
Abstract
Introduction
Temozolomide and concomitant radiotherapy followed by temozolomide has been used as a standard therapy for the treatment of newly diagnosed glioblastoma multiform since 2005. A search for prognostic factors was conducted in patients with glioblastoma routinely treated by this strategy in our institution.
Methods
This retrospective study included all patients with histologically proven glioblastoma diagnosed between June 1, 2005, and January 1, 2012, in the Franche-Comté region and treated by radiotherapy (daily fractions of 2 Gy for a total of 60 Gy) combined with temozolomide at a dose of 75 mg/m2 per day, followed by six cycles of maintenance temozolomide (150–200 mg/m2, five consecutive days per month). The primary aim was to identify prognostic factors associated with overall survival (OS) in this cohort of patients.
Results
One hundred three patients were included in this study. The median age was 64 years. The median OS was 13.7 months (95% confidence interval, 12.5–15.9 months). In multivariate analysis, age over 65 years (hazard ratio [HR] = 1.88; P = 0.01), Medical Research Council (MRC) scale 3–4 (HR = 1.62; P = 0.038), and occurrence of postoperative complications (HR = 2.15; P = 0.028) were associated with unfavorable OS.
Conclusions
This study identified three prognostic factors in patients with glioblastoma eligible to the standard chemotherapy and radiotherapy treatment. Age over 65 years, MRC scale 3–4, and occurrence of postoperative complications were associated with unfavorable OS. A simple clinical evaluation including these three factors enables to estimate the patient prognosis. MRC neurological scale could be a useful, quick, and simple measure to assess neurological status in glioblastoma patients.
Introduction
Glioblastomas are the most common primary brain tumors in Europe and North America, with an incidence of approximately three to five cases per 100,000 persons 1 over one year. According to the World Health Organization (WHO) classification, 2 glioblastomas are grade IV gliomas and account for approximately 60%–70% of malignant gliomas.3,4
In 2005, after two phase II studies,5,6 Stupp et al reported the results of the European Organisation for Research and Treatment of Cancer and the National Cancer Institute of Canada (EORTC-NCIC) 22981/26981/CE.3 trial and demonstrated that the addition of temozolomide to radiotherapy for newly diagnosed glioblastoma significantly improves the overall survival (OS) and the progression-free survival (PFS). 7 Since those results, after biopsy or surgery, concomitant temozolomide along with radiotherapy followed by six months of maintenance temozolomide has been recognized as a standard of care for newly diagnosed glioblastomas.8,9 But despite recent advances in neurosurgery, radiation therapy, medical oncology, and biology, with, for example, the identification of methylated MGMT promoter as a favorable prognostic and predictive factor, the prognosis of this disease remains poor: the median OS ranges from 8 to 18 months1,10,11 when patients receive the current standard of care. Long survivors are rare, with less than 30% of patients alive at two years and less than 10% alive at five years. 11
The primary aim of this retrospective study was to identify prognostic factors associated with OS in a cohort of patients with glioblastomas treated according to the protocol of EORTC-NCIC trial in daily practice. The objective was to be able to provide an identification of optimal candidate who are worth exposure to this regimen.
Patients and Methods
Data collection and eligibility
All patients with histologically proven glioblastoma diagnosed between June 1, 2005, and January 1, 2012, were prospectively registered in our computerized institutional database (patient identity and treatment characteristics). All patients candidate to be treated by standard radiotherapy and chemotherapy treatment were selected. Patients who did not receive at least one fraction of radiotherapy and one dose of concomitant chemotherapy by temozolomide were excluded. Patients could be assessed even if they did not receive the entire maintenance treatment. A trained neurologist retrospectively collected clinical and radiological characteristics in patients’ charts. The neurological status of the patients was assessed using the five-point Medical Research Council (MRC) scale. 12 In this scale, five grades are described as follows: (0) no neurological deficit; (1) some neurological deficit but function adequate for useful work; (2) neurological deficit causing moderate functional impairment; (3) neurological deficit causing major functional impairment; and (4) no useful function - inability to make conscious responses. The MRC neurological scale was assessed after the biopsy or surgery and before the beginning of the radiotherapy and chemotherapy treatment. The extents of the surgery were defined as biopsy, partial resection, or macroscopically complete resection, which were determined by the surgeon. Toxicity was graded according to the Common Terminology Criteria for Adverse Events of the National Cancer Institute, version 3.0. Medical imaging of the brain, by magnetic resonance imaging and/or by CT scan, allowed assessing the location of the lesion, the presence or absence of mass effect/brain edema/bleeding/necrosis.
Treatment Protocols
Between four and six weeks after surgery or biopsy, the patients began radiotherapy with concomitant temozolomide. The radiotherapy consisted of a fractionated conformal three-dimensional radiotherapy, and a total dose of 60 Gy was delivered in 30 daily fractions of 2 Gy each. During radiotherapy, oral temozolomide was administered at a daily dose of 75 mg/m2, given seven days per week from the first day to the last day of radiotherapy. Maintenance temozolomide was given 4 weeks after the completion of radiotherapy, at a dose of 150 mg/m2 per day for 5 of 28 days during the first cycle, thereafter, if tolerated, at a dose of 200 mg/m2 on days 1–5 of 28 days for a total of six cycles. 7 Prophylactic antibiotics against Pneumocystis carinii were not routinely applied. Antiemetics, antiepileptic drugs, and corticosteroids were prescribed if needed.
Aim and statistical analyses
The primary aim was to identify the relationship between routinely available factors and the length of OS. Secondary objectives were to identify the relationship between the same factors and the length of PFS, to assess treatment compliance and safety.
The Kaplan–Meier method was used to estimate survival times. OS was estimated from the date of surgery (biopsy or resection) to the date of death or the date of the last follow-up examination. PFS was estimated as the time from surgery to documented disease progression or death from any cause, whichever occurred first. The Cox regression model was used to search the relationship between patients’ outcome and numerous factors. Factors identified by a P-value <0.20 in univariate analysis were included in a stepwise multivariate logistic-regression model. All calculations were performed with SAS software version 9.3 (SAS Institute, Inc., http://www.sas.com). P-values <0.05 were accepted as significant.
Results
Patient and tumor characteristics
From June 2005 to January 2012, a total of 155 patients with glioblastoma were diagnosed in our university hospital. A total of 103 patients were included in this study (Fig. 1): 30 patients received their treatment in other centers closer to their residence or were lost to follow-up; 22 patients did not receive the standard treatment based on radiotherapy and chemotherapy with temozolomide as described in the EORTC-NCIC trial. The demographic and clinical characteristics of patients are outlined in Table 1. The median age was 64 years (range: 23–86 years). There were 68 men and 35 women giving a sex ratio of 1.9. WHO performance status was 0 for 37% of cases. MRC scale was 0 (free of neurological symptoms) in 27% of the population. At the time of analysis, 95 (92%) patients had died.
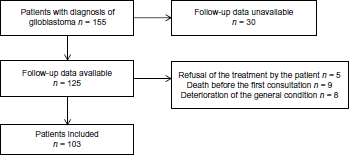
Flowchart.
Patient demographic and clinical characteristics (n = 103).

The initial complaints were sensitivomotor deficiency (29%), intracranial hypertension or/and headache (19%), epileptic seizures (19%), neuropsychological changes with frontal syndrome (9%), balance disorder (12%) speech disturbance (17%), loss of memory (7%), visual symptoms (5%), and others complaints in 10% of patients. The median time from the first symptom to the diagnosis was 19 days (range: 3–383 days). The most common localization of the tumor was the frontal lobe in 39% of cases.
Treatment
Biopsy was performed in 23 patients (22%), 42 patients (41%) underwent incomplete surgical resection, and 38 patients (37%) had a macroscopically complete resection. Thirty-five patients (34%) received carmustine wafers (four to nine implants). Seventy-one patients were on antiepileptic drugs (enzyme inducing and/or nonenzyme inducing), whereas 34 seizures were described. All patients were on corticosteroid during their radiotherapy plus chemotherapy treatment. The median time from diagnosis to the start of radiotherapy was 43 days (range: 10–400 days). Thirty-two patients (31%) completed the chemoradiotherapy protocol followed by six cycles of temozolomide. Six patients did not complete radiotherapy due to disease progression or death. Sixty-five patients did not complete the chemotherapy part of the protocol due to the following reasons: clinical and/or radiological progression (52%), death (8%), toxicity (7%), stability (14%), choice of the patient (14%), and unknown (5%). Only 56 patients (54%) received a second-line treatment. There was no impact of a second line of treatment on OS.
The most frequent adverse event (Table 2) during the chemoradiotherapy protocol was fatigue (in 22% of patients). Eight percent of the patients had grade 3–4 platelet toxicity. Suicide attempts were described in two patients (2%).
Adverse events (n = 72).

OS and prognostic factors
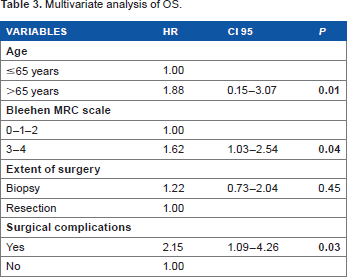
The median OS was 13.7 months (95% confidence interval [CI], 12.515.9 months). The 12-month, 24-month, and 5-year OS rates were 60.2%, 24.6%, and 4.8%, respectively. In multivariate analysis (Table 3), occurrence of postoperative complications (hazard ratio [HR] = 2.15; P = 0.03), age older than 65 years (HR = 1.88; P = 0.01), and MRC scale 3–4 (HR = 1.62; P = 0.04) were associated with shorter OS. OS was not statistically different between patients with an MRC scale 0–2 versus patients with an MRC scale 3–4 (P = 0.06), but we observed a trend for an unfavorable survival in patients with an MRC scale 3–4 (Fig. 2).
Multivariate analysis of OS.

Kaplan-Meier estimates of OS according to MRC scale.
The kind of surgery (biopsy or surgical resection) did not impact OS (HR = 1.22; P = 0.45). Among the patients who underwent surgical resection, the addition of carmustine wafers did not modify survival (P = 0.12). In univariate analysis, gender (P = 0.47), WHO status (P = 0.09), symptoms at presentation, and radiological characteristics (location, mass effect, brain edema, bleeding, and necrosis) had no significant impact on OS (P > 0.05).
PFS and prognostic factors
In multivariate analysis, MRC scale 3–4 (HR = 2.10; P = 0.01) and biopsy without surgery of the lesion (HR = 1.75; P = 0.04) was associated with shorter PFS.
Discussion
In 2005, Stupp et al demonstrated in a randomized phase III trial that temozolomide and concomitant radiotherapy followed by temozolomide improved OS (from a median of 12.1–14.6 months; HR = 0.63) and PFS (from a median of 5–6.9 months; HR = 0.54) with acceptable tolerability compared with radiotherapy alone. 7 Athanassiou et al published a second randomized trial with fewer patients, confirming an improvement in OS with the addition of temozolomide. 13 Indeed, this regimen has become a standard of care, and it has improved the disease outcome by prolonging the OS, increasing the rate of 5-year survivors from 1.9% to 9.8%. 11 In this retrospective study, the outcomes and prognostic factors of glioblastoma patients routinely treated with radiotherapy plus concomitant and temozolomide according to the current standard of care were assessed.
The median OS of glioblastoma patients in our institution was 13.7 months (95% CI, 12.5–15.9 months). Age, MRC neurological scale, and postoperative complications were identified as prognostic factors in multivariate analysis. The current study had limitations, including the limitations of any retrospective study. Important variables such as quality of life, dominant hand, or MGMT methylation status were not evaluated in daily practice. All patients treated with standard chemotherapy and radiotherapy were included in our study whatever be their age or performance status. However, there is a need and requirement to report the use of standard of care in routine population. Such studies offer a perspective of real-world practice, with data more reflective of the prognosis of a patient in the office. Day-to-day clinical care studies can provide different and complementary data about treatment benefits and toxicities. These studies can also help to target the population who may benefit the most from the treatment and identify prognostic and predictive factors. 14 Several institutions reported their experience with the EORTC-NCIC chemoradiotherapy protocol in glioblastoma patients.15–19 The median OS was ranged between 12.0 and 18.3 months. The efficacy of the chemoradiotherapy regimen in our unselected population was between these ranges. The rate of long-term survivors was relatively low in our study with 24.6% of the patients alive at two years and 4.8% alive at five years. Fewer patients (31%) in our institution completed the whole treatment regimen, mainly due to early progression or death.
Prognostic factors in glioblastoma have been identified both in prospective clinical trials (mainly the EORTC-NCIC 22981/26981/CE.3 trial) and in some retrospective studies. Young age, high Karnofsky performance status, extend of resection, recursive partitioning analysis classes, use of adjuvant temozolomide, and high dose of radiotherapy are associated with prolonged OS.7,9,20–22 High glycemia and prolonged hospitalization also represent unfavorable prognostic factors.23,24 In the EORTC-NCIC trial, the addition of temozolomide and the methylation of MGMT promoter are the two main factors that impact OS. In a study aiming to identify prognostic factors for survival in 333 patients with malignant gliomas included phase I and II clinical trials, 22 age, poor Karnofsky performance status, corticosteroid use, short PFS, tumor outside of the frontal lobe, and grade IV gliomas, which were associated with a shorter OS. Our study adds novelty to the current literature through the use of MRC neurological scale and because the population was limited to glioblastoma patients candidate to be treated by standard radiotherapy and chemotherapy treatment. Surprisingly, the MRC neurological scale was rarely used in studies and has never been identified as a prognostic factor in glioblastoma studies. The stringing inclusion criteria aimed to homogenize the study population in order to be able to generalize the results in this population in clinical routine. MRC has provided different scales, the most commonly used is for muscle strength testing. To the best of our knowledge, this is the first report where MRC neurological score appears as a prognostic factor. This score of the neurological deficit was routinely feasible and reproducible in neuro-oncology. This assessment allowed a quick clinical evaluation with a grading scale (0–4) compared with the well-validated 25 performance status assessment by the WHO scale and might be of interest in future study including brain tumors.
The primary aim of therapy in glioblastoma is not only to prolong life but also to maintain or restore a good quality of life. A multidisciplinary management involving neurologists, surgeons, radiation oncologists, medical oncologists, and neuro-radiologists could provide best specific therapies and best supportive care to the patients. The tolerability of the treatment was satisfying with only 6% of grade 3–4 thrombopenia and 3% of infections. Two suicide attempts were described; it emphasizes that supportive care must be an integral part of the management of brain tumors. In the phase III trial, the level of adverse events was higher “with 12% of grade 3–4 thrombopenia and 5% of severe infection. No suicide attempt was described. Two factors might explain the higher level of toxicity in the clinical trial: (1) 47% of the patients completed both radiotherapy and concomitant and adjuvant temozolomide as planned in the clinical trial group and only 31% of patients completed the whole protocol in our study and (2) hematological controls were less frequent in the routine than in the clinical trial.
Conclusion
We identified three prognostic factors in patients with glioblastoma eligible to the standard of chemoradiotherapy and radiotherapy treatment. An age over 65 years (HR = 1.88; P = 0.01), MRC scale 3–4 (HR = 1.62; P = 0.038), and occurrence of postoperative complications (HR = 2.15; P = 0.028) were associated with unfavorable OS. A simple clinical evaluation including age, neurological status according to the MRC scale, and assessment of postoperative morbidity enables to estimate the patient prognosis. MRC neurological scale could be a useful, quick, and simple measure to assess neurological status in glioblastoma patients.
Author Contributions
Conceived and designed the study: CV, GM, EM, JBM, GV, FC, NCBG, EB, SSV, JG, RBG, AP, TM, LC, XP, EC. Analyzed the data: CV, GM, EC. Wrote the first draft of the manuscript: CV, GM, EM, LC, XP, EC. Contributed to the writing of the manuscript: CV, GM, EM, JBM, GV, FC, NCBG, EB, SSV, JG, RBG, AP, TM, LC, XP, EC. Agree with manuscript results and conclusions: CV, GM, EM, JBM, GV, FC, NCBG, EB, SSV, JG, RBG, AP, TM, LC, XP, EC. Jointly developed the structure and arguments for the paper: CV, GM, EM, JBM, GV, FC, NCBG, EB, SSV, JG, RBG, AP, TM, LC, XP, EC. Made critical revisions and approved final version: CV, GM, EM, JBM, GV, FC, NCBG, EB, SSV, JG, RBG, AP, TM, LC, XP, EC. All authors reviewed and approved of the final manuscript.