
Abstract
The usual treatment of gynecologic cancer has been surgery, chemotherapy and radiotherapy. New therapies are being developed to improve efficacy of treatment. Interferons are inducible secretory glycoproteins that have immunomodulatory, antiviral, anti-angiogenic and anti-proliferative effects. Their potential antitumor effect has been demonstrated in many studies. Some patients obtain beneficial effects; in other patients the treatment failure can occur. IFNs can modulate the immune response and inhibition of tumor angiogenesis. When any alteration in gene expression occurs, there is modulation of the receptors of other cytokines and enzymes that control cell function. These alterations can influence the differentiation, cell proliferation rate and apoptosis. The molecular mechanisms that control apoptotic cell death can be improved through cancer management using IFN in single, combination or adjuvant treatment. Malignant cells generally present defects in programmed cell death and apoptosis. Immunomodulation and angiogenesis inhibition are indirect antitumor mechanisms mediated by apoptosis. With regard to immunomodulation, IFNs can have antitumor effects through increases in cytotoxic T cells, natural killer cells and dendritic cells. Angiogenesis inhibition can result from endothelial cell apoptosis. This factor is important in inhibiting tumor genesis and forming metastases. The aim of this review is to discuss the role of Interferon in the treatment of gynecologic malignancies/breast cancer and mechanisms of action.
Introduction
The interferon (IFN) group of cytokines was so named because of their ability to interfere with viral replication. These substances are inducible secretory glycoproteins that are produced in vitro and by eukaryotic cells in response to viral infection or other factors (Di Saia PJ. 1985). They have immunomodulatory, antiviral, anti-angiogenic and anti-proliferative effects (Platanias LC, 1995; Haller O et al. 2006). Over recent decades, their effects have been used and studied in relation to neoplasias. Current research is now showing new mechanisms of action. It has been demonstrated that some patients obtain beneficial effects whereas treatment failure can occur in other cases. Our purpose here is therefore to discuss this.
Interferon
Structure
IFNs can be divided in types I and II. Type I consists of IFN-α, IFN-β, IFN-ω and IFN-κ while Type II consists of IFN-γ. IFN-α and IFN-β has a length of 166 amino acids and a 20-amino-acid secretory peptide at the aminoterminal end. These two IFNs have about 45% homology of their nucleotides and 29% homology of their amino acid sequences. IFN-γ has a length of 143 amino acids and a 20-amino-acid secretory peptide (Gray PW and Goeddel DV, 1982). Type I is coded by genes on chromosome 9, and type II is coded by a single gene on chromosome 12 (Platanias LC, 1995; Stark GR, 1998). All of the type I IFNs bind to type I IFN receptors, while IFN-γ binds to type II IFN receptors (Stark GR, 1998). Many studies have demonstrated that type I IFN receptors (IFNRs) have a multichain structure in normal and malignant hematopoietic cells (Platanias LC et al. 1993; Uzé G et al. 1995). IFNRs can be divided into two types: IFNAR1 and IFNAR2 (Uzé G 1990 et al.). Both of these are able to mediate the biological effects of IFNs (Colamonici OR and Domanski P, 1993). Type II IFN receptors consist of two subunits: IFNGR1 and IFNGR2 (Novick D et al. 1994). These receptors are also found in cells of hematopoietic origin.
A long-acting pegylated form (PEG-IFN) has been developed to improve the pharmacological properties of IFN α-2b. PEG-IFN is a mixture of pegylated proteins with differing sites of PEG attachment (Wang YS et al. 2000). PEG conjugation is thought to increase the serum half-life, prolonging patient exposure to IFN-alpha2b without altering the biologic potency to the protein (Grace M et al. 2001). Satisfactory results have been demonstrated in some diseases, such as hepatitis C (Shepherd J et al. 2007; Charlton M, 2005).
Mechanisms of action
After IFN-α and IFN-γ bind to their receptors, the specific tyrosine kinases (tyk2) are phosphorylated, along with other tyrosine kinases: JAK-1 and JAK-2 (Janus-activated kinase). As activated tyrosine kinases induce the formation of protein subunits, the IFN-stimulated gene factor (ISGF)-3 α complex is guided to the nucleus, thereby building a DNA-binding complex specific for the IFN-stimulated response element (ISRE). The formation of signal transduce includes IFNAR1, IFNAR2, JAK1, JAK2, STAT1 and STAT2. A similar sequence of events occurs when the IFN-γ receptor is activated, but STAT-1 homodimer binds to DNA elements that are termed gamma-activated sites (GAS). The events of IFN-γ signaling include the action of some proteins: IFNGR1, IFNGR2, JAK1, JAK2 and STAT1: see Figure 1 (Stark GR et al. 1998).
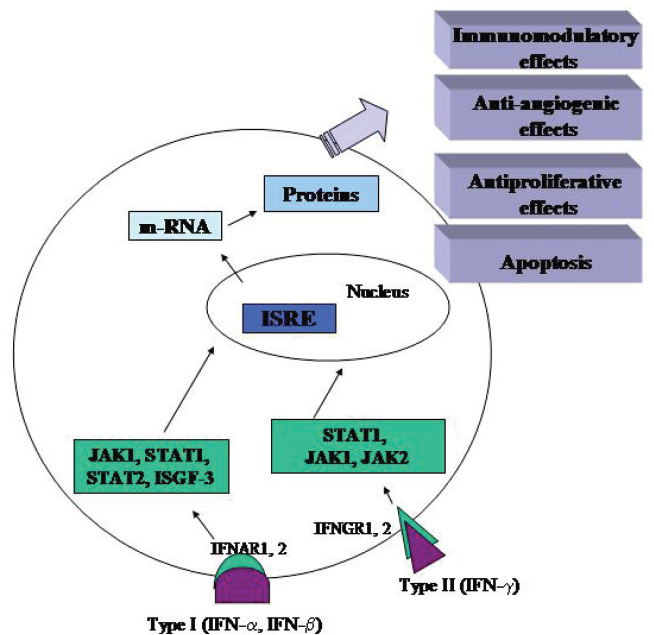
Mechanisms of action of Interferons.
With the great advances in techniques for using proteomics and gene microarrays, the mechanisms for IFN action have become easier to view. IFNs perform their effects through binding to cell surface receptors and activating members of the JAK kinase family. Activated JAK kinases phosphorylate the STAT (signal transducer and activator transcription) family of transcription factors (Caraglia M et al. 2005). The antitumor effects result from direct action on the proliferation or antigenic composition of tumor cells, or from the effect of modulation on immune effector cell populations with tumor cell specificities (Kufe DW et al. 2003).
IFNs can affect cell proliferation or induce cell differentiation of the tumor cells. In addition to this, they can have indirect effects, such as modulation of the immune response and inhibition of tumor angiogenesis. IFN regulates gene expression and modulates the expression of the proteins on the cell surface. When any alteration in gene expression occurs, there is modulation of the receptors of other cytokines and enzymes that control cell function. These alterations can influence the differentiation, cell proliferation rate and apoptosis (Kufe DW et al. 2003). All of the effects of IFN, whether direct or indirect, are a result of gene expression regulation. IFN-α and IFN-β can act in all phases of the mitotic cell, particularly G1 (Balkwill F and Taylor - Papadimitriou J 1978).
It is recently shown that the binding affinity of interferon toward IFNAR1 and IFNAR2 receptors correlates with antiviral and antiproliferative effects, (Piehler J et al. 2000; Jaitin DA, 2006; Kalie E et al. 2007; Slutzki M et al. 2006). Human tumor associated macrophages may become tumoricidal under the influence of IFN, producing a diffusable substance in agarose culture which causes the antiproliferative effects on tumor cells (Saito T et al. 1986).
Apoptosis is a genetically regulated cellular death. It is important in the control of many physiological events (embryonic development and immune regulation), and it is important for eliminating gene damage, i.e. for avoiding uncontrolled cell proliferation with genotype alterations and diseases, among which cancer (Thompson CB, 1995), being an attractive mechanism for the antitumor action of IFN. The molecular mechanisms that control apoptotic cell death can be improved through cancer management using IFN in single, combination or adjuvant treatment (Lowe SW and Lin AW, 2000; Krammer PH, 2000). Mutations in p53, the first tumor suppressor gene found to be related to apoptosis, occur in most malignant tumors, and they are frequently associated with advanced stage and poor prognosis (Wallace-Brodeur RR and Lowe SW, 1999).
Malignant cells generally present defects in programmed cell death and apoptosis. IFN can act to induce apoptosis, and the mechanism for this consists of activating the caspase cascade (Ashkenazi A and Dixit VM, 1998; Earnshaw WC et al. 1999; Barton C et al. 2005; Muscat A et al. 2006; Saidi RF et al. 2006). The apoptosis induced by IFN-α was associated with the activation of caspases 1, 2, 3, 8 and 9 (Thyrell L et al. 2002). The initiators of the caspase cascade are caspases 8 and 9, and the main effector is caspase 3. (Thornberry NA and Lazebnik Y, 1998).
Immunomodulation and angiogenesis inhibition are indirect antitumor mechanisms mediated by apoptosis. With regard to immunomodulation, IFNs can have antitumor effects through increases in cytotoxic T cells, natural killer cells and dendritic cells. Angiogenesis inhibition can result from endothelial cell apoptosis. This factor is important in inhibiting tumor genesis and forming metastases (Lindner DJ, 2002).
The objective of an ideal immunotherapy method is the complete destruction of all neoplastic cells. Additional studies are still needed in order to attain full understanding of the mechanism for IFN action. This is fundamentally important for discovering new strategies about cancer treatment, either on its own or in association with other therapeutic strategies, such as surgery and chemotherapy.
Clinical Use of IFN in Gynecological Cancer
Lower genital tract
Over the last two decades, several studies have shown the use of IFN for treating cervical intraepithelial neoplasia (CIN) (Byrne MA et al. 1986; Choo YC et al. 1986; Cinel A et al. 1991; Di Roma E et al. 2001; Dunham AM 1990; Frazer IH et al. 1999; Frost L et al. 1990; Grismondi GL et al. 1995; Katesmark M et al. 1999; Micheletti L et al. 1992; Murta EF and Tavares Murta BM, 2004; Rotola A et al. 1995; Schiffman MH, 1995; Sikorski M and Zrubek H, 2003). Physical methods are the ones most utilized for treating high-grade lesions. Among these are loop electrosurgical excision procedure (LEEP) and laser, for treating CIN II, and conization for CIN III (Di Roma E et al. 2001). Nonetheless, the use of IFN has shown promise. Stellato et al. (1992), studying the effects of intralesional IFN-α-2β in patients with CIN in association with human papillomavirus (HPV) infection, obtained a complete response from 33% of the cases, partial regression in 58% and therapeutic failure in 8% (Stellato G, 1992). However, Byrne et al. using topical gel containing IFN-α on CIN cases, (Byrne MA et al. 1986) and Frost et al. applying intralesional IFN-α-2β, obtained results that were similar to those using placebo (Frost L et al. 1990).
Several studies have shown good results from the use of IFN-β for treating CIN cases. Cinel et al. utilizing topical cream containing IFN-β on patients with CIN in association with HPV infection, obtained a complete response from 85.36% of the patients with CIN I, 84.20% with CIN II and 37.50% with CIN III (Cinel A et al. 1991). Grismondi et al. treated 58 patients with CIN in association with HPV infection, using intramuscular IFN-β, and obtained a complete response from 87.9% of the cases (Grismondi GL et al. 1995). Micheletti et al. treated 32 women with intralesional IFN-β, also with a diagnosis of CIN in association with HPV infection, and obtained a complete response from 71% of the patients with CIN I, 64% with CIN II and 45% with CIN III (Micheletti L et al. 1992). Cazorla et al. treated 39 women with diagnoses of CIN I and CIN II, using intramuscular IFN-β, and obtained a response rate of 75%, with a recurrence rate of 25% (Cazorla E et al. 2005). Katesmark et al. utilizing intralesional IFN-β in 26 women with diagnoses of CIN I and CIN II, observed that the lesion disappeared in 73% of the cases (Katesmark M et al. 1999). Rotola et al. comparing the use of intralesional IFN-β separately and in association with intramuscular IFN-β in patients with CIN observed that associations presented better results (Rotola A et al. 1995).
Studies involving IFN-γ for treating CIN cases have presented therapeutic success (Iwasaka T et al. 1990) but the long-term result has been inferior to surgical treatment (Sikorski M and Zrubek H, 2003). Slotman et al. utilizing subcutaneous IFN-α-2b in a patient with intraepithelial neoplasia in the vulva, vagina and uterine cervix, showed that the lesion became reduced at all sites, and the uterine cervix cases presented complete remission of the disease (Slotman BJ et al. 1988).
With regard to invasive neoplasia of the uterine cervix, IFN has also been utilized in cases at advanced stages (III and IV), generally in association with radiotherapy and chemotherapy. A randomized study on patients with cancer of the uterine cervix in stage IIIB, comparing the use of IFN-α-2b in association with radiotherapy with the use of radiotherapy alone, did not show any significant improvement in the local response and survival of the patients who utilized this association (Yazigi R et al. 2003). The combination of chemotherapy (cisplatin and 5-fluorouracil), radiotherapy, subcutaneous IFN-α-2a and oral retinoic acid at stage IIIB of cervical cancer was well tolerated (Wilailak S et al. 1990).
The association of IFN-α and retinoic acid may have a cumulative antiproliferative effect, thereby improving the sensitivity of the cells to radiotherapy, in the treatment of cancer of the uterine cervix (Basu P et al. 2006). Another association consists of IFN-γ and cisplatin, for treating cervical cancer in association with HPV, and this may increase the sensitivity to anti-Fas in cell lineages in cases of cancer of the uterine cervix that are positive for HPV. The probable mechanism is up-regulation of Fas and the expression of caspase 8, even without alterations in the levels of p53. It is known that, when the Fas ligand binds to the Fas death receptor, this may activate the caspase cascade and lead to apoptosis (Hougardy BM et al. 2005).
In vaginal cancer, Murta and Tavares obtained complete response in treating a patient with invasive vaginal carcinoma using intralesional IFN-α-2b, with total remission of the lesion observed by means of colposcopy and cytology. The patient evolved with pregnancy three years afterwards, without any sign of recurrence during the follow-up (Murta EF and Tavares Murta BM, 2004). Vaginal melanoma is rare and, despite the poor prognosis, may give some response using IFN following (Androutsopoulos G et al. 2005).
Other strategies have been tried in the disease of lower genital tract related to HPV. The preventive vaccines have been developed against a variety of human viral pathogens and are often a cost-effective approach to interfere with the diseases caused by these pathogens (Ehreth J, 2005). In relation to the vaccine against HPV, although these anticipated reductions in CIN 2 and invasive cervical cancer would be impressive, it must be noted that there would still be many serious HPV infections against which the vaccine would not protect. Thus, it will be necessary to educate health care providers and patients about this limitation of the vaccine (Lowy DR and Schiller JT, 2006).
Endometrium
There are few studies on the use of IFN in cases of endometrial carcinoma. Some studies have shown that IFN-β may induce the formation of estrogen and progesterone receptors in vitro (De Cicco F et al. 1988; Codegoni AM et al. 1996) and in vivo (Sica G et al. 1993) endometrial cancer cells. This might predict a greater therapeutic response rate for these tumors, to adjuvant treatment with hormone therapy.
Ovarian cancer/pseudomyxoma peritonei
Patients have limited options with regard to treatment for advanced or recurrent cases of ovarian cancer. Chemotherapy is based mainly on the use of intravenous cisplatin. Another option is the use of IFN, either alone or in association with chemotherapy.
High response rates to ovarian cancer treatment can be attained by means of intraperitoneal IFN administration (Berek JS et al. 1985; Wall L et al. 2003). This exposes the tumor to high concentrations of the drug, with lower systemic toxicity. In addition, it diminishes the hepatic metabolism problems and inactivation before the drug gets close to the tumor cell population. Through this, local stimulation of immunological mediators such as natural-killer cells, T-cells and peritoneal macrophages takes place (Markman M, 1987). Intraperitoneal therapies have been tried, especially for treating minimal residual disease that is confined to the peritoneal cavity, following second-look surgery (Welander CE, 1987; Fujiwara K et al. 2007), and for patients who have no evidence of disease subsequent to surgery and chemotherapy (Alberts DS et al. 2006).
The in vitro cytotoxicity potential is higher when IFN is combined with cisplatin, anthracyclines or alkylating agents (Welander CE, 1987). IFN-α and IFN-γ are active against ovarian cancer, both in vitro and invivo (Wall L et al. 2003; Allavena P et al. 1990; Nehme A et al. 1994). There is in vitro evidence that intraperitoneal IFN-γ can increase the sensitivity of the cancer cells to cisplatin (Nehme A et al. 1994). IFN-γ can inhibit the expression of dysregulated oncogenes, such as HER-2/neu, and increase the response of cells that are resistant to cisplatin (Marth C et al. 1997). IFN-γ has a modulatory effect on cells of the immune system, thereby leading to stimulation of natural killer cells and macrophages, which are both known to have antitumor activity (Berek JS et al. 2003). It also has an antiproliferative effect, and this is improved when in association with cisplatin (Barton C et al. 2005).
IFN-α is active against ovarian cancer in vitro (Freedman RS et al. 1983) and in vivo (Einhorn N et al. 1988); this substance has been used in many phase I and II studies on women with malignant ovarian neoplasia that is persistent to second-look laparotomy (Willemse PH et al. 1990). The Table 1 shows some IFN-α studies.
IFN-α studies in ovarian cancer and their main results.
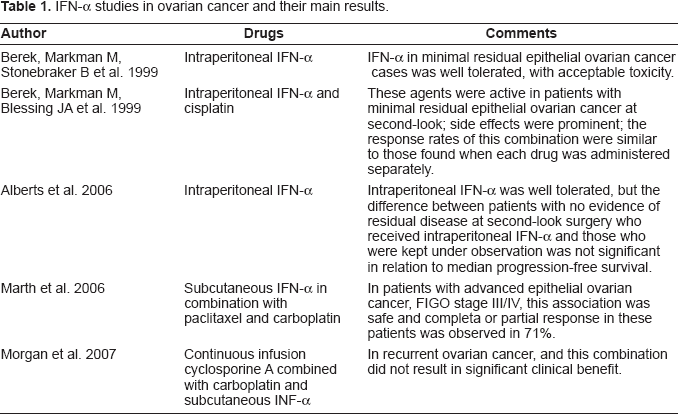
The efficacy of alternating intraperitoneal recombinant alpha-2-interferon (r-alpha 2-IFN) and cisplatin as salvage therapy for less than or equal to 5 mm residual-disease ovarian carcinoma showed pathologic complete remission in 50% of the patients, no limiting toxicity (Nardi M et al. 1990). In the other hand, other study demonstrated that intraperitoneal IFN-α does not seem to improve the results achievable with intraperitoneal carboplatin in this subset of patients, while the toxicity and the costs of the combination are higher than with chemotherapy alone (Bruzzone M et al. 1997).
The adverse effects of Interferon therapy in the ovarian cancer are fatigue, leukopenia and thrombocytopenia, and more rarely nephrotoxicity and myocardial infarction (Abdulhay G et al. 1985).
Pseudomyxoma peritonei is a rare disease and it is characterized by intraperitoneal disseminated mucous produced by adenomucinous tumor cells in implants on peritoneal surfaces. These implants are the final stage of a distribution process following the rupture of an intraperitoneal located mucinous neoplasm. This disease can originate from ovarian mucinous cystadenoma, is a progressive disease and the excessive mucous accumulation causes compression of the intestines, gastrointestinal function is compromised and eventually obstruction is imminent. Consequently, this disease always results in the death of the patient unless radically treated. The main strategies for treatment are aggressive cytoreductive surgery and peritonectomy in combination with intraoperative hyperthermic intraperitoneal chemotherapy (Smeenk RM et al. 2007). Maiche and Sjostrom showed failed treatment of pseudomyxoma peritonei with intraperitoneal IFN-α (Maiche AG and Sjostrom J, 1996).
Breast
With regard to breast cancer, IFN has been utilized in cases of distant metastasis, in which the disease is already incurable. The first-line treatment in these cases with positive hormone receptors is anti-estrogen therapy. When the tumor becomes resistant to this therapy, one option is the use of IFN. By using two forms of treatment together–-a combination of IFN-β and interleukin-2–-some good results have been obtained (Nicolini A and Carpi A, 2005; Nicolini A et al. 2005).
The use of IFN-γ for treating breast cancer is based on the fact that this substance increases the expression of caspase-8, through an up regulation mechanism that involves IRF1 (Interferon Regulatory Factor 1). As mentioned earlier, caspase-8 is involved in the apoptosis mechanism (Ruiz-Ruiz C et al. 2004). On the other hand, Kimmick et al. (2004), demonstrated that the association of IFN-α with interleukin-2 for treating metastatic breast cancer was not effective for improving survival (Kimmick G et al. 2004). There is evidence that the expression of IRF1 and IRF2 is altered in breast cancer in relation to normal breast tissue (Doherty GM et al. 2001). Some studies have shown positive responses in breast cancer treatment when interleukins were used in association with IFN (Gutterman JU et al. 1980; Borden EC et al. 1982).
The combination of tamoxifen and IFN-β may be more effective than the use of tamoxifen alone, and this effect can be observed independent of whether or not the tumor expresses estrogen receptors (Lindner DJ and Borden EC, 1997). It is known that IFN-β may increase the expression of estrogen and progesterone receptors in breast cancer cells in vitro (Sica G et al. 1992). A randomized clinical trial using IFN-β and γ in association with hormone therapy in patients with advanced disease showed that the serum increase in IFN-γ and the decrease in sIL-2R are predictive factors for a good response to treatment (Barak V et al. 1988). Stimulation of cellular immunity by the association of IFN-β and interleukin-2 sequence in patients on tamoxifen treatment had significantly prolonged median overall survival and duration of response compared to the patients treated with tamoxifen (Nicolini A and Carpi A, 2005; Nicolini A et al. 2005; Nicolini A et al. 2006).
The utilization of chemotherapy followed by the combination of IFN-β, retinoids, and tamoxifen was effective in the treatment of metastatic breast cancer. The main side effects were leukopenia, thrombocytopenia, anemia, nausea/vomiting, stomatitis and diarrhea. Toxicity from maintenance therapy was mild and mainly hepatic. This combined approach for the treatment of metastatic breast cancer was feasible (Recchia F et al. 1998).
The utilization of cyclosporine A and IFN-γ after high-dose chemotherapy with peripheral blood progenitor support in women with high-risk primary breast cancer was well tolerated, without increased toxicity (Vahdat LT et al. 2007).
Therefore, the IFN can be a possible therapeutic option in the breast cancer. However, this treatment must be utilized in metastatic tumors and when the tumor becomes resistant to other therapies, because the hepatic toxicity (mainly in hepatic metastasis) and the other side effects.
Conclusion
The treatment of distant metastases is a great challenge in Oncology. Several studies have demonstrated the importance of IFN in cases of advanced disease, whether used alone or in association with chemotherapy, radiotherapy or surgery. In the other hand, interferon treatments can failure in other women.
Immunotherapy has been shown to be a valid option when other therapeutic possibilities have been exhausted. With the new discoveries elucidating the complex mechanisms for IFN action, and the varied responses that the host may present, new horizons have been emerging and space has been opened up for the use of immunotherapy as a single weapon, even in relation to pre-neoplastic lesions. Better knowledge of the interactions shown by IFN in patients with gynecologic and breast cancer may be useful in developing new therapeutic methods with lower toxicity and greater effectiveness, thus promoting better prognosis and quality of life for these patients.
Sources of Funding
Not declared
Conflict of Interest
Not declared
Place Where was Produced the Manuscript
Research Institute of Oncology (IPON)/Discipline of Gynecology and Obstetrics, Federal University do Triângulo Mineiro (UFTM), Uberaba, Minas Gerais, Brazil.
Footnotes
Acknowledgement
We thank CNPq, FAPEMIG and FINEP.