
Abstract
Background
Despite tremendous importance of early cancer diagnosis in children, few studies on this topic have been conducted in Egypt. Early stage diagnosis can have a positive effect on prognoses and the quality of life of children with cancer. We investigated delays in the diagnosis of childhood cancers in Egypt and determined the factors associated with these delays.
Methods
This retrospective study included 172 children with cancer from two pediatric oncology units. The interval between symptoms onset and final diagnosis for each child was estimated and examined by univariate and multivariate analyses to determine correlations with the child's sex, age at diagnosis, type and site of malignancy, family residence, socioeconomic status, and parental educational level.
Findings
The median total diagnosis delay period was 47 days caused by patients and/or parents (8 days) and diagnosis (28 days). Statistically significant patient factors associated with delayed diagnosis were age (<5 years), lower parental education, and socioeconomic status. Sex residence and family size were not significant. Malignancy type and tumor site significantly affected the time for diagnosis. The lowest median value was associated with germ cell tumors (GCTs) and leukemia, and the highest value was in children with brain tumor. Missed diagnoses were initially recorded in 39.5% of the patients and were associated with patient and tumor factors.
Interpretation
Delayed diagnosis of childhood cancer is related to age, family, socioeconomic status and parental education, and cancer type and site. Efforts should be made to promote awareness, develop effective steps to eliminate possible contributing factors, and determine the best intervention method.
Introduction
Despite tremendous advances in the field of pediatric oncology during the past two decades, cancer remains a leading cause of death in children. 1 Early diagnosis is fundamental for cancer management because it allows treatment of early stage disease, which results in better prognoses for these children and can also have a positive effect on their quality of life.2,3 There are many published reports on children with cancer in developed countries;3–5 however, few articles on this subject have been published in developing countries, particularly in Egypt. In South Africa, Stefan et al found a median total delay of 34 days in the diagnosis of childhood cancer. 6 In Nigeria, James et al determined the median overall lag time in the diagnosis of childhood cancer to be 13.1 weeks. The shortest lag time was 8.1 and 8.7 weeks for patients with leukemia and Wilms’ tumor, respectively, and the longest was 101.7 weeks for patients with Hodgkin's disease. 7
A study examining the delays in childhood cancer diagnosis in Egypt would be particularly important because of the wide prevalence of poverty, cultural differences between people, and the economic differences that exist among Egypt's population. We investigated factors associated with delays in the diagnosis of childhood cancers in Egypt and discussed steps that are essential for shortening these delays in diagnosis.
Subjects and Methods
A predesigned questionnaire was used to collect data from parents or legal guardians of 172 children (0–15 years of age) diagnosed with cancer at two referral centers in Egypt between November 2010 and November 2012. Cases were collected from the Zagazig University Pediatric Oncology Unit, which is a regional referral center for children with cancer that serves the eastern Egyptian delta, the canal areas, and parts of the Sinai with approximately 5 million inhabitants. The Banha Pediatric Oncology Unit at the specialized children's hospital serves approximately 3 million inhabitants of the center of the delta. The sociodemographic characteristics of these two areas are representative of a larger Egyptian cohort that includes the entire delta. The ethics committees of both centers approved this study.
The patients’ data, including age, sex, parental educational level, socioeconomic status, duration of illness at diagnosis, and type of malignancy were recorded. The first symptoms of the malady, first diagnosis by a health care professional, first doctor's notes, and any prescription given before the final diagnosis were also recorded. After a review of the available patients and their cancer types, the following most commonly observed malignancies were included in the analysis: leukemia (including acute lymphoblastic leukemia, acute myeloid leukemia, and chronic leukemia), lymphomas (including Hodgkin's and non-Hodgkin's lymphoma), Wilms’ tumor, neuroblastoma, rhabdomyosarcoma, germ cell tumors (GCTs), brain tumors, histiocytosis, bone tumors (including Ewing's sarcoma and osteosarcoma), and other cancers, which included less common malignancies (eg, nasopharyngeal carcinoma, thymoma, and others).
A child with cancer was considered to be symptomatic starting at onset of unrelieved symptoms that were directly attributed to the malignancy. The term “patient delay,” also called “parent delay” in some articles,4–9 was defined as the interval between symptoms onset and the first visit to the primary doctor. We used the term “patient factors” to describe factors associated with delay attributed to the patient such as age, sex, family size, parental education, residence, and socioeconomic level. We used the term “diagnosis delay” (commonly referred to as “physician delay” or “health system delay” by other authors) 6 to describe the interval between the first contact with the primary doctor and diagnosis. “Tumor factor” denotes the type of tumor. The total delay was calculated from the date of symptoms onset until the date of diagnosis and the beginning of treatment. The term “misdiagnosis” was used when the malignant disease was not the first diagnosis and another benign disease was suspected.
Statistical analysis
The factors associated with total delays were identified by univariate analysis to assess the impact of each factor separately on total delays and to determine correlations between possible contributing variables and total delays. For comparison of two groups of categorical variables, independent
Results
A total of 172 children with different malignancies were included in this study [boys, 105 (61%); girls, 67 (39%); boy:girl ratio, 1.5:1; age range, 6 months–14 years; mean age, 5.3 years; median age, 5 years].
The median patient delay from the time of symptom appearance to seeking medical advice was 8 days (mean, 21 days), and the median diagnosis delay was 28 days (mean, 29 days). The median total delay period was 47 days (mean, 50 days) (Table 1).
Length of delay in days for the total series.

We analyzed the risk factors associated with total delay of diagnosis in children. We determined correlations of these factors with the mean total delays in cancer diagnosis. The distribution of patients in each factor group and the associations with the mean total delays for each factor are shown in Table 2; a
Patient factors associated with total delayed diagnosis of cancer in Egyptian children Characteristic.

Sex (
For the factors associated with delayed diagnosis, the median total delay period was 47.5 days (mean, 49.85), which varied from 3 days to 372 days (Table 3).
Length of delays (days) by type of malignancy.

A significant difference in total delays for different diagnoses was found (
Determinants of delayed cancer diagnosis obtained from multivariate analysis using a linear regression model.

After performing univariate analysis to determine the factors that were significantly associated with total delays in diagnosis, the statistically significant factors (diagnosis, socioeconomic level) were then included in a multivariate analysis using a linear regression model to identify the independent variables associated with total delays in cancer diagnosis. As shown in Table 4, socioeconomic level was identified as the only statistically significant and independent determinant of delayed cancer diagnosis (
We analyzed the median patient delay from the first appearance of symptoms until referral to a primary physician and the median patient delay associated with the health system until final diagnosis. The comparison is illustrated in Figure 1.
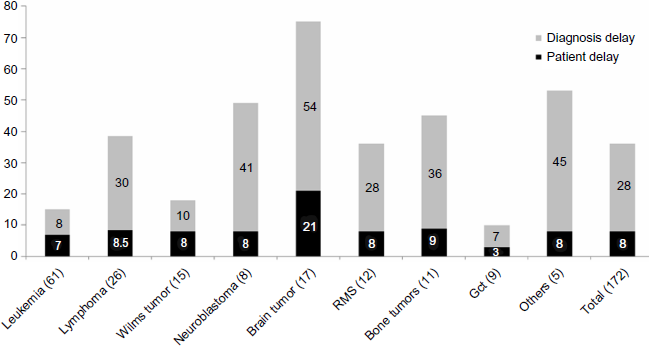
Median delay (days) associated with patient factors for different tumor types.
Misdiagnosis was initially recorded in 68 patients (39.5%). Of the 61 children diagnosed with leukemia, 23% were initially misdiagnosed. Of the children diagnosed with Wilms’ tumor, 33% were initially misdiagnosed. Of the children diagnosed with brain tumors and histiocytosis, 70 and 75%, respectively, were initially misdiagnosed. Initial misdiagnosis occurred in 42.3% of children with lymphomas, 50% of children with neuroblastoma, 45% of children with bone tumors, 50% of children with rhabdomyosarcoma, and 11% of children with GCTs (Fig. 2).

Numbers of cases misdiagnosed in our series by type of diagnosis.
Discussion
This study is one among a few studies concerning delay of cancer diagnosis in Africa,6,7 and to the best of our knowledge, is the first in Egypt. In our series, the median total delay period was 47 days, diagnosis delay was 28 days, and patient delay was 8 days. A number of studies have investigated factors associated with delayed diagnosis in children.3–8 In 2007, Dang-Tan and Franco published a review of 23 epidemiological studies that examined diagnosis delays in childhood cancer. They found that factors associated with diagnosis delays varied across studies 3 and included the child's age, level of parental education, type of cancer, presenting symptoms, and others. 3
Our results are similar to the results reported in Israel, which is a geographically closed country. In 2004, Haimi et al reported similar values of 7 weeks, 4 weeks, and 1 week for the median total delay period, diagnosis delay, and patient delay, respectively. These similarities reflect the same milieu for two countries that are geographically close. 9 In contrast, the median total delays in a 2011 study conducted in South Africa reported a much shorter total delay of 34 days; this can be explained by the fact that this study was conducted at the Taygerberg Hospital, a center of excellence situated in a large urban area where all health services are readily accessible. 6 Approximately half of our results were reported in patients from Nigeria in 2010 with corresponding results of 13.1, 8.8, and 2 weeks for the median total delay period, diagnosis delay, and patient delay, respectively. 7 Differences in health attitudes and related socioeconomic and cultural factors between the two areas may have influenced our results.
There was no statistically significant difference in the total delayed diagnosis period between males and females (
Parental education and socioeconomic level, both of which are closely related, were determined to be important factors in suspecting and interpreting symptoms and signs of malignancies in our series. A statistically significant correlation (
In our series, the type of cancer clearly influenced diagnostic delay. Most patients diagnosed with GCTs had teratomas, sacrococcygeal tumors, and testicular tumors. Because these tumors were often visible from outside the body or present with a mass, diagnosis was often made early and treatment initiated earlier. Klein-Geltink et al reported patient and physician delays of 0.6 days and 1 week, respectively, for patients with GCTs.
4
In our series, a significant difference in total delays was found between different types of diagnoses (
In our study, the median patient delay period (8 days) was also affected by the type of tumor, which was shortest with GCT, leukemia, and tumors presenting as masses (eg, Wilms’ tumors, neuroblastoma, and bone tumors) and longest with brain tumors. This finding may be because the presenting features of these malignancies are more alarming to parents, whereas in those with brain tumors, the symptoms are often non-specific, vague, and misleading. In such patients, symptoms are often attributed to a more benign condition, such as fatigue, simple eye problems, or any another conditions. An increase in public awareness and authorization of young people to seek and obtain prompt help for any complaint would reduce delays in cancer diagnosis in children.
It is the authors’ opinion that the problem with delay in diagnosis is not confined to the patient, and the initial contact of patient with a primary care physician has a considerable impact on early childhood cancer diagnosis. The ability of primary care physicians to recognize serious symptoms that may indicate cancer varies considerably. In our series, 39.5% of the patients were misdiagnosed. This issue was extensively discussed in South Africa, where misdiagnosis was reported in 58% of patients. 6 The type of cancer may also influence a physician's ability to make a correct diagnose. For example, young children with Wilms’ tumor can have more identifiable signs at presentation than older children. In contrast, children with brain tumors, who often have a slower tumor growth rate than other cancers, present with less menacing symptoms to a general pediatrician. Therefore, efforts to further educate young physicians and general pediatricians about the presenting signs and symptoms of cancer in children will undoubtedly improve the diagnostic skills of the physicians and influence their index of suspicion and time of referral if presented with a child with possible cancer.
This study had certain limitations, including its retrospective nature, the relatively small sample size, and the fact that the patients mainly represented lower Egypt and the delta. Recall bias is a concern, particularly when addressing the beginning of symptoms. We overcame this by reviewing the initial referral letters and contacting the referring doctors when possible.
The influence of delayed diagnosis in children with cancer remains unclear, and more research is required to identify how delays affect morbidity and mortality.
Conclusion
The delay in diagnosis of childhood cancer in Egypt determined in this study was comparable with the findings published by other authors. In our study, delays in the diagnosis of childhood cancer were most influenced by the child's age, family's socioeconomic status and parental education, cancer type, and site of cancer. Every effort should be made to promote public and parental awareness of childhood cancer. Further education of inexperienced physicians should improve their awareness of the signs of cancer, which will allow effective steps to be taken to eliminate possible contributing factors and to determine the best intervention methods.
Author Contributions
Performed statistical analysis and interpretation of the data: RMS. Wrote the first draft of the manuscript: ERA, LMS, NMK. Agree with manuscript results and conclusions: ERA, LMS, NMK, RMS. Jointly developed the structure and arguments for the paper: ERA, LMS, NMK, RMS. Made critical revisions and approved final version: ERA, LMS, NMK, RMS. ERA and LMS had full access to all the study data and take responsibility for the integrity of the data and accuracy of the data analysis. All authors reviewed and approved of the final manuscript.