
Abstract
Background
Exercise has been shown to decrease breast cancer risk and slow the progression of breast cancer. Physician recommendations and clinical research data most often are for gym-based exercise programs. However, the importance of exercise location on mood and stress hormones that may influence adherence to exercise has not been addressed.
Methods
Women first walked for an hour outdoors along a university path and then a week later, for an hour indoors on a treadmill in a typical gym environment. Pre and post outdoor and indoor exercise moods (happy, pleased, sad, frustrated, worried, angry, delighted, and joy) were assessed by a 6 point Likert questionnaire, and saliva samples were collected for analysis of cortisol, and alpha amylase (a surrogate for serum norepinephrine).
Results
Nineteen healthy, non-smoking, postmenopausal women (average age 58 ± 4) participated. Compared with scores after walking outdoors, walking indoors was associated with higher scores of worry (p = 0.02; mean difference 0.9; 95% CI (0.17, 1.6) and frustration (p = 0.03; mean difference 0.9; 95% CI (0.12, 1.6), and lower scores for feelings of being pleased (p = 0.03; mean difference -0.8; 95% CI: -1.7, 0.1) and delighted (p = 0.05; mean difference -0.9; 95% CI: -1.75, -0.02). Changes in salivary hormone levels did not vary significantly between the two environments.
Conclusion
Walking outdoors was associated with improved mood, but walking indoors was not. Improved mood may reduce breast cancer risk indirectly by promoting regular exercise. Physician recommendations for exercise should include gym and non-gym based exercise options.
Introduction
Exercise has been shown to reduce breast cancer risk (Monninkhof et al. 2007; Lee, 2003; Kruk, 2007; Bardia et al. 2006; Bernstein et al. 2005) and delay progression (Cunningham et al. 1998; Holmes et al. 2005). Most but not all of the studies of exercise and cancer incidence have reported a 20%-30% reduction among regular exercisers, and two studies have shown increased risk (Lee, 2003). In a review of 19 cohort studies and 29 case-control studies, Monninkhof identified an inverse association between regular exercise and decreased breast cancer risk for postmenopausal women, with reductions in risk ranging from 20% to 80% (Monninkhof et al. 2007). To allow for comparisons between a wide variety of activities ranging from quietly reading a book to running a marathon, epidemiologic studies generally reduce exercise to generic metabolic equivalents of effort (Ainsworth et al. 2000). This reduction and homogenization of activity may mask important covariates of health such as mood and stress hormone modulation associated with exercise.
Although a seemingly simple concept, exercise is more than the “bodily movement produced by skeletal muscles that results in energy expenditure” (Caspersen et al. 1985). The exact components of exercise that are beneficial have not been defined, although modulation of body size, obesity (Carmichael, 2006) and lean body weight (Wyshak and Frisch, 2000), serum sex steroid hormone levels (McTiernan et al. 2006; Campbell and McTiernan, 2007), immune function (Fairey et al. 2002), and metabolic hormones such as insulin and insulin like growth factors (Boyd, 2003) have been suggested.
The advent of machine-assisted recreational activity is reasonably recent, with the first treadmills for cardiac fitness in 1952. Since then, they have rapidly been adopted as an integral part of general fitness programs. Weather and personal safety issues, plus the ability to safely use treadmills at any hour of the day, has made the treadmill an integral part of fitness programs, especially controlled exercise intervention studies {Galvao, 2005 #119}.
Improvements in mood have been shown by exercise (McArdle et al. 1991; Pawlow and Jones, 2002; Jin, 1989; Jin, 1992; van Stegeren et al. 2006; Chatterton et al. 1996; Slosnik et al. 2000; Morse et al. 1989) and sunlight (Boyce et al. 2003; Lambert et al. 2002). However, most exercise trials have used controlled facility based settings (McTiernan et al. 2004; Tworoger et al. 2007; Campbell and McTiernan, 2007; Fairey et al. 2002) without regard for availability of natural light. Walking outdoors at a self-regulated pace differs in many ways from the same physical activity done in controlled gym-based exercise program and these differences may influence the beneficial effects of exercise on postmenopausal women.
Improved mood could be an important factor in promoting good health and reducing breast cancer risk, as well as prolonging survival in breast cancer patients. The potential usefulness of exercise as a non-drug therapy for depression has been shown by a study by Blumenthal, in which exercise as a treatment for major depression was equivalent to antidepressive medications (Blumenthal et al. 1999). In a subsequent study by the same authors, exercise was again reported to be effective and to have a lower relapse rate (Babyak et al. 2000). Specific to the importance of mood to breast cancer, a Danish study reported that those breast cancer patients who had been hospitalized for depression were significantly more likely to die of breast cancer than women matched for the same stage of breast cancer but who had not been hospitalized for depression (Hjerl et al. 2002). Even mild depression may hinder women from adherence to medical treatment for breast cancer, and hence survival (Somerset et al. 2004).
Salivary cortisol levels and mood states have also been found to be correlated, with higher cortisol associated with negative affect and lower cortisol with positive affect (Hartridge and others 1998). The hypothesis of this study was that specific exercise environments could also modulate mood and influence stress hormones associated with breast cancer (Drell and others, 2003; Hjerl and others, 2002; Knight and others, 2005; Lang and others, 2006; Su et al. 2005; Sephton and others, 2000). Since blood draws are often in themselves stressful, and saliva hormone levels are highly correlated with serum hormone levels (Dorn and others, 2007; van Stegeren and others, 2006), saliva samples were used to monitor changes in cortisol and norepinephrine (as approximated by alpha amylase (van Stegeren and others, 2006)).
Subjects and Methods
Study population
The Human Subjects Research Review Board of the U.S Army and The Palmetto Health Alliance Institutional Review Board in Columbia SC approved this study (February 17, 2005). Subjects were recruited by advertisements and word of mouth. Signed informed consent was obtained from each woman. To reduce any fluctuations in mood or hormonal status associated with the menstrual cycle, we limited our study to postmenopausal subjects. Eligibility criterion included self-reported postmenopausal status (no menstruation for at least 12 months), regularly engaged in recreational exercise at least 3 hours/week, as well as answering “no” to all questions on the Physical Activity Readiness Questionnaire (PAR-Q) (Chisholm et al. 1975). Twenty-four eligible women were identified and all indicated that they were interested in participating in the study. However, because of the heavy rainfall in the early afternoon of the study, five did not come to the first exercise session. Thus, nineteen enrolled in the study. There were no dropouts.
Mood states were measured using the Positive Affect Scale (PAS) and the Negative Affect Scale (NAS), a validated standard questionnaire that includes a brief list of six mood states (Diener and Emmons, 1985). Participants were instructed to consider their current feelings and to mark how happy, joyful, delighted, pleased, depressed/sad, angry, frustrated, and worried/anxious they felt on a standard six point Likert continuum scale, with 0 representing “not at all” and 6 for “extremely”. Although mood states are usually measured over longer periods of time, in a study of daily stressors, the PAS and NAS scales were used and found to be sensitive enough to detect changes in mood as measured six times a day (Hartridge et al. 1998).
A randomized crossover study design was impossible as atmospheric conditions are highly variable in May, with great daily differences in temperature and humidity. Therefore, this was a crossover study with each woman serving as her own control. All women walked outdoors on the same day (May 24, 2005).
On the days of the exercise study, subjects were asked to refrain from eating or drinking anything other than water for 3 hours prior to each exercise session. Immediately before each exercise period, a nurse practitioner qualified in adult medicine conducted a brief cardiovascular health assessment, including measuring blood pressure, pulse rate, and lung and heart sounds. The women then completed the mood questionnaire, and provided a saliva sample, following the standard salvia collection guidelines provided by Salimetrics (Salimetrics, 2004): Each subject rinsed her mouth with water and then 10 minutes later, expectorated into a 2-inch section of a plastic straw, allowing saliva to collect in a 2-mL cryo-vial. Chairs and desks were available for women as they completed the questionnaire and collected saliva samples. After each exercise session, a nurse practitioner again measured each subject's blood pressure and pulse, and then the subject answered the same brief questionnaire, and provided a second saliva sample.
Each subject walked at her own pace for one hour around the campus Horseshoe (grassy area lined with brick paths, old trees, and flowerbeds). Due to heavy rainfall, women began walking at 6:20 pm, ending by 7:20 pm. To gain some sense of walking speed, women collected a marker each time they completed a circle of the Horseshoe.
The women returned to the campus approximately a week later, again between 5:00 pm and 6:45 pm, for scheduled time slots to walk for one hour on the treadmills in the exercise lab located in the basement of the campus gym. The gym lab was located in the university gym, and provided an environment similar to that found in a commercial gym. There was a variety of exercise equipment, with similar spacing and décor. Each woman was given an opportunity to operate the treadmill and instructions were given on how to vary the speed and grade of the treadmill. Time was given for each woman to feel comfortable with its controls before beginning the exercise session. An attendant checked frequently to assess comfort of the women with the speed each choose.
In both environments, women were instructed to walk at a pace that was comfortable. Bottled water was freely available along the walking path and in the gym.
Saliva samples were stored at –80 °C until the end of the study when they were shipped to Salimetrics (State College, PA) for analysis of cortisol and alpha amylase using enzyme-immunoassay kits. Standard assay procedures were used by Salimetrics to analyze the saliva samples. Samples were measured in duplicate for salivary cortisol and averaged for use in the data analysis. Following standard Salimetrics protocol, saliva was analyzed only once for alpha-amylase.
Sound levels at the beginning and end of the exercise sessions were measured with a 7-Range Analog Display Sound Level Meter (RadioShack). Music levels in the lab were matched to that recorded in two other exercise areas of the gym. Temperature and humidity were measured using an Indoor/Outdoor Thermometer (RadioShack).
To simulate the environment of a typical gym, music typical of an exercise area in genre (hard rock) and decibel level was played for the gym session of the study but not during the outdoor walking session, again typical of the kind of exercise environment most women would experience when walking outdoors.
Statistics
Results for each variable were tested for normality (D'Agostino-Pearson test) using GraphPad Software, Inc (GraphPad Prism 5, San Diego, CA). Only alpha amylase values were non-normal, and were then log transformed for subsequent analyses. SAS PROC MIXED (SAS version 8.02, Institute Cary, NC) was used to compare the data. PROC MIXED is a robust variant of the mixed linear model that has great flexibility, allowing for correlated and nonconstant variability within the data. For our primary analyses, we fit a repeat measures mixed model, where subject was the repeated factor, and all other variables were fit as fixed effects. In addition to the variable of interest, other variables included in the model were age, race, BMI, indoor versus outdoor environment, post measures of systolic blood pressure, and pulse. Since baseline moods could be associated with many factors beyond the control of this study, an intent-to-treat approach was used for analysis, comparing only moods after exercise in the two environments.
Results
Demographic data for the 19 subjects are presented in Table 1. The average age was 58 ± 4 years. Six subjects were African American, and thirteen were European American. Generally well-educated, all had completed high school, five had some college, six had completed college, one had a completed technical training course, and six had done advanced studies. Nine of the women came from households with annual incomes totaling $60,000 or more. The mean body mass index was 26.7 ± 6. Nine of the women were within normal range (18.5 to 25), three were overweight (26–29), six were obese (BMI > 30) and one was under weight (<18.5). Nine were married, and ten were single. Thirteen of the women were on some kind of medication (hormone replacement therapy (n = 4), osteoporosis prevention (n = 5), antihypertensives (n = 5), three were being treated with cholesterol lowering drugs (n = 3). Twelve of the nineteen women took dietary supplements or multivitamin pills. Only two women took neither medications nor vitamins/dietary supplements.
Demographic characteristics and baseline health descriptions.

Environmental conditions were almost identical between the two sites. During the outdoor walk, humidity was 45% vs 46% indoors; temperature was 72 °F/22 °C outdoors vs 73 °F/23 °C indoors. The light in the exercise lab was 180 lux versus 220 lux outdoors.
There was less noise outdoors (65 decibels), and the sounds were primarily from conversations, traffic, and birdsongs, compared with 74 decibels indoors.
On average, the self-chosen speed for the outdoor exercise period was 5.1 kilometers/h (8 ± 1.3 times around a pre-set course on the campus that measured 0.6 kilometers), and 4.3 ± 0.6 kilometers/h on the treadmill. Four of the women varied (increased) their treadmill speeds during the hour. For averaging purposes, we used their final chosen speed.
Moods were affected by environment (Table 2; Fig. 1). Indoor walking was associated with higher scores for negative feelings of worry, frustration, anger, and sadness; for worry and frustration, significant changes were worry (p = 0.02; 95% CI: 0.17, 1.6); frustration (p = 0.03; 95% CI :0.12, 1.6), with lower scores for positive moods of feeling happy, delighted, joyful, and pleased; significant changes were feeling pleased (p = 0.03; 95% CI: -1.7, 0.1) and delighted (p = 0.05; 95% CI: -1.75, -0.02) Slight decreases (p < 0.07) in happiness, joy, and increased anger after walking indoors were also noted. Sadness was the least affected mood, decreasing only slightly with walking outdoors (p = 0.3). When comparing pre-post mood states, walking outdoors was associated with improved positive moods and decreased negative moods, whereas walking on the treadmill was predominantly associated with stable mood states, with only anger showing a change (increasing slightly).
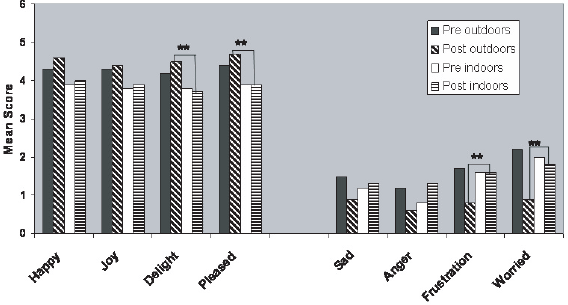
Comparision of mood score changes with indoor and outdoor exercise ** indicates p < 0.05
Changes in post exercise mood compared between indoor and outdoor environment.
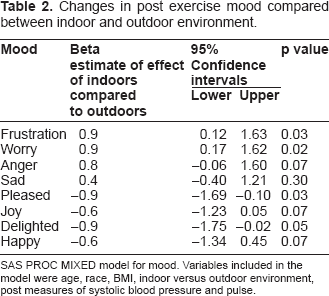
SAS PROC MIXED model for mood. Variables included in the model were age, race, BMI, indoor versus outdoor environment, post measures of systolic blood pressure and pulse.
Salivary hormone levels varied significantly with mood states (Table 3).
Significant variables contributing to post exercise stress hormone levels. Variables included in the model were moods, age, race, BMI, indoor versus outdoor environment, post measures of systolic blood pressure, and pulse.

SAS PROC MIXED model for stress hormones. Variables included in the model were mood, age, race, BMI, indoor versus outdoor environment, post measures of systolic blood pressure and pulse.
Discussion
Many physical variables differed between our two study sites. The outdoor environment offers a variety of external stimuli that can not be reproduced mechanically indoors. The campus walk was esthetically pleasing, following brick pathways lined with flowering plants and large trees, whereas the exercise lab was in a gym basement in an older campus building. Assistants directed participants to the gym lab, welcoming them. As many commercial gyms are located in warehouses and other facilities without windows, the gym lab was similar to local gyms in many parts of the U.S.
Walking indoors on the treadmill was either associated with no change from baseline to a slight worsening of mood, compared with walking outdoors, where moods improved from the baseline. Interestingly, neither frustration nor worry varied between the different environments at the two baselines, but both improved during the outdoor exercise only. Only one of the women in our study reported feeling more comfortable walking on the treadmill.
Treadmill walking was not a means for stress reduction in this group of postmenopausal women. All eight of the moods were unfavorably affected even at baseline during the indoor exercise session. The reasons for this could include feeling uncomfortable in a college gym, either because almost everyone was young, whereas the women were closer to the age of the mothers of most students. Other studies have identified gyms creating a general sense of “lycraphobia” (discomfort of the general public in the presence of highly fit exercisers in traditional gym settings) (Hillsdon and Thorogood, 1996; Peacock et al. 2007).
In a study similar to this study, Peacock reported that 20 people who walked for half an hour first outdoors along wooded paths and then a week later for the same amount of time indoors in a shopping mall experienced greater benefits from the outdoor excursion, reporting decreased anger and improved self-esteem (Peacock et al. 2007). The mood improvement experienced by our women after walking outdoors is similar to the effects reported by Wirz-Justice who found that an hour walk outdoors reduced the symptoms of seasonal affective disorder by 50% (Wirz-Justice et al. 1996). Another study of women with mild to moderate depression symptoms reported that a brisk 20-minute outdoor walk and a vitamin supplement increased women's overall mood, self-esteem, and general sense of well-being (Brown et al. 2001). However, the study did not differentiate between the effects of the walk and the vitamin supplement.
The women, almost all of whom were strangers to each other, began walking along the campus path at about the same time, and ended about the same time. The pace was self-regulated, and many women fell into conversation with other participants during the walk. In theory, this could have contributed to greater social contact and satisfaction, particularly at the second exercise period. However, although the treadmill exercise period followed the campus walk, none of the same women conversed with their neighbors while on the side by side treadmills in the exercise lab. This could have been related to the music or the unfamiliar setting of the gym. It is possible that if women were allowed to listen to music of their own choice while walking on the treadmill, they also would have improved moods. Although it is possible to bring personal audio equipment into the gym, most gyms play loud music with a heavy beat so it was a reasonable part of our simulated gym setting.
Due to overcast skies on the day of the outdoor walking exercise, light conditions did not vary between the two environments. Our study did not allow us to differentiate between natural light outside and overhead fluorescent lighting in the gym. It is possible the natural spectrum sunlight may have positively improved mood during outdoor exercise, and the effect may have been independent of brightness.
An intriguing study of breast cancer risk among Finnish women reported no risk reduction with exercise (Luoto et al. 2000). However, in a subgroup of women who commuted to work by walking or bicycling at least 30 minutes or more daily (an obligatory outdoor activity), a lower breast cancer risk (RR: 0.87) was noted. Finland is a country with low winter sunlight exposure.
Although Hartridge and colleagues found a high correlation between mood states and salivary cortisol for the 120 participants in his study, similar results were not found in the current study. However, Hartridge was interested in acute changes in cortisol throughout the day, recording mood and obtaining saliva samples six times/day during normal activity, whereas this study only compared before and after an hour of uneventful exercise.
Exercise programs commonly fail, with only about 50% of people who enroll in an exercise program continuing beyond 10 weeks (Jones et al. 2005). The most sustainable programs with the best overall results were those that favored walking without requiring participation in gym-based exercise programs (Hillsdon and Thorogood, 1996). Walking outdoors includes variable sights, sounds, and serendipitous events that are unpredictable as well as varying walking pace. However, not all outdoor walking environments have a favorable impact on mood; Pretty found that unpleasant rural and urban scenes significantly decreased the pleasure of walkers (Pretty et al. 2005).
A recent study in California found that 87% of peoples’ work, leisure and home activities take place indoors (Shimer et al. 2005). It is possible that living so much of our lives indoors is stressful in ways not yet defined. Outdoor activity may provide necessary stimulation beyond exposure to vitamin D from the sun, providing a needed break from electronic media or telecommunications. Given the abundant information on the beneficial effects of natural light, even through windows, on healing from depression, job performance, and job satisfaction (Joseph, 2006), it would not surprising that natural light would enhance the health benefits of exercise.
This study has several limitations. First, it was a pilot study, and therefore the sample size was small. The preferred walking environment by the women in our study was not ascertained before the study, so it is possible this study sampled an outdoor-biased group. In addition, we used a non-systematic recruitment process in which notices were posted on several websites, including the Columbia Master Gardeners website, the university faculty website, several nurse and nurse practitioner websites. We also invited women who indicated their willingness to be in research studies when seen for routine mammography screenings, as well as postmenopausal women from a variety of social settings, including parent teacher association events, church-sponsored events, and women walking along neighborhood streets. Although we made every effort to balance recruitment venues on the basis of women who might be equally expected to exercise indoors and outdoors, one of the women was recruited as she walked and none of the women were recruited from a private gym. A slight bias may have arisen by not specifically inviting women who exercised indoors in private gyms, but the effect would be minimal on the study results. To better understand pre-existing personal bias, future studies should include questions regarding preferred exercise location.
The effects of weather conditions on mood are problematic. The difficulty of comparing mood during exercise done in sunny compared to overcast conditions seemed greater than the problems of comparing sequential outdoor and then indoor exercise sessions, although the effects of knowing the study procedures could have influenced some women. Alternatively, the influence of being part of a group during the first outdoor walking session, compared to being one of four women using the four treadmills in the gym, could have created a sense of disappointment during the second exercise session. However, none of the women normally exercised as part of a group, so it would not be expected that walking side by side with another participant on treadmills would be a reason for disappointment. In addition, we gave the incentive gift card at the end of the indoor exercise session, which might have influenced women and provided a reason for improved mood. Since this is not what we observed, possibly the neutral effects of the indoor environment on mood would have been more negative without the incentive cards. A replication of this study with a larger sample size in a geographic location with less variable weather would allow a randomized crossover design that could answer some of these questions.
This was a small pilot study with nineteen women exercising only once in each environment, but it would also be typical of what a postmenopausal woman might experience when beginning a fitness program. In a recent study of exercise and quality of life among breast cancer survivors found that only 31% of the women met physical activity guidelines for 60 minutes of strenuous activity or 150 minutes of moderate to strenuous activity per week (Milne et al. 2007). Enjoyment of exercise and long-term adherence are essential elements of any wellness program. The improved moods that were associated with outdoor walking, in particular decreased worry and frustration, could make the difference between a successful fitness program and an unsuccessful one. In turn, continued participation in exercise programs reduces such known risk factors for breast cancer as sex steroid hormone levels and obesity, which in turn, may directly influence breast cancer risk and survival. For healthy women, increased exercise may decrease breast cancer risk; for breast cancer survivors, increased physical activity may be associated with increased longevity and decreased health care costs related to breast cancer recurrence and depression. If the results of this study are replicated in other settings, it may help inform clinicians about the importance of exercise settings that will encourage physical activity among postmenopausal women. Physician recommendations for exercise could include gym and non-gym based exercise options.
The benefits of exercise may well encompass more than the “bodily movement produced by skeletal muscles that results in energy expenditure” (Caspersen et al. 1985), and optimal environments for bodily movement need to be described. Future studies of physical activity should include a description of the exercise environment, the pleasantness of the landscape, and if done inside, the availability of natural light.
Footnotes
Acknowledgements
This research was supported by the Department of Defense Concept Award DAMD17-00-1-0659 and Mary Curran at Salimetrics L.L.C. who performed the immunoassays. Mindy Holland assisted in project organization, Girl Scouts of Troop 1401 offered water to the participants, and Dr. Shawn Youngstedt provided the light readings.