
Abstract
Purpose
To validate serum neutrophil gelatinase-associated lipocalin (NGAL) as an early biomarker for acute kidney injury (AKI) in sepsis-related conditions and its predictive and prognostic values.
Patients and Methods
This study included 65 patients, who were clinically evaluated for sepsis, severe sepsis, or septic shock, and 20 apparently healthy served as controls. Patients were divided into two groups: Group I (AKI-sepsis): 65 newly admitted patients diagnosed as sepsis, who were further divided into three subgroups according to the severity: systemic inflammatory response syndrome, severe sepsis, and septic shock, and Group II (control group): 20 apparently healthy subjects matched for age and sex, serum creatinine and serum NGAL concentrations were estimated initially within 24 hours of admission and after 72 hours of admission in all patients and control groups.
Results
Serum NGAL increased significantly with increasing severity of renal impairment. Receiver-operating characteristic analysis suggested that serum NGAL cutoff value of 40 ng/mL within the first 24 hours of admission is highly specific and sensitive for predicting AKI, with sensitivity of 90.9% and specificity of 75.8%.
Conclusion
We concluded that early measurement of serum NGAL level in sepsis can serve as a clinically useful marker for early prediction of AKI and for grading of its severity.
Introduction
Acute kidney injury (AKI) in pediatrics is a complex disorder with clinical manifestations ranging from mild dysfunction to complete anuric kidney failure. 1 The exact incidence of pediatric AKI is unknown, but it is likely higher than the reported, as infants very commonly have nonoliguric renal failure. AKI is a common sequel of sepsis. It was suggested that sepsis-induced AKI may have a distinct pathophysiology and identity. 2 Few clinical studies of biomarkers in AKI in septic patients suggest promising evidence that these biomarkers may aid in early detection of AKI in sepsis and may have value for predicting subsequent deterioration in kidney function. Delay in the diagnosis of AKI using conventional biomarkers like urine output and serum creatinine has been one of the important obstacles in applying effective early interventions. 2
Several biomarkers have been evaluated for early diagnosis of AKI, among which neutrophil gelatinase-associated lipocalin (NGAL) appears to be most promising. 3
NGAL, a protein synthesized by renal tubular cells, has the property to transport lipophilic molecules such as vitamins, hormones, and antigenic agents. It is a novel biomarker for acute kidney dysfunction of several etiologies and is increased in both serum and urine 48 hours before the increase of creatinine. It has a strong correlation with early diagnosis of AKI. 2
Meanwhile, the desirable biomarker needed for detection of AKI should be noninvasive, sensitive, and specific, increases proportionate to degree of damage, can predict clinical outcomes and efficacy of therapy, and its results should be available even when the damage is limitable. 1
Patients and Methods
This study included 65 patients who were clinically evaluated for sepsis, severe sepsis, or septic shock, and their ages ranged from 2 to 48 months. Twenty apparently healthy children served as controls. Patients were selected from the emergency unit of Pediatric Department, Minia University Hospital, in the period between November 2011 and August 2012 after the approval of ethics committee review board of the Faculty of Medicine, Minia University. This research was conducted in accordance with the principles of the Declaration of Helsinki.
Patients (Group I) were subdivided into three subgroups according to the severity of sepsis as defined by the International Pediatric Sepsis Consensus Conference 4 : Group la (systemic inflammatory response syndrome [SIRS]): 23 patients aged 2–36 months (13 males and 10 females), Group Ib (severe sepsis): 20 patients aged 2–48 months (9 males and 11 females), and Group Ic (septic shock): 22 patients aged 2–36 months (10 males and 12 females).
AKI was defined using the creatinine criteria of the pediatric risk–injury–failure–loss–end-stage renal disease (pRIFLE) staging system. 2
Group II (control group) included 20 apparently healthy subjects matched for age and sex. Informed consents were obtained from the parents of all the subjects.
Venous blood samples were taken at the time of admission for assessment of serum NGAL levels and initial serum creatinine concentrations. Patients were subsequently discriminated, within 72 hours of admission, according to the pRIFLE criteria, into acute kidney affection (n = 30; 16 in stage R, 4 in stage I, and 10 in stage F) and nonacute kidney affection (n = 35) subgroups. Creatinine criteria were met by all the patients with acute kidney affection, while urine output criteria were met by only 12 of them. Patients with any factor that may affect renal parameters prior to admission, including renal disease, congenital deformities of the kidney whether anatomical or vascular, renal transplantation, recent febrile illness, or drug that can affect renal function were excluded.
Serum creatinine and serum NGAL concentrations were estimated initially within 24 hours of admission and another sample within 72 hours of admission.
Method of measurement of serum NGAL
The assay was carried out by an enzyme linked immunosorbent assay (ELISA) technique using reagents provided by Quantikine (R&D Systems, Inc.). In this technique, a monoclonal antibody specific for NGAL has been precoated on a microplate. Standards and samples were pipetted into the wells and any NGAL present was bound by the immobilized antibody. After washing away any unbound substances, an enzyme-linked monoclonal antibody specific for NGAL was added to the wells. Following a wash step to remove any unbound antibody-enzyme reagent, a substrate solution was added to the wells and color developed proportionately to indicate the amount of NGAL bound in the initial step. The intensity of color was measured at the wave length of 450 nm.
Statistical Methods
Standard computer program SPSS for windows, version 10.0 (SPSS Inc.), was used for data entry and analysis. All numerical variables were expressed as mean ± SD. Comparison of two groups was done using Student's t-test and Mann–Whitney test for parametric and nonparametric variables, respectively, while analysis of variance (ANOVA) and chi-square (χ 2 ) test were used to compare the frequency of qualitative variables among the different groups. Pearson's and Spearman's correlation tests were used for correlating parametric and nonparametric variables, respectively. For all tests, the probability (P) value less than 0.05 was considered significant.
Results
In the present study, the main presentation of SIRS patients was gastrointestinal symptoms such as gastroenteritis and severe dehydration (30.4%), while severe sepsis and septic shock were presented by neurological symptoms such as meningitis and convulsion (35% and 52.4%, respectively).
Serum creatinine and NGAL (1st and 2nd) levels were significantly higher in patients with septic shock than in those with SIRS and severe sepsis (P = 0.001), while urinary output was significantly lower in patients with severe sepsis than in those with SIRS and septic shock (P = 0.02; Table 1). Also, there was a high significant difference between septic patients group with AKI and non-AKI patients group with regard to urinary output (P = 0.01) and a high significant difference with regard to serum creatinine and NGAL (P = 0.0001; Table 2).
Comparison between different groups of sepsis regarding laboratory findings.
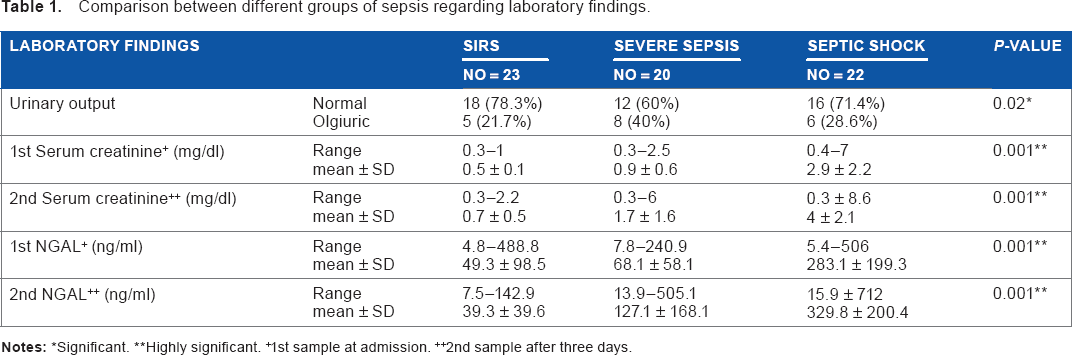
Significant
Highly significant.
1st sample at admission.
2nd sample after three days.
Comparison between patients with sepsis at admission regarding acute kidney injury.

Significant.
Highly significant.
There were no significant differences in NGAL level at admission between nonoliguric and oliguric patients, whereas after three days of admission, it is significantly higher in nonoliguric patients than in oliguric patients (P = 0.03; Table 3). Patients were classified according to pRIFLE at admission: the number of patients at risk stage were 16 (25%), at injury stage were 4 (6.3%), and at failure stage were 9 (14.1%), and after three days their number increased to 19 (29.7%) at risk stage, 9 (14.1%) at injury stage, and 16 (25%) at failure stage with P-values of 0.3, 0.06, and 0.05, respectively, while 35 patients with normal renal function on admission became 20 after three days (P = 0.004; Table 4).
Serum NGAL levels in oliguric and nonoliguric patients at admission and after three days of admission.

Significant.
NGAL at admission.
NGAL on follow-up after three days.
Staging of patients according to pRIFLE classification.
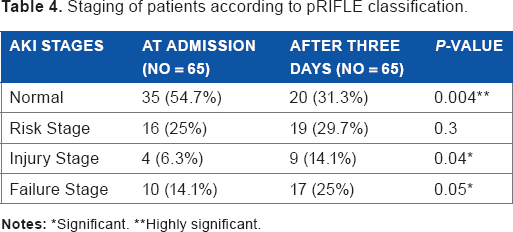
Significant.
Highly significant.
The mean level of NGAL in patients with sepsis at admission significantly increased in a stepwise pattern in different stages of pRIFLE (P = 0.001) and continued to increase after three days (P = 0.001; Table 5).
Comparison of NGAL level between stages of acute kidney affection at admission and after three days of admission.
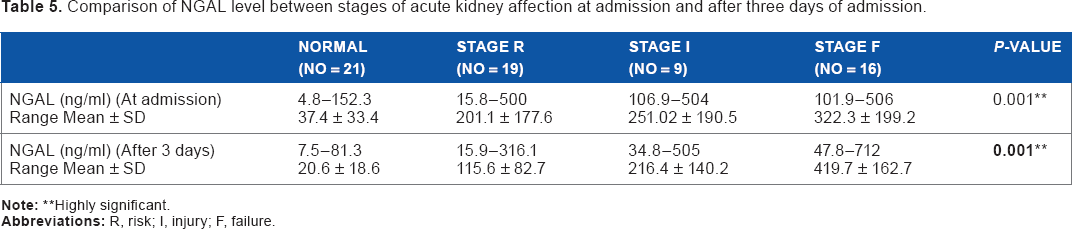
Highly significant.
Also, there was a positive significant correlation between serum creatinine and NGAL at admission and after three days of admission, reflecting the importance of NGAL as a renal function test (Table 6).
Correlation between serum creatinine and NGAL in patients.
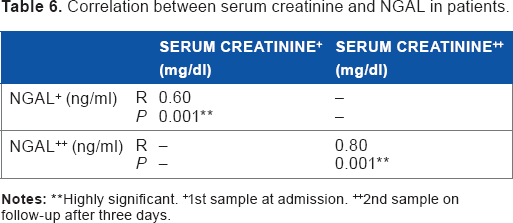
Highly significant.
1st sample at admission.
2nd sample on follow-up after three days.
The receiver-operating characteristic (ROC) curve for serum creatinine and NGAL at admission showed area under the curve (AUC) of 0.93 ± 0.03 and 0.94.7 ± 0.03, respectively, with cutoff values of 0.9 and 40, respectively.
Meanwhile, ROC analysis of serum NGAL showed a higher sensitivity of 90.9% for AKI than serum creatinine (82.7%; Table 7). After three days of admission, serum creatinine shows an AUC of 0.9 with sensitivity of 95.5% and specificity of 95% at a cutoff value of 0.7 mg/dL compared to NGAL, this means that serum creatinine is more specific for follow-up of kidney injury than NGAL (Table 8).
Cutoff value, AUC, sensitivity, specificity, and predictive values for serum creatinine and NGAL in prediction of acute kidney affection in patients at admission.

Cutoff value, AUC, sensitivity, specificity, PPV, and NPV values for serum creatinine and NGAL in prediction of acute kidney affection in patients after three days of admission.

Discussion
In the present study, we found that urinary output was significantly lower in patients with severe sepsis versus septic shock and SIRS (P = 0.02). These results in accordance to the study by Uchino et al. 5 reported that severe sepsis is a highly prevalent syndrome that prompts admission to intensive care and a leading precipitant of AKI and oliguria. The current study showed that there was a highly significant statistical difference between sepsis patients with AKI and sepsis patients without AKI with regard to serum creatinine and serum NGAL (P = 0.0001), also found that some of these patients might develop loss of renal function after three days, and serum NGAL identified these patients before such loss of renal function. There might be alternative explanations for the serum NGAL (+)/serum creatinine (—) syndrome that a small number of patients might have died soon after serum NGAL testing, possibly too early to manifest serum creatinine (+) AKI. 6 In the present study, we found that a significantly statistical difference with regard to urinary output between sepsis patients with AKI and patients without AKI and serum NGAL level after three days of admission is slightly higher in nonoliguric patients than in oliguric patients (P = 0.03).
Our result was in agreement with the study by Kellum et al. 7 who reported that AKI can occur without affecting urine output and classifying AKI as oliguric or nonoliguric has a prognostic value, rather than a diagnostic indication. Also, in agreement with the study by Devarajan 1 who reported that immediately after a kidney injury, blood urea or creatinine levels may be normal and the only sign may be decreased urine production. At the same time, the degree of oliguria does not necessarily correlate with the severity of injury, and interventions including diuretics, dopamine, and mannitol can cause disproportionately higher urine output.
In the current study, 30 patients developed AKI; according to the pRIFLE classification, 25% of patients at admission satisfied the R criterion in their pRIFLE, 6.3% of patients satisfied the I criterion, and 14.1% of patients satisfied the F criterion, while 35 patients were with normal renal function on admission. We found that by follow-up the R criterion patients increase to 29.7%, patients with I criterion increase to 14.1%, and F criterion patients increase to 25% with P-values of 0.3, 0.06, and 0.05, respectively, while 35 patients with normal renal function on admission became 20 patients after three days (P = 0.004). Our study also was in agreement with the study by Akcan-Arikan et al. 8 who reported that AKI occurred very early in the pediatric intensive care unit course, most often within two days of admission and pRIFLE can serve well to improve understanding of AKI epidemiology and potentially optimize evaluation and treatment for AKI in children.
Our results showed a significant positive correlation between serum NGAL and creatinine levels on the first day and after three days of admission in all sepsis patients, reflecting the importance of serum NGAL as a renal function test.
In addition, we found significantly higher serum NGAL in stage R category of pRIFlE criteria than in the control group. This ascertains the high sensitivity of serum NGAL as a predictor of AKI.
In our patients, both higher serum NGAL values and presence of septic shock were associated with more severe AKI. We also found that serum NGAL relates to disease severity, as it was significantly elevated in those with severe AKI in patients with septic shock and indirectly associated with a worse outcome (increased mortality in those with AKI).
Similarly, Haase et al. 6 found that without diagnostic increases in serum creatinine, NGAL-positive patients with sepsis-related conditions might likely have subclinical AKI and therefore carry a worse prognosis, as indicated by the need for renal replacement therapy than serum NGAL-negative patients.
Meanwhile, ROC analysis for serum creatinine shows an AUC of 0.9 with sensitivity of 95.5% and specificity of 95% at a cutoff value of 0.7 mg/dL compared to serum NGAL, this means that serum creatinine is more specific for follow-up of AKI in sepsis than NGAL, more specific for kidney. Our results were in agreement with the study by Hamed et al. 9 who concluded that serum NGAL is raised in critically ill septic children in pediatric ICU and is a marker of bacterial infection and systemic inflammation. However, in AKI associated with sepsis, serum creatinine is more sensitive and specific than serum NGAL for follow-up of AKI.
In our study, ROC analysis was performed to predict mortality, AUC for serum NGAL and serum creatinine (0.60 ± 08 and 0.49 ± 0.09, respectively), and at admission and after three days AUC for serum NGAL and serum creatinine (0.90 ± 0.03 and 0.86 ± 0.05, respectively), which means that serum NGAL at and after admission is more specific in prediction of mortality than serum creatinine. In contrast, the study by Zappitelli 10 reported that serum NGAL was a good diagnostic marker for AKI development (AUC 0.78) and persistent AKI for 48 hours or longer (AUC 0.79) but not for mortality from AKI, when it was recorded, an increase in serum creatinine had occurred (AUC 0.63).
Early prediction of AKI by current clinical and laboratory methods remains inadequate, and NGAL has emerged as a promising noninvasive biomarker of kidney injury; there were some limitations that must be considered.
Although the majority of NGAL in urine or blood derives from the injured kidney, nonrenal NGAL sources have been reported, which might adversely affect the diagnostic accuracy. The effect of CKD on the accuracy of NGAL for AKI prediction or differentiation from prerenal states remains a confounding factor that is open to further research. The available data suggest that patients with stable CKD display low concentrations of NGAL similar to normal controls, but those with progressive CKD may exhibit higher concentrations that may approach those seen in prerenal states or even in mild forms of AKI. The lack of a gold standard AKI definition, the lack of specific cutoff values for NGAL, and differences in clinical assay characteristics are additional limitations to the widespread use of NGAL in clinical practice at the present time. 11
From our results, we strongly recommend early measurement of serum NGAL level in sepsis as a clinically useful marker for early prediction of evolving AKI and for grading of its severity.
Additionally, earlier detection may lead to earlier intervention or more focused efforts to restrict nephrotoxic agents such as certain antibiotics that would propagate injury.
Author Contributions
Analyzed the data: NMI. Laboratory data analysis: WMAEH. Wrote the first draft of the manuscript: SEM. Contributed to the writing of the manuscript: MF, SEM, NMI. Agree with manuscript results and conclusions: MF, SEM. Jointly developed the structure and arguments for the paper: SEM, MF Made critical revisions and approved final version: SEM. All authors reviewed and approved of the final manuscript.