characteristics and concurrent medications on caspofungin pharmacokinetics were also evaluated. Of the three pharmacokinetic parameters that were evaluated (AUC0–24, C1 hr, and C24 hr), none were found to be significantly associated with clinical outcome. In addition, when the in vitro activity of caspofungin against the isolates collected from these patients was included in this analysis, none of the three pharmacokinetic/pharmacodynamic parameters (AUC0–24/MIC, C1 hr/MIC, and C24 hr/MIC) was found to be a significant factor for predicting clinical or microbiological response. Interestingly, new onset fever and neutropenia were associated with moderate decreases in caspofungin exposure (25% reduction in AUC0–24) and trough levels (35.9% reduction in C24 hr) compared to patients with persistent fever and neutropenia. Greater pharmacokinetic variability also appeared higher in those who weighed less compared to heavier patients. Three medications were associated with statistically significant reductions in caspofungin pharmacokinetic parameters in these patients: dexamethasone and vancomycin, which reduced caspofungin trough levels, and acyclovir, which was found to result in decreased C1 hr concentrations. The reduced concentrations associated with dexamethasone use are consistent with the changes in caspofungin levels observed in adults who are receiving concomitant inducers of drug clearance. There were no associations between pharmacokinetic parameters and clinical adverse effects, and only ALT > 2.5 times the baseline value and caspofungin C24 hr concentrations was found to be statistically significant.
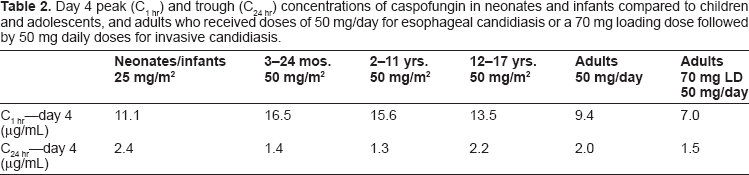
The pharmacokinetics of caspofungin have also been evaluated in neonates and infants. In this small study, patients less than three months of age who were receiving an intravenous amphotericin B formulation for invasive candidiasis were enrolled to receive either a single dose (n = 6) or multiple doses (n = 12) of caspofungin at 25 mg/m2. 69 Peak (C1 hr) and trough (C24 hr) plasma concentrations were then measured either on day 1 or day 4 of therapy. Thirteen of the eighteen patients enrolled had a gestational age of <36 weeks. The levels that were achieved were then compared to those previously measured in adults,56,57,61,70 as well as children and adolescents.55,60 The peak concentrations of caspofungin in neonates and infants were similar to those achieved in adults with esophageal candidiasis both on day 1 and day 4, but were moderately higher than those observed in adults with invasive candidiasis (Table 2). In contrast, trough concentrations in this young population were elevated compared to adults who received caspofungin for either indication. Compared to children and adolescents, caspofungin peak concentrations were lower in neonates and infants, while trough concentrations were somewhat increased. It should be noted though that the dose used in neonates and infants (25 mg/m2) was half that used in children and adolescents (50 mg/m2). These results are consistent with the reduced clearance in neonates and infants relative to older pediatric patients, and that clearance of this echinocandin may increase from infancy to childhood. Although a high rate of clinical and laboratory adverse events was observed in this study, this was expected due to the nature of this population, and none of these adverse effects was considered by the investigators to be due to caspofungin. Interestingly, a reduction in hemoglobin was the most common laboratory adverse event. However, no patients discontinued caspofungin due to this or any other laboratory adverse events.
Day 4 peak (C1 hr) and trough (C24 hr) concentrations of caspofungin in neonates and infants compared to children and adolescents, and adults who received doses of 50 mg/day for esophageal candidiasis or a 70 mg loading dose followed by 50 mg daily doses for invasive candidiasis.
Drug Interactions
One of the main advantages of the echinocandins, including caspofungin, is the drug interaction profile. As each echinocandin is neither a substrate nor inhibitor or inducer of mammalian cytochrome P450 enzymes, there are few clinically significant drug interactions associated with members of this antifungal class. This is in contrast to the azoles, which are associated with numerous drug-interactions as most of the members of this class are both substrates and inhibitors of cytochrome P450 enzymes. Most of the data regarding drug interactions with the echinocandins have come from healthy volunteer studies in adults. Increases in serum aminotransferase levels have occurred in those receiving cyclosporine and caspofungin, and cyclosporine has also been reported to increase the AUC of caspofungin by approximately 35%.71,72 This interaction is not specific to caspofungin as similar increases in AUC levels have also been reported for micafungin. 73 In contrast, tacrolimus concentrations may be decreased when administered concurrently with caspofungin but not micafungin.72,74 This interaction between caspofungin and tacrolimus may require more frequent monitoring of serum levels of this calcineurin inhibitor. 72 Although caspofungin is not a substrate of cytochrome P450 enzymes, logistic regression modeling has suggested that concomitant administration of inducers of metabolism, such as efavirenz, nevirapine, phenytoin, dexamethasone, or carbamazepine, may reduce caspofungin concentrations. Additionally, a 30% decrease in caspofungin trough concentrations has been observed in healthy volunteers who were began to receive rifampin 14 days prior to the initiation of caspofungin. 72 The exact mechanism of this interaction is unknown, but may be due to an induction of uptake transporters, such as Oatp1 and Oatp2, by rifampin.75,76 Few drug interactions have been reported with caspofungin in pediatric patients. As previously described, reductions in caspofungin trough concentrations were observed with concurrent use of dexamethasone and vancomycin, and acyclovir resulted in decreased peak bloodstream concentrations in pharmacokinetic studies of caspofungin in pediatric patients. 67 The clinical significance of these interactions is unknown.
Clinical Efficacy
Few clinical studies have evaluated the efficacy of caspofungin in pediatric patients as either treatment for established infections or as empiric therapy in the setting of neutropenic fever. Zaoutis et al conducted a prospective, multi-center, open-label study of caspofungin in children and adolescents as therapy against invasive candidiasis or aspergillosis. 64 Patients age 3–16 years received caspofungin, dosed at 70 mg/m2 on the first day followed by 50 mg/m2 daily thereafter as either primary or salvage therapy against invasive candidiasis, or as salvage therapy against invasive aspergillosis. Response to therapy was measured at the end of caspofungin therapy. Ten patients with invasive aspergillosis, 38 with invasive candidiasis, and one with esophageal candidiasis were enrolled. One of the invasive candidiasis patients was excluded due to an infection with a Trichosporon species rather than Candida. Five of the patients who received salvage therapy for invasive aspergillosis had a favorable response at the end of therapy, 3 of which were judged to be a complete response. The five patients who failed to respond were either neutropenic at study entry or received chemotherapy, and each died despite treatment with caspofungin or other antifungal therapy. Favorable responses were observed in 81% of patients with invasive candidiasis, with similar rates between those that received caspofungin as primary (25 of 30) or salvage therapy (5 of 7). Patients whose infections were caused by C. parapsilosis responded well with 7 of 8 having a favorable outcome at the end of therapy. Complete resolution of oro-esophageal lesions occurred in the one patient with esophageal candidiasis, and only one patient with either invasive aspergillosis or invasive candidiasis had a relapse within 28 days of completing therapy. A similar response rate was reported for micafungin against invasive candidiasis in a pediatric sub-study that compared this echinocandin to liposomal amphotericin B. 77 The favorable response rates observed in this open-label study are similar to those previously reported for adults who received caspofungin as salvage therapy for invasive aspergillosis (48%) and as primary therapy for invasive candidiasis (74%) (Fig. 1).70,78

Favorable response rates in children and adolescents compared to adults who received caspofungin either as treatment for invasive or esophageal candidiasis, or as salvage therapy against invasive aspergillosis.
Caspofungin has also been evaluated as empiric therapy in pediatric patients with febrile neutropenia. In a prospective, multi-center, double-blind study, patients age 2–17 years that were receiving cancer chemotherapy or had undergone a hematopoietic stem cell transplant and had persistent neutropenia (absolute neutrophil count < 500/mm3 for 96 hours) and were febrile despite broad-spectrum antibacterial therapy were randomized to receive either caspofungin (70 mg/m2 loading dose followed by daily doses of 50 mg/m2) plus placebo, or liposomal amphotericin B (3 mg/kg/day) plus placebo. 65 Efficacy was based on a composite endpoint that included: (1) successful treatment of any baseline fungal infection based on the assessment of the Adjudication Committee, (2) absence of any breakthrough fungal infection during therapy or within 7 days of completing therapy, (3) survival for 7 days after completion of therapy, (4) no premature discontinuation of therapy due to drug-related toxicity or lack of efficacy, and (5) resolution of fever for at least 48 hours during neutropenia. A total of 83 patients were randomized, and 81 were included in the modified intent-to-treat population that was used to evaluate efficacy. A favorable overall response was observed in 46.4% of those randomized to caspofungin and 32% of those who received liposomal amphotericin B. Among high-risk patients, defined as those who had undergone an allogeneic bone marrow or peripheral blood stem-cell transplantation or had received chemotherapy for a relapse of acute leukemia, favorable responses were observed 9 of 15 (60%) who received caspofungin and in none of the 7 patients who received liposomal amphotericin B. Overall, the favorable response rates observed these pediatric patients were similar to those reported in a study of adults who received empiric therapy with either caspofungin (33.9%) or liposomal amphotericin B (33.7%). 79 As fever may neither be a sensitive or specific indicator of invasive fungal infections, some have suggested removing resolution of fever from the composite endpoint in empiric therapy trials. 80 In this study, both the caspofungin and liposomal amphotericin B groups had progressive increases in overall favorable response rates as the definition of fever became less conservative and reached 89% for caspofungin and 84% for liposomal amphotericin B recipients when resolution of fever was completely removed from the composite endpoint.
Although the efficacy of caspofungin has not been evaluated in neonates in clinical trials, case-series have reported that this agent may be effective within this population. In one case-series from a single-center, caspofungin monotherapy was used as salvage therapy in 10 neonates, 9 of which were born premature (mean gestational age 33 weeks), who had persistent candidemia despite the administration of amphotericin B deoxycholate. 81 Two of the patients also developed disseminated candidiasis while on amphotericin B and one experienced both infusion-related and renal toxicities secondary to this polyene. After the initiation of caspofungin, blood cultures cleared in all patients within three to seven days. An atrial vegetation secondary to C parapsilosis resolved after 9 days of caspofungin in one patient, and renal Candida bezoars were cleared after 19 days of therapy in another. No clinical or adverse effects were reported in these patients. Other case reports have also reported the successful treatment of persistent candidemia and Candida septicemia with caspofungin monotherapy in neonates.82,83
Caspofungin was also reported to be effective as part of combination therapy in neonates with persistent candidemia. In this single center retrospective review, caspofungin was added to antifungal therapy that included a lipid formulation of amphotericin B either as monotherapy or already combined with fluconazole or flucytosine, in 13 infants with persistent candidemia who were in the neonatal intensive care unit, 12 of whom were premature (median gestational age 27 weeks). 84 Microbiological sterilization of the blood cultures occurred in 11 of the 13 patients within 1 to 21 days of caspofungin initiation. Recurrent infections with the same Candida species occurred in 3 of these patients after caspofungin was discontinued. Two of these patients were again treated with caspofungin and achieved microbiological clearance. These results were compared to 11 patients in the neonatal intensive care unit with persistent candidemia who did not receive caspofungin therapy. Microbiological clearance of the blood cultures was achieved in 5 of these control patients.
One study has also evaluated the effectiveness of combination therapy with caspofungin in severely immunocompromised children and adolescents. In this retrospective study, charts were reviewed for patients age 6 months to 17 years with acute leukemia and other hematologic malignancies who received combination therapy with caspofungin and either liposomal amphotericin B or voriconazole for at least 7 days for the treatment an invasive fungal infection. 85 In 17 of the 19 episodes of invasive mycoses, the patients had agranulocytosis (absolute neutrophil counts < 200/mm3) while in 2 other episodes the patients were severely neutropenic (absolute neutrophil counts < 500/mm3). Four of the episodes were considered proven, 12 probable, and 3 had possible invasive fungal infections, each of which was considered to be refractory to monotherapy with liposomal amphotericin B. Caspofungin was added to liposomal amphotericin B in 11 patients, while therapy was immediately changed to caspofungin plus voriconazole in 4 patients. Six of those treated with caspofungin and liposomal amphotericin B had a complete response and one died after 8 days of this combination. Four patients failed to respond to this regimen and were subsequently switched to caspofungin plus voriconazole. The combination of caspofungin and voriconazole was used to treat 12 invasive fungal infections in 10 patients. Complete resolution was reported in 5 of these infections, 4 had a partial response to therapy, and failure was observed in 3 episodes. In this study, each of the 5 patients in which severe neutropenia failed to resolve died. Overall, complete resolution was observed in 57.9% of the episodes of invasive fungal infections and a favorable response in 78.9%. When those with possible infections were excluded, the complete and favorable response rates were 62.5% and 68.4%, respectively.
Safety
In the clinical and pharmacokinetic studies discussed above, caspofungin monotherapy has been generally well tolerated with few significant clinical or laboratory adverse effects. Furthermore, few patients have had to discontinue therapy with this echinocandin due to drug toxicity. In the prospective, multi-center, open-label study of caspofungin as therapy against invasive candidiasis or aspergillosis in children and adolescents, thirteen of the 49 patients had at least one adverse event that was possibly related to caspofungin therapy. 64 However, none were considered serious and no patients discontinued therapy as a result. The most common drug-related laboratory adverse events were elevated liver transaminase levels, which occurred in 10 patients. These levels exceeded five times the upper limit of normal in only one patient and resolved once caspofungin therapy was discontinued. In the prospective, multi-center, double-blind study in patients with febrile neutropenia both caspofungin and liposomal amphotericin B were well tolerated. 65 Clinically significant adverse effects were reported in only 1 patient who received caspofungin and in 3 recipients of liposomal amphotericin B. The rates of hypokalemia (3.6% and 11.5% for caspofungin and liposomal amphotericin B, respectively) and nephrotoxicity (5.5% and 8.0%) were also similar between the treatment groups. The rates of infusion-related reactions were also similar between these agents, although these were generally considered to be mild in those who received caspofungin but severe in patients who received liposomal amphotericin B. Five patients randomized to caspofungin discontinued treatment due to a lack of efficacy or drug toxicity compared to 4 who received liposomal amphotericin B.
In addition to its excellent safety profile as monotherapy, caspofungin is also well tolerated when administered in combination with other antifungals. When caspofungin was combined with a lipid formulation of amphotericin B or to a regimen already consisting of a lipid amphotericin B formulation plus fluconazole or flucytosine in premature infants with persistent candidemia in the neonatal intensive care unit, severe thrombophlebitis was occurred in one patient and two experienced hypokalemia, which improved with potassium supplementation and continued therapy. 84 Four patients did experience a greater than 3-fold elevation in ALT and AST levels, three of which improved after the completion of therapy. Similarly, combination therapy with caspofungin plus liposomal amphotericin B or voriconazole was well tolerated in children and adolescents with acute leukemia or another hematologic malignancy. 85 Hypokalemia was the most frequently reported adverse events and occurred in 9 patients, 8 of which also received liposomal amphotericin B. Additionally increases in AST and ALT to more than 5 times the upper limit of normal were observed in four patients who received caspofungin in combination with voriconazole.
The safety profile of caspofungin in neonates, children, and adolescents was confirmed by a systematic review of 5 clinical registration studies, which included 171 pediatric patients, age 1 week to 17 years, who received at least one dose of caspofungin. 68 The overall incidence of drug-related clinical and laboratory adverse events were 26% and 16%, respectively, and were similar among the different pediatric age ranges. Fever, rash, and headache were the most common clinical adverse events, while increases in AST, ALT, and decreases in potassium were the most common drug-related laboratory events. The laboratory adverse events resolved either during subsequent caspofungin therapy or within 14 days of discontinuation, and none were considered serious or led to discontinuation of therapy. Two patients discontinued caspofungin therapy due to a drug-related adverse event. This included one patient with moderate hypotension, which resolved with the administration of a saline bolus, and the other who had a moderate rash that resolved within 10 days without treatment.
Conclusions
The role of caspofungin, and possibly the other echinocandins, in the treatment of invasive fungal infections, such as invasive candidiasis and invasive aspergillosis, will undoubtedly increase in infants, children, and adolescents. Overall, this agent is well tolerated both in the pediatric population as well as in adults. This is especially attractive in highly immuncompromised or critically ill patients where drug toxicities may adversely affect therapy. In addition, the lack of clinically significant drug interactions with caspofungin compared to other antifungals is also highly desirable in patients receiving poly-pharmacy. Although clinical data demonstrating efficacy are limited and no studies have been performed directly comparing treatment outcomes with other available antifungal agents, response rates in pediatric patients are similar to those reported from large clinical trials conducted in adults. However, because of the lack of comparative data and limited experience with caspofungin, at this time it is difficult to recommend caspofungin as first line therapy for the treatment of invasive fungal infection in neonates, children, and adolescents. Further studies are warranted to fully determine the place of caspofungin as therapy against invasive fungal infections in pediatric patients.
Author Contributions
Wrote the first draft of the manuscript: NPW. Contributed to the writing of the manuscript: NPW, LAH. Agree with manuscript results and conclusions: NPW, LAH. Jointly developed the structure and arguments for the paper: NPW, LAH. Made critical revisions and approved final version: NPW, LAH. All authors reviewed and approved of the final manuscript.
Competing Interests
NPW has received research support from Pfizer, Merck, Basilea, and Astellas, and has served on advisory boards to Merck and Viamet. LAH reports no disclosures.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.