
Abstract
Several non-stimulant medications have been used in the treatment of attention deficit hyperactivity disorder (ADHD). Atomoxetine, was introduced in 2002. The safety and efficacy of atomoxetine in the treatment of ADHD for children, adolescents, and adults has been evaluated in over 4000 patients in randomized controlled studies and double blinded studies as well as in recent large longitudinal studies. This paper provides an updated summary of the literature on atomoxetine, particularly in relation to findings on the short- and long-term safety of atomoxetine in children and adolescents arising from recent large longitudinal cohort studies. Information is presented about the efficacy, safety, and tolerability of this medication.
Introduction
Several non-stimulant medications have been used in the treatment of attention deficit hyperactivity disorder (ADHD). The non-stimulant atomoxetine was introduced in the United States in 2002. The safety and efficacy of atomoxetine in the treatment of ADHD for children, adolescents, and adults has been evaluated in over 4000 patients in randomized controlled studies and double blinded studies, as well as in recent large longitudinal studies.1–6
Though stimulant medications are frequently used as first-line agents, atomoxetine may also be considered as an initial choice, particularly in the presence of select comorbid disorders including active substance abuse, anxiety disorder, or tic disorder. 7
Atomoxetine mechanism of action
The mechanism of action of atomoxetine in the control and maintenance of ADHD symptoms is thought to be through the highly specific presynaptic inhibition of noradrenaline (NA), although the exact mechanism of action is not yet understood. Atomoxetine (Strattera®, Eli Lilly and Company) is a highly selective NA reuptake inhibitor, thereby increasing synaptic NA. It is the first nonstimulant medication approved by the United States Food and Drug Administration (FDA) for the treatment of attention deficit hyperactivity disorder (ADHD). It has a low affinity for serotonin or dopamine receptors, 8, 9 and the regions of the brain affected by atomoxetine are limited. It acts almost exclusively in the prefrontal cortical (PFC) regions, which play a key role in attention and higher cognitive processes but not in other dopamine rich brain regions such as the nucleus accumbens and striatum. 9 In addition, atomoxetine increases NA in other brain regions, with a substantial density of NA transporters, such as the brain stem areas and subcortical structures. 10 Genetic and imaging evidence point to dysregulation of NA as having a central role in the pathophysiology of ADHD. 11 Hence, atomoxetine may be used either as the sole pharmacological agent or in combination with stimulant medications, which act directly to enhance dopaminergic activity to treat ADHD.
Atomoxetine is efficiently absorbed after oral administration (range 63%-94%), and its bioavailability is minimally affected by food. After oral administration, atomoxetine reaches a maximum plasma concentration within two hours. Atomoxetine is highly bound to albumin and does not affect the binding of other common medications. 12
Atomoxetine metabolism
The metabolism of atomoxetine occurs primarily in the liver via the P450 (CYP2D6) system. The resulting conversion to 4-hydroxy-atomoxetine is glucuronidated and excreted in the urine. There are distinct differences within populations of CYP2D6 activity (extensive versus poor metabolizers). Genetic testing is available to detect the small percentage (<10%) of slow metabolizers who can have more than five times the blood level of medication and an extended half-life for a given dose. Atomoxetine has a plasma half-life of about five hours in extensive metabolizers. 13 Dosages of atomoxetine must also be reduced in patients with both renal and hepatic disease. 14 Response to atomoxetine should also be monitored more closely whenever a CYP450 2D6 inhibitor is added to or withdrawn from therapy, as dosage adjustment of atomoxetine may be necessary in extensive metabolizers. During co-administration, patients should be advised to contact their physician if they experience excessive adverse effects of atomoxetine such as dizziness, dry mouth, anorexia, sleep disturbances, and palpitations. Though atomoxetine does not induce or inhibit the cytochrome P450 (CYP2D6) system, it is involved in drug interactions that involve selective serotonin reuptake inhibitors (eg, fluoxetine and paroxetine) and other drugs (eg, quinidine) metabolized through this pathway, which may reduce atomoxetine clearance and cause higher peak plasma concentrations and slower elimination of atomoxetine. 12
Atomoxetine has a low affinity for various receptors, such as serotonergic, cholinergic, histaminic, alpha1-adrenergic, and alpha2-adrenergic and hence is not involved in drug interactions with these agents.
Atomoxetine interactions
Atomoxetine should not be used within two weeks after discontinuing MAOI (monoamine oxidase inhibitors) or other drugs that affect brain monoamine concentrations. Atomoxetine should be prescribed with caution if a patient is taking asthma medications (albuterol or other beta2 agonists) or other medications with chronotropic or pressor effects. In combination with either citalopram, 15 venlafaxine, or stimulants, involuntary movements have occurred. 16 These symptoms are likely to resolve after the discontinuation of atomoxetine.
The efficacy of atomoxetine, in addition to its safety and tolerability, in the treatment of ADHD are discussed in the Results section of this article. This review provides an updated summary of the literature on atomoxetine to that provided by Hammerness et al, 17 particularly in relation to findings on the short- and long-term safety of atomoxetine in children and adolescents arising from recent large longitudinal cohort studies.
While qualitative reviews of the literature, such as the information below, are useful for summarizing results and drawing conclusions about general trends, it remains important to appreciate that such reviews cannot easily evaluate the many factors associated with study design and measurement that may influence the apparent medication effect from the results of a single study.
Methods
Literature search
In accordance with our aim to extend the review of Hammerness et al, 17 we have included a literature search of studies since 2009 that report on the efficacy, safety, and tolerability of atomoxetine.
The literature search was undertaken on 14 June 2012. The other dates refer to the dates covered within the search using the different search engines and are the actual names of the search engines (e.g, “psychINFO (from 2002 through the first week of June 2012)” was the title of the search engine used), therefore, the different years listed (i.e, 2002 vs. 2009). Search terms were “ADHD” and “atomoxetine.” Both words were entered separately, before search results for both words were combined with a limit for publication year set as 2009–current. An initial screen was undertaken on all search results where publication titles and abstracts were examined and publications filtered if they did not appear to meet eligibility criteria at the outset. Those which were not filtered out at the screening phase (including ones we were unsure of from the title and abstract) were subsequently assessed for eligibility by examination of the full-text article. Requests to the University of Sydney library or the corresponding author were made to obtain full-text for the articles which were not accessible online.
Journal papers were included in the review if they met the following criteria: clinical study utilizing atomoxetine as a treatment, human child or adolescent participants (<18 years of age) with a primary diagnosis of ADHD determined by a clinician or based on Diagnostic and Statistical Manual of Mental Disorders IV (DSM-IV), outcomes of either effect of atomoxetine on ADHD symptom measures and/or safety, and written in the English language. Excluded were monographs, reviews, meta-analyses and pooled analyses papers, books, case reports, articles not published by peer-reviewed scientific journals, papers available only in a language other than English, adult studies, trials without any adverse events reporting or efficacy outcomes in relation to ADHD symptom severity after atomoxetine treatment, animal studies, and papers reporting already-published data (in these cases, only one of the papers per study were included).
Outcomes of interest
The change in scores before and after treatment (mean and standard deviation [SD]) reflecting the efficacy of atomoxetine on behavioral and cognitive performance measures specifically were extracted from the literature. The numbers of participants who withdrew from a study because of a lack of efficacy of atomoxetine were also recorded. Where mean change data were not published, it was calculated using the published pre- and post-treatment values. The efficacy of atomoxetine in the treatment of ADHD was assessed through review of the effects of length of treatment, dosing, impact of age or prior stimulant use, and comorbid conditions. Information about the safety of atomoxetine, tolerability, and adverse events (type and frequency) were recorded and were compared with reports from earlier studies.
Results
The literature search for papers from 2009 yielded 183 results in total. After excluding papers that did not meet eligibility criteria as well as duplicates (eleven papers were duplicated), 33 papers met the criteria for the review of papers from 2009 (Fig. 1). Information from these papers and previously published data is summarized in regard to findings on mechanism of action, metabolism, efficacy, tolerability, and safety.
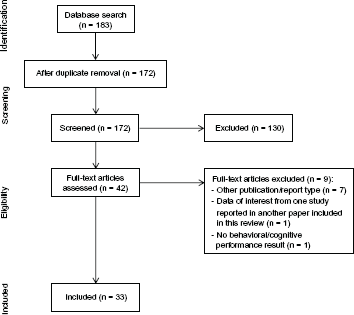
Literature flow chart.
Efficacy
The papers included in this review since 2009 observed the efficacy of atomoxetine on a wide spectrum of measures including reported ADHD symptoms, quality of life, other internalizing and externalizing symptoms, functioning and life participation, clinical global impressions, cognitive performance measures, family impact and functioning, perceived difficulties, school performance and academic functioning, and health outcomes (eg, risky behaviors and sleep habits) (Table 2). These measures included direct performance measures as well as perceived ratings by the child, parent, teacher, investigator, or clinician (Table 2). The findings of these papers are briefly summarized below, and further detail is provided in Tables 1 and 2.
Participant characteristics.

Efficacy table.

Dose refers to mean endpoint dose unless otherwise specified.
Short-term treatment
For the purpose of this review, we have included papers that incorporated short-term post-treatment assessments at less than or equal to eight weeks. Twenty-one of the papers located from the literature search reported results within this time frame (Table 2). Within these short-term reports, improvements after atomoxetine treatment were observed from as early as two weeks, where Dittman et al, for example, reported an improvement in perceived difficulties and parent-rated ADHD symptoms. 18 This was the only study located using our search criteria which reported measures taken at a time point as early as two weeks.
Overall, the recent literature suggests that within eight weeks of treatment, atomoxetine was beneficial in significantly improving child-, parent-, clinician-, and teacher-rated ADHD symptoms, internalizing and externalizing behavior ratings, perceived difficulties, functioning and life participation, academic/school functioning, youth risk behavior, classroom behavior, depressive symptoms, sleep habits, and quality of life (Table 2). More objective performance measures of attention (continuous and switching) and executive abilities (the ability to organize, plan and anticipate) were also significantly improved after treatment with atomoxetine within this time period (Table 2). In those studies that incorporated a placebo arm, the improvements observed after treatment with atomoxetine were often superior to placebo across these measures (Table 2).
Within these studies, atomoxetine was either used as a sole treatment (at times comparing different doses or daily dose frequencies), or combined with behavioral therapy, psychotherapy in addition to behavior management, methylphenidate, mood stabilizers, or antipsychotic medications. These atomoxetine treatment arms were compared with treatment arms utilizing methylphenidate, ABT-089, and/or placebo or compared participants with ADHD to “healthy” controls or with participants with ADHD in addition to comorbid reading disorder, comorbid dyslexia. Other participant groups included within two of these studies had reading disorder alone and ADHD with comorbid bipolar disorder (Table 1). Six of the studies included did not have any comparison treatments or groups. Significant benefits were observed after treatment whether atomoxetine was used alone as a sole treatment or in combination with another medication or treatment modality. When combined with behavior therapy such as in Waxmonsky et al's studies,19,20 greater benefits were reported in some (but not all) parent- and/or teacher-ratings on sub scales pertaining to disruptive behaviors, social skills, academic performance, and impairment and depression ratings (Table 2). Methylphenidate in combination with atomoxetine may also provide superior benefits to symptom and behavior ratings beyond what atomoxetine alone provides, as further improvements to outcome measures were observed in a three-week atomoxetine plus methylphenidate phase following four weeks of atomoxetine alone.21,22 When comparing atomoxetine alone with methylphenidate, the effects from both treatments were comparable in that both treatments significantly improved behavior and cognitive measures.23,24 Atomoxetine was superior to ABT-089 across symptom, behavior, and quality of life measures (Table 2). 25
In cohorts with comorbid conditions, short-term benefits of atomoxetine treatment were consistently reported in ADHD symptom levels with no significant differences between groups, including groups with comorbid bipolar disorder, reading disorder, oppositional defiant disorder (ODD), or between inattentive and hyperactive-impulsive ADHD subtypes (Table 2). Further, de Jong et al also found a positive effect of atomoxetine compared with placebo on cognitive performance tasks including measures of visuospatial working memory and inhibition in their cohorts with ADHD, ADHD plus reading disorder, and in reading disorder alone. 26 Atomoxetine, however, had no significant effect on depression or mania ratings in those with comorbid bipolar disorder (although there were no comparison treatments or groups). 27
Within these short-term studies, atomoxetine doses ranged from 0.2 to 1.8 mg/kg/d (Table 2). Investigations into atomoxetine dosing examined the effect of different dosing concentrations (two studies), fast versus slow titration (one study), or one versus two doses per day (one study). Cho et al 28 and Takahashi et al 29 examined atomoxetine doses of 0.2, 0.5, 1.2, and 1.8 mg/kg/d in 6 to 18 year olds, and their results suggest that the lower doses (0.2 and 0.5 mg/kg/d) were ineffective for improving ADHD symptom ratings, while significant benefits were observed with the higher doses (1.2 and 1.8 mg/kg/d). No differences were observed when participants adopted either a slow or fast titration schedule, and significant improvements to ADHD symptoms, life participation, family functioning, academic achievement, and some risky behavior ratings were observed after both titration schedules (Table 2).30,31 In relation to one versus two daily doses, Waxmonsky et al found that one daily dose was superior to two daily doses in behavior and impairment ratings, where after eight weeks of treatment, significant benefits were observed in some of the measures only in those who took one daily dose (Table 2).19,20 Additionally, Waxmonsky et al assessed participants every fortnight and found that improvements in parent-rated behaviors improved from the commencement of treatment (within the first fortnight) when one dose per day was taken, while benefits with two daily doses were first noticed halfway through the eight-week treatment period.
In summary, improvements in ADHD symptoms, behavior, functioning, quality of life, and cognitive performance measures are seen within the first 2 to 8 weeks of treatment with atomoxetine in children and adolescents with ADHD alone and in those with ADHD and comorbid disorders. Atomoxetine is also effective whether it is used alone or in combination with methylphenidate or other treatment modalities, and there is currently limited evidence that atomoxetine is more effective at higher doses and when taken as a single daily dose.
Long-term treatment
Long-term studies summarized in this section include those reporting results taken after treatment of more than eight weeks in duration. The two longest studies ran for either 10 months 32 or for eight weeks with an additional 40 week maintenance period.30,31 Seventeen studies reported results from longer-term time points.
Overall, the results from the longer-term studies were consistent with the findings from the short-term studies, whereby atomoxetine improved many of the outcome measures even up to 10 months post-treatment (Table 2). Similar to the short-term reports, the longer-term studies compared atomoxetine to other treatments (stimulants 32 and methylphenidate23,24) and to placebo arms and combined atomoxetine treatment with other treatment modalities (motivational interviewing plus cognitive behavior therapy 33 and psychoeducation for parents 34 ). Atomoxetine dosing was examined also in relation to fast versus slow titration35,36 and compared low doses (0.8 mg/kg/d) to higher doses (1.4 mg/kg/d).30,31 Cohorts used for comparisons included healthy controls and participants with ADHD with comorbid dyslexia (Table 2).
Three studies compared the efficacy of atomoxetine to methylphenidate or stimulant medication.23,24,32 Bastiaens et al reported similar benefits in ADHD symptom ratings, quality of life, internalizing and externalizing symptoms, and functioning for both treatments (atomoxetine and stimulants) with no differences between treatments (Table 2). 32 However, the results from Yang et al 23 and Yildiz et al 24 suggest that although there are similar benefits with atomoxetine and methylphenidate, the magnitude and consistency of improvement from methylphenidate may be marginally superior to atomoxetine (Table 2). Across both studies, methylphenidate demonstrated improvements in a larger number of measures than atomoxetine and also yielded improvements that were significantly greater than those from atomoxetine (on the Tower of Hanoi test) and greater than changes observed in control participants (on the Trail-making test, Table 2). It should be noted, however, that there were differences between the cohorts enrolled in the Bastiaens et al study compared with those in the studies by Yang et al and Yildiz et al: the cohort in Bastiaens et al's study included those with comorbid internalizing disorders, whereas the participants from the latter two studies only had externalizing disorders (conduct disorder and ODD) (Table 1). This may in part explain the differences observed in response to atomoxetine and methylphenidate/stimulant medication.
Atomoxetine was also compared with placebo, where both treatment arms were combined with four sessions of psychoeducation for parents 34 or motivational interviewing plus cognitive behavior therapy. 33 Atomoxetine was superior to placebo when both groups also received four sessions of psychoeducation for parents in improving ADHD symptom and improvement ratings, 34 while there was no difference between the improvements seen in ADHD symptom ratings after atomoxetine and placebo when participants also received motivational interviewing plus cognitive behavior therapy. 33 In Thurstone et al's older cohort, the group receiving atomoxetine had a significant reduction in non-tobacco substance use over the prior 28 days, but the change was not significantly different to the placebo group. 33 No other changes were observed (Table 2).
There were no significant differences in improvements seen when participants were administered a fast versus slow titration schedule, and improvements were seen with both titration schedules in ADHD Symptom ratings and some quality of life measures (Table 2).35,37 Interestingly, physical well-being scores worsened significantly more after atomoxetine treatment than placebo, while most other quality of life measures improved after atomoxetine treatment compared with placebo.
Only one trial was undertaken (reported in two papers) comparing a low dose to a high dose after a 40-week maintenance period.30,31 As mentioned in the short-term treatment section above, atomoxetine was very effective in improving outcome measures during the initial eight-week acute treatment phase and was effective at both 0.8 and 1.4 mg/kg/d doses in maintaining improvements (compared with baseline) in parent-rated life participation scores. However, life participation scores were significantly poorer after the 40-week maintenance phase in comparison with scores achieved after the previous eight-week acute treatment phase in the low-dose (0.8 mg/kg/d) group, suggesting that a higher dose is required to maintain these benefits. The same was observed in ADHD symptom ratings, whereby the lower dose was unable to sustain improvements in total, inattentive, and hyperactive-impulsive symptom scores after the 40-week maintenance phase. The higher dose (1.4 mg/kg/d) was also unable to sustain the improvement in symptom ratings only in the inattentive symptoms score. In a subgroup of participants classified as having high risk-taking behavior, improvements to academic functioning and risky behaviors were maintained at 40-weeks (Table 2).
Within the long-term studies included in this review, one approximately 16-week long study looked at the effects of atomoxetine on ADHD compared with ADHD with a specific comorbidity. Specifically, Sumner et al studied ADHD compared with ADHD with dyslexia and found that atomoxetine improved ADHD symptom ratings, life participation scores, and educational achievement in both ADHD groups with no differences between those with ADHD alone compared with those with comorbid dyslexia. 38 A working memory test battery for children was also used in this study, where those with comorbid dyslexia showed an improvement in phonological loop standard score (from tests including digit recall, word list matching, word list recall, and non-word list recall), while those with ADHD alone had significant improvements (which were also significantly greater than in those with dyslexia) in central executive measures from tests including backward digit recall, listening recall, and counting recall (Table 2).
There is clearly still a paucity of long-term atomoxetine literature available, particularly in regards to the effects of different dosing schedules and comorbidities, so it is difficult to draw conclusions from what is currently available. However, these latest papers indicate that atomoxetine may be effective at higher doses in longer-term control of symptoms, functioning, symptoms, and behavior. Regular follow-ups of patients to continuously reassess symptom levels is currently indicated to maximize the likelihood that initial benefits from treatment are maintained.
Tolerability and safety
General tolerability
Atomoxetine is generally well tolerated in healthy children and adolescents, with typically only mild adverse effects, which seldom lead to discontinuation of medication. 4 Adverse events include headache, abdominal pain, nausea, decreased appetite, weight loss, vomiting, and somnolence. There is a very low incidence of serious adverse events. A full list of the nature and frequency of side effects in treatment with atomoxetine (and comparator) groups is provided in Table 3. The importance of methodology to permit determination of risk of adverse events and tolerability is emphasized in the outcomes of these papers and is included in the discussion below.
Safety.
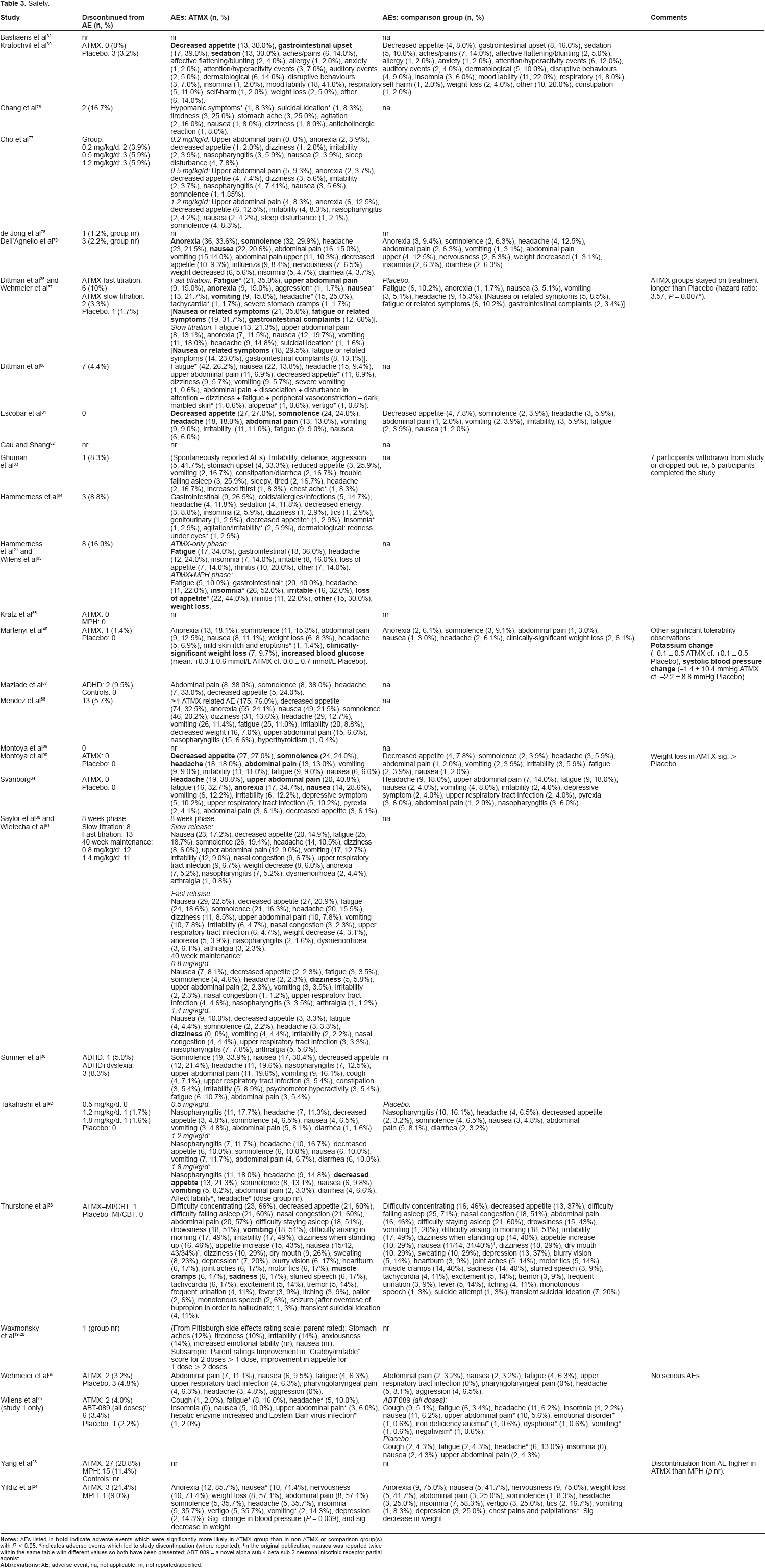
Kratochvil et al1,39 reported that atomoxetine was well tolerated by both younger and older children with ADHD. Rates of adverse events were similar in both age groups, although the types of adverse events experienced differed between the groups. Atomoxetine treatment in the 6- to 7-year-olds resulted in higher rates of upper abdominal pain, decreased appetite, vomiting, and somnolence compared with placebo, while 8- to 12-year-olds experienced higher rates of decreased appetite, somnolence, irritability, and fatigue. Statistically significant increases in pulse and decreases in weight for both younger and older children on atomoxetine treatment were noted compared with placebo in the 2008 study only. 1 Increases in systolic and diastolic blood pressures in the older children and decreased weight in the younger children, although statistically significant, were not judged as clinically significant. Of the 33 studies since 2009, 11 reported side effects in a comparator group, 8 of which included a placebo group (Table 3). While the nature and frequency of side effects were comparable with earlier studies and greater than in the placebo groups, participants did not discontinue treatment more often in the treatment groups compared with participants receiving placebo (Table 3).
Several recent papers reported on the impact of dosage on side effects. These titration studies reported on side effects with dosing between 0.2 and 1.8 mg/kg.28,29,31,37 The occurrence of gastrointestinal side effects were equivalent to placebo at doses of 0.5 mg/kg or less. Where weight loss was reported, there were no statistically significant differences between the atomoxetine-treated group compared with the placebo group in a double-blind study of 93 participants by Kratchovil et al. 39 In another double-blind study of 105 participants, Martenyi et al 40 reported a statistically significant higher rate of weight loss in the atomoxetine treated group compared with the placebo group (9.7% versus 6.1%).
Some subpopulations may vary in tolerability of atomoxetine. Tolerability of atomoxetine may be reduced in children and adolescents with an autistic spectrum disorder. In the study by Troost et al, 41 5 participants (42%) discontinued because of side effects including gastrointestinal symptoms, irritability, sleep problems, and fatigue, though this was a young population. 42 Tolerability was greater and side effects were fewer in a recent cohort of 24 participants reported by Fernandez-Jaen et al. Adverse side effects occurred in 5 participants (21%), 2 of whom discontinued medication as a result. 42
Rarely, atomoxetine may be associated with serious liver injury. 43 Reports of liver injury related to atomoxetine were reviewed by Bang et al in 2008 and are discussed further in regard to safety below. 44 No new or unexpected safety concerns have been reported over longer-term treatment. 45
The frequency of adverse events with atomoxetine treatment is impacted by the method of drug initiation. Participants rapidly titrating to a full treatment dose within the first week of treatment and those receiving daily rather than twice-daily dosing are more likely to experience side effects. Optimal ways to initiate therapy with atomoxetine were studied by Grennhill et al. 46 Some children may tolerate a divided dose well during initiation of treatment and are then able to switch over to a once-daily dosing schedule for maintenance. Side effects were also more commonly noted in association with faster titration schedules in studies from 2009.30,35
Growth
It has been postulated that growth delay may be intrinsic in the ADHD condition rather than being drug-induced, 47 and studies have not found evidence that unmedicated children and adolescents with ADHD are smaller than expected.48,49 While weight loss of about 1 kg over a period of 2 to 3 months is reported to occur in 5% to 10% of patients treated with atomoxetine, recent studies of greater than 12 weeks duration have not included measurements of growth.
Several earlier open-label studies of atomoxetine administered for 2 years or longer have been conducted, and two meta-analyses have recently reported on growth outcomes.
Kratochvil et al 50 included data from 13 studies of 6- to 7-year-old children who were treated with atomoxetine up to a mean dose of 1.47 mg/kg/d. At the end at the 24-month treatment, weight was on average 2.5 kg less and height on average 2.7 cm less than expected based on baseline percentile. In another meta-analysis, Spencer et al 51 pooled data from both children and adolescents aged 6 to 16 years. After 24 months of treatment, there was a decrease of 2.7 percentile points for weight (corresponding to a mean 0.87 kg less than expected) and a decrease of 2.2 percentile points for height (0.44 cm less than expected). These differences between observed and estimated growth in both these studies were statistically significant. The slowing in growth velocity was most evident after 18 months of treatment and tended to attenuate afterwards.
The clinical significance of this effect has been considered negligible at the group mean level but may be important at the individual patient level with extended treatment beyond two years. The mechanism of the effect is speculated to be through a decrease in caloric intake. Caloric supplementation has been suggested as a possible remedy, but its efficacy has not been tested. Because the therapeutic effect of atomoxetine requires continuous dosing, drug holidays are not an option during the academic year, but may be considered for selected patients during non-academic periods.
In a 5-year safety of treatment study, Spencer et al 52 reported on the impact of atomoxetine on growth in a large sample of children and adolescent participants. Maximum decrement of weight loss was observed at 15 months (–9.9%, P < 0.001); however, by the 5-year time point, participants had slightly overshot their starting weight percentile.
Similarly, maximum decrement from expected height was observed at 18 months (–6.6 percentage points, P < 0.001). At present, continuous atomoxetine treatment does not appear to have a significant effect on juvenile growth and final stature for most patients.
Suicidality
McCarthy et al 53 used the United Kingdom General Practice Research Database to assess 5351 patients aged 2 to 21 years from January 1, 1993, to June 30, 2006, who had taken medication to treat ADHD. In over 18,000 patient years, there were seven acute deaths, three of which were attributed to suicide. No deaths occurred among those taking atomoxetine, though an increased standard mortality rate was reported for those taking medication for ADHD.
Several authors have published case reports describing acute suicidality and aggression commencing shortly after initiating treatment with atomoxetine, and, in 2008, a boxed warning was placed into the package insert for atomoxetine. These symptoms have been managed successfully by ceasing atomoxetine or adding a further medication.54,55 The FDA recommends that prior to prescribing atomoxetine to a patient, clinicians should consider psychiatric comorbidities, obtain personal and family histories of mood disorders and suicidality, and monitor for any negative changes in mood after the commencement of atomoxetine treatment. 17 In a group of 70 participants with ADHD and comorbid substance use, Thurlstone et al 33 noted lower rates of suicidal ideation (11%) in the group randomized to receive atomoxetine compared with the group receiving placebo (20%), further illustrating the importance of randomization and adequate comparator groups in evaluating tolerability and side effects from medication in clinical outcome studies.
Psychosis
Psychotic adverse events have been reported in association with stimulant medications and atomoxetine. The FDA review of ADHD drug randomized controlled trials reported the highest psychosis adverse event rate (13.2/100 person-years) with methylphenidate (in the form of transdermal patches) followed by dexamphetamine (2.0/100 person-years) and atomoxetine (0.8/100 person-years). As per the current FDA medication guide, clinicians should inquire about personal or family histories of mood disorders and psychosis prior to initiation of atomoxetine. 56
Hepatic injury
By 2005, there had been 7962 pediatric and adult case reports of hepatic injury associated with atomoxetine, of which 41 were identified as requiring further analysis. 43 Most of these events were mild increases in hepatic transaminase levels. During the 4 years after the market launch of atomoxetine, 351 cases of liver injury reported in relation to the drug treatment for ADHD. Of those 351 cases, 69 had explanations unrelated to the use of the drug, 146 presented insufficient information to assess the cause, 133 contained confounding factors and were labelled as possibly related to drug use, and the remaining 3 cases reported liver injury probably related to atomoxetine use. 43 The etiology of drug-induced liver injury with atomoxetine is uncertain. There have been no cases of liver failure. Cases of liver injury have resolved following cessation of medication. 57
Withdrawal from lack of efficacy.

Given the rare nature of these reports, it is not currently recommended for clinicians to do routine monitoring of liver function during treatment.
Cardiovascular effects
Concern about the cardiovascular safety of atomoxetine falls into two main areas: concern about acute dynamic effects of this medication on heart rate and blood pressure and concern that these changes may confer increased risk of major cardiac or neurovascular events.
It is well documented that atomoxetine may increase heart rate in both younger and older children. A statistically significant treatment-group difference in systolic blood pressure and diastolic blood pressure has been observed for older children but not for younger children. 1
A small minority of children and adolescents taking atomoxetine (2.5% in pediatric placebo controlled trials) have been identified, with larger heart rate increases of 25 beats per minute (bpm), whereby 1.1% have increases in heart rate of this magnitude on more than one occasion. 43 These observations underpin the recommendation for pulse and blood pressure to be measured at baseline and periodically while on therapy to enable children and adolescents at heightened risk to be identified.
In a large cohort of over 440,000 adults aged 25 to 64 years, including over 150,000 users of ADHD medications, evidence was not found of an increased risk of heart attack or stroke associated with current ADHD medication use. 58 Similarly, this study did not find evidence to support an increased risk of cardiovascular complications for current use of any of the specific medications examined (ie, methylphenidate, amphetamines, or atomoxetine) or for an increase in risk with increasing duration of current use of ADHD medications. Furthermore, results were similar when restricted to new users or to those with or without ADHD. Results also were similar when the cohort was restricted to those with or without evidence of prior cardiovascular disease or to those with or without evidence of prior non-ADHD psychiatric conditions. Authors of this large longitudinal study recognized several limitations. 58 Use of ADHD medications was based on electronic records of filled prescriptions. Use of ADHD documented on these records may not fully correspond with actual medication taken; however, electronic pharmacy databases have been found to be excellent unbiased sources of information on drug use, and it seems unlikely that any misclassification of use would be differential with respect to the endpoints of interest. While diagnosis of myocardial infarct is also reliably recorded and occurred at an expected rate in the non-treated population, the recording of other vascular events is less well validated. 59
The findings of no increased risk of serious coronary heart disease in young or middle-aged adults associated with use of ADHD medications are consistent with some but not all previous reports. 60 A cohort study conducted among adults over 18 years of age compared risk of cerebrovascular accidents (CVA) and transient ischemic attacks (TIA) among those prescribed atomoxetine and those prescribed stimulant ADHD medications with risk or CVA and TIA among adults in the general population. 61 Higher rates of CVA and lower rates of TIA were observed in current users of atomoxetine compared with users of stimulants, although the number of events was small and risk ratios were not statistically significant. Compared with rates in the general population, users of ADHD medications had higher rates of TIAs and lower rates of CVA, although the latter was not statistically significant.
Non-clinical cohort studies have examined the cardiovascular effects of atomoxetine in conjunction with examining the effects of other medications used to treat ADHD. Gould et al used a case-control design to examine the association between ADHD medications and risk of sudden death in children and youths aged 7 to 19 years of age. 62 This study found an elevated odds ratio of 7.4 (95% CI 1.4–74.9) of sudden death associated with use of medication (stimulants or atomoxetine) to treat ADHD. In contrast, no increase in sudden cardiac deaths among children, adolescents, and young adults using ADHD medications (methylphenidate, dexamphetamines, or atomoxetine) was observed in a cohort study conducted in the General Practice Research Database in the United Kingdom by McCarthy et al. 53
Findings from the report by Habel et al 58 are reassuring with respect to the cardiac safety of relatively short-term use of ADHD medication use in young and middle-aged adults. As stated in an earlier review by Perrin et al, current evidence does not suggest that treatment with therapeutic doses of ADHD pharmacotherapies in healthy children causes serious cardiovascular effects or sudden death. 63 However, sudden death has been reported in association with atomoxetine treatment at usual doses in children and adolescents with structural cardiac abnormalities or other serious heart problems. Although some serious heart problems alone carry an increased risk of sudden death, the National Institute for Health and Clinical Excellence NICE guidelines recommend that atomoxetine generally should not be used in children or adolescents with known serious structural cardiac abnormalities, cardiomyopathy, and serious heart rhythm. 64
Children who are being considered for treatment with atomoxetine should have a careful clinical history (including assessment for a family history of early sudden death) and physical exam to assess whether cardiac disease is present as well as to inquire about possible cardiac symptoms including chest pain and syncope. Electrocardiogram is not a mandatory component of cardiovascular assessment and monitoring before or during ADHD treatment with atomoxetine.63,65
Neurological effects
ADHD patients have been shown to have incidence rates of unprovoked seizures and epilepsy as many as two to three times greater than non-ADHD children. 66
The incidence of seizures has not been found to differ between subjects on atomoxetine and placebo for current versus non-use (relative risk 1.1). 67 The rate of seizures as an adverse event with atomoxetine use has been estimated at between 0.1% and 0.2%. In post-market reports of seizure, the rate of seizures among children and adolescents prescribed atomoxetine was within the normal population occurrences. 68
Overdose
Based upon poison centre reports,69,71 adverse drug reactions do not correlate with atomoxetine dose, 69 though serious outcomes have been more commonly found with greater maximum dose. No major outcomes or fatalities have been reported.
Gastrointestinal symptoms and lethargy are typically reported with overdose of atomoxetine.69,71 Seizures were reported in two patients, including one adolescent female who ingested 2840 mg of atomoxetine in a suicide attempt. 72
While subacute effects of atomoxetine seem negligible under therapeutically relevant concentrations, abnormalities in cardiac conduction should be considered in cases of atomoxetine overdose and when administering atomoxetine to patients at increased risk for long QT syndrome. 73 Sinus tachycardia and increased blood pressure have also been noted.69,71
Adverse effects of overdose with atomoxetine also include mood symptoms and agitation. 69 In one study, 17% of patients had acute agitation when treated with benzodiazepines. 71
Sleep
In a randomized, double-blind, cross-over study comparing the effect of methylphenidate (given thrice daily) and atomoxetine (given twice daily) on the sleep of children with ADHD, methylphenidate increased sleep-onset latency significantly more than atomoxetine. 74 Moreover, both children's diaries and parent reports indicated a better quality of sleep (in terms of “getting ready in the morning,” “getting ready for bed,” and “falling asleep”) with atomoxetine compared with methylphenidate. Both medications decreased nighttime awakenings, but the decrease was greater for methylphenidate. Clearly, these results from a single study need to be replicated.
In studies from 2009, insomnia and disturbances in sleep were reported to occur with frequencies ranging between 10% and 60%. Importantly, the occurrence of disturbances in sleep were not significantly different in studies in which there was a placebo group.33,39,75
Summary
Atomoxetine is a highly selective noradrenaline reuptake inhibitor. It is both clinically effective and cost effective in the treatment of children and adolescents with ADHD.
Treatment doses of less than 0.5 mg/kg/day are unlikely to be effective. Higher doses of 1.8 mg/kg/day may also enable greater ADHD symptom control as well as management of comorbid externalizing disorders, though may result in increased side effects. Twice-daily dosing assists in ameliorating these effects and is a useful strategy when prescribing atomoxetine at doses greater than 1.2 mg/kg/day.
Atomoxetine decreases comorbid anxiety at usual treatment doses for ADHD.
Approximately 10% of patients are poor metabolizers of atomoxetine (CPY2D6) and will have blood levels four to five times that of patients who are efficient metabolizers for a given dose. The dose of atomoxetine also needs to be decreased in those with liver or renal disease and when prescribed with other medications impairing metabolism in the cytochrome P450 system. Atomoxetine should be withheld for at least two weeks after discontinuing MAOIs.
Atomoxetine is well tolerated. Gastrointestinal symptoms and lethargy are the main reason for discontinuation of atomoxetine, which is recorded at around 5% in many studies. Atomoxetine does not adversely affect seizure threshold orties. Around 1% of patients prescribed atomoxetine have been noted to have large increases in resting heart rate (>25 bpm) on more than one occasion. Statistically significant but not clinically significant increases in blood pressure are observed only in older patients taking atomoxetine.
The safety profile of atomoxetine is also well established, both in terms of clinical prescription and overdosage. Overdose effects include lethargy, liver injury, and cardiac conduction changes. As indicated by the black box warning, atomoxetine is associated with increased suicidal ideation, though it has not been associated with death from suicide. The etiology of drug-induced liver injury with atomoxetine is uncertain. There have been no cases of liver failure with atomoxetine. Seizures have been reported twice. All medication-related effects attributed to atomoxetine have resolved either with cessation of medication or addition of a further medication.
The medication guide for atomoxetine can be found at http://www.fda.gov/cder/Ofnces/MG/AtomoxetineMG/pdf
Author Contributions
Conceived and designed the experiments: MRK. Analysed the data: MRK, TWT. Wrote the first draft of the manuscript: MRK. Contributed to the writing of the manuscript: MRK, TWT, SDC. Agree with manuscript results and conclusions: MRK, TWT, SDC. Jointly developed the structure and arguments for the paper: MRK, TWT. Made critical revisions and approved final version: MRK, TWT, SDC. All authors reviewed and approved of the final manuscript.
Funding
MRK is a member of Ad Board for Eli Lilly and Shire. MRK and SDC received honoraria from Janssen Cilag, Eli Lilly and Shire, for presentations and development of educational materials. TWT has no financial disclosures or conflicts of interest to disclose.
Competing Interests
MRK's institution has received grants from NHMRC, and he has received payment for lectures from Janssen-Cilag and Eli-Lilly. SDC has received payment for lectures from Janssen-Cilag and Eli-Lilly Other authors disclose no competing interests.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.
Footnotes
Acknowledgements
The authors would like to acknowledge Prof. Leanne M. Williams, who was an investigator on the ACTION study evaluating atomoxetine at the Brain Dynamics Centre, Westmead Millennium Institute for Medical Research and University of Sydney Medical School––Westmead, Westmead, NSW, Australia. TWT was supported by a Research Fellowship from the Westmead Millennium Research Foundation.