
Abstract
Terminal 11q deletion, known as Jacobsen syndrome (JBS), is a rare genetic disorder associated with numerous dysmorphic features. We studied two cases with multiple congenital anomalies that were cytogenetically detected with deletions on 11q encompassing JBS region: 46,XX,der(11) del(11)(q24). Array comparative genomic hybridization (aCGH) analysis confirmed partial deletion of 11.8–11.9 Mb at 11q24.1q25 (case 1) and 13.9–14 Mb deletion at 11q23.3q25 together with 7.3–7.6 Mb duplication at 12q24.32q24.33 (case 2). Dysmorphism because of the partial duplication of 12q was not overtly decipherable over the Jacobsen phenotype except for a triangular facial profile. Aberrant chromosome 11 was inherited from phenotypically normal father, carrier of balanced translocation 46,XY,t(11;12)(q23.3; q24.32). In the present study, both cases had phenotypes that were milder than the ones described in literature despite having large deletion size. Most prominent features in classical JBS is thrombocytopenia, which was absent in both these cases. Therefore, detailed functional analysis of terminal 11q region is warranted to elucidate etiology of JBS and their clinical presentation.
Introduction
Terminal 11q deletion syndrome, also known as Jacobsen Syndrome (JBS), is a rare genetic disorder associated with multiple dysmorphic features and occurs in 1 in 100,000 live births with a female predominance of 2:1.1–4 JBS occurs because of the loss of contiguous set of genes present at 11q23 with deletion size varying from 7 to 20 Mb in size but could be as small as 2.9 Mb in some cases.1,3,5 A “de novo” deletion is seen in 85% JBS patients, and 15% cases arise as a result of parental translocations. 6 Hallmark clinical features of JBS include pre- and post-natal physical growth retardation, intellectual disability, and characteristic facial dysmorphism. We present two cases of JBS who presented milder phenotypes than those described in literature despite of larger deletion size.
Case 1
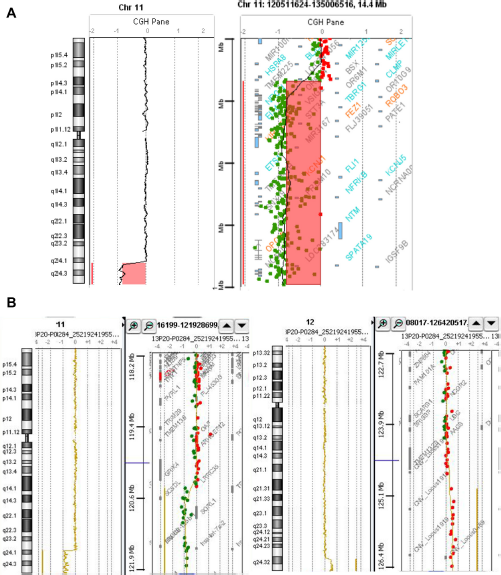
A 4-year-old girl was born to non-consanguineous young parents. No family history of physical and intellectual disability was recorded. Antenatal period was uneventful except suspected intrauterine growth retardation. She was born through Caesarian section with a birth weight of 2.25 kg. She initially had developmental delay but by the age of referral (ie, 4 years), she achieved all motor milestones but was failing to thrive. Short stature and facial dysmorphism were also noted. Her height was 90 cm (<third centile) and was also presented with microbrachycephaly The facial profile showed sparse eyebrows, telecanthus, deep set eyes, strabismus, prominent epicanthal folds, low set dysmorphic ears, depressed nasal bridge, and a bulbous upturned nasal tip. The vermillion of upper lip was thin, and retrognathia along with a high arched palate is noted. No major limb dysmorphism was found except for bilateral short and clinodactyly The neck was short, broad, and had slight webbing. No neurocutaneous markers were noted, and the genitalia was normal (Fig. 1a). Central nervous system examination revealed hypotonia. The child had no meaningful speech despite normal hearing potential, but her receptive language had developed marginally. The child had a low IQ of 30 suggesting severe intellectual disability. 2D echocardiogram showed ventricular septal defect and tricuspid valve tags. The skeletal survey and ultrasonography of the abdomen were normal. Magnetic resonance imaging revealed marginal white matter affection and a thin corpus callosum. Hearing and ophthalmic evaluation including fundus was normal. There were no symptoms of platelet dysfunction on clinical examination in the form of superficial bleeding (which may reflect qualitative and quantitative platelet abnormalities). The platelet count at presentation was normal. Platelet morphology with peripheral smear did not reveal giant platelets or any other abnormality. Karyotyping showed heterozygous segmental distal deletion of 11 with breakpoint at q24 region ie, 46,XX,der(11)del(11) (q24) of “de novo” origin. Oligonucelotide array comparative genomic hybridization [aCGH] characterized the large deletion of 11.8–11.9 Mb size at 11q24.1q25 [arr cgh 11q24.1q25 (123,045,174–134,868,407)x1 (hg19-GRCh37)] (Fig. 2a).

(
(
Case 2
A girl was referred at an age of 6½ years for chromosomal analysis because of multiple congenital anomalies and developmental delay. She was born to young and non-consanguineous parents. The birth history was uneventful. She presented a global developmental delay during examination. At the time of the referral, her height was 107 cm (at the third centile). Physical examination showed microcephaly, flat occiput, epicanthal folds, hypertelorism, mild ptosis, strabismus, low and posteriorly set ears, depressed and low nasal bridge, prominent and bulbous nasal tip, choanal atresia, flat alae nasi, smooth and long philtrum, large open mouth, thin vermillion of upper lip, everted lower lip, retrognathia, and high arched palate. Her neck was short and broad. Arachnodactyly was noted in the upper limb. She had no genital abnormalities (Fig. 1b). Her cardiac evaluations and ultrasound of the abdomen were unremarkable, and skeletal survey showed mild lordosis. She had an affected cognition with an IQ of 37, but did have some meaningful words to her vocabulary. Iron deficiency anemia was detected on the hemogram and later on confirmed by serum iron profiles. The patient neither had abnormal bleeding time nor bleeding manifestation. There was no thrombocytopenia as evident by normal platelet count or platelet dysfunction as evidenced by the clinical examination and platelet morphology on smear examination.
Cytogenetic study exhibited heterozygous deletion of the #11q distal region at the site q24 ie, 46,XX,der(11)del(11)(q24). Oligonucleotide aCGH further confirmed a 13.9–14 Mb deletion at Hq23.3q25, but a relatively large 7.3–7.6 Mb duplication at 12q24.32q24.33 was also observed [arr cgh Hq23.3q2 5(121,000,318–134,868,407)x1, 12q24.32q24.33(126,482,69 8–133,767,986)x3 (hg19-GRCh37)] (Fig. 2b). This structural rearrangement was missed by the conventional cytogenetic analysis. The aberrant chromosome 11 was inherited from the phenotypically normal father who was the carrier of a balanced translocation 46,XY,t(11;12)(q23.3; q24.32).
Discussion
JBS is a rare chromosomal disorder involving terminal deletion of chromosome 11q. The implementation of array technology in the clinics has permitted precise characterization of the deletions and detailed genotype–phenotype correlation in cases with JBS. We present two cases of JBS with deletions spanning 11.9 and 14 Mb, respectively. Despite the difference in the deletion size, both patients had nearly similar phenotypes as shown in Table 1. The critical region underlying intellectual disability7,8 is located within the 4.11 Mb of the 11q telomere encompassing genes SNX19, THYN1, OPCML, VPS26B, NCAPD3, and NTM, which were deleted in our patients. Deletion of the NTM (neurotrimin) gene hampers the normal expression of the NTM protein in the developing nervous system that may promote neurite outgrowth that has been associated with cognitive function.7,8 Larger deletion encompassing all four genes associated with JBS-related thrombocytopenia (FLI1, ETS1, NFRKB, and JAM3) did not manifest a phenotype in both of our patients. Thrombocytopenia is a usual feature in >88% JBS patients. 9 We could not see any correlation between the size of deletion and manifestation of thrombocytopenia; this could be because of the heterogeneous nature of the deletion. Recently, it has been shown that second hit may be a prerequisite for the full blown expression of the thrombocytopenia. 10 JAM3 is suggested as the candidate gene for JBS cardiac phenotype 11 that was deleted in both these patients. However, ventricular septal defect and tricuspid valve tags were observed only in case 1. Absence of heart disease in case 2 even with ETS1 deletion is consistent with the hypothesis of a more centromeric localization of the cardiac critical region.12,13 A crucial role of the ETS1 gene in heart development is reported. 13 ETS1 gene is also proposed as a candidate gene for involvement in limb anomalies, which was not observed in our cases. 14 Although most features of JBS may be caused by deletion of different sets of contiguous genes, relative difference in the phenotypic expression may depend on the genetic background and gene–gene interactions in individual patient. The absence of typical JBS features in our patients may exclude an impact of genes in the deleted region on these features, but indicate a possible proximal localization of critical genes for JBS phenotype suggestive of a reduced penetrance. The overlap of phenotypic features between JBS and Noonan syndrome was not characteristically discernable in our patient other than a triangular facial appearance. 15 The current study suggests that the detailed analysis is necessary in cases with milder phenotype. This can help to understand the underlying genetic etiology in 11q deletion phenotypes.
Comparison of clinical features observed.

Author Contributions
Conceived and designed the experiments: FJS, JA. Wrote the first draft of the manuscript: FJS, JJS, CD, MR. Contributed to the writing of the manuscript: FJS, MR, CD, JA, AP, DN, JJS. Agree with manuscript results and conclusions: FJS, MR, CD, JA, AP, DN, JJS. Jointly developed the structure and arguments for the paper: FJS, MR, CD, JA, AP, DN, JJS. Made critical revisions and approved final version: FJS, MR, CD, JA, AP, DN, JJS. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
Our thanks to Dr. Sunil Trivedi for giving critical comments and to both the families for their kind co-operation.