
Abstract
Introduction
The purpose of the present retrospective study was to review outcome and patterns of failure of patients who were treated with radiotherapy for cervical lymph node metastases from an unknown primary site (CUP).
Patients and Methods
Between 2000 and 2009, 34 patients diagnosed with squamous cell CUP were admitted to radiotherapy in curative intent. In 26 of 34 patients (76%) neck dissection was performed prior to radiotherapy, extracapsular extension (ECE) was seen in 20 of 34 patients (59%). Target volumes included the bilateral neck and panpharyngeal mucosa. Concomitant chemotherapy was applied in 14 of 34 patients (41%).
Results
After a median follow-up of 45 months for the entire group, 2 of 34 patients (6%) presented with an isolated regional recurrence, another 2 of 34 patients (6%) developed both local and distant recurrence, and 6 of 34 patients (18%) had distant failure only. Estimated overall survival after 2- and 5 -years was 78% and 63%. All patients with N1 or N2a disease (n=6) were disease free after 5 years. ECE, concomitant chemotherapy and involvement of neck levels 4 and 5 were associated with worse overall survival on univariate analysis.
Conclusion
Radiotherapy of the panpharynx and bilateral neck leads to excellent local control while distant metastases are the most frequent site of failure and prognostically limiting. Therefore intensified concomitant or sequential systemic therapies should be evaluated in future trials.
Introduction
In approximately 3% of all squamous cell carcinomas metastatic to cervical lymph nodes, a primary site cannot be identified despite extensive diagnostic workup. 1 With the introduction of 18 F-fluorodeoxyglucose positron emission tomography (FDG-PET-CT) a primary tumor can be found in up to 25% of cases when standard workup with physical examination, cross-sectional imaging, tonsillectomy, and panendoscopy with blind biopsies are not able to detect a primary site.2,3 Assuming that the occult primary site is located in pharyngeal axis, most patients are treated by radiotherapy, either alone or in combination with up-front or subsequent neck dissection.
In the absence of randomized trials, however, neither the optimal treatment sequence nor the appropriate target volumes are clearly defined for this group of patients. Current treatment strategies are based on experience derived from retrospective data. Major controversies exist regarding the required extent of radiotherapy. While some authors advocate radiotherapy to the involved neck only, others propose bilateral treatment of the neck with inclusion of the panpharyngeal axis (comprehensive radiotherapy) in order to eradicate potential occult primary tumors.4,5 In early nodal stages (N1 and N2a), in the absense of risk factors such as extracapsular extension, neck dissection alone without adjuvant radiotherapy might be sufficient. 6
In the present study we report our experience with comprehensive radiotherapy, which was routinely applied at our institution for patients with cervical squamous cell cancer of an unknown primary site (CUP). Our goals were to assess survival, patterns of failure, treatment related toxicity and prognostic factors. Furthermore, we investigated the role of concomitant chemotherapy with radiotherapy.
Patients and Methods
The local ethics committee waived the requirement for written informed consent in this retrospective trial.
Between 2000 and 2009 a total of 34 patients were treated with radiotherapy for cervical lymph-node metastasis from an unknown primary squamous cell tumor. The diagnosis has been pathologically confirmed by fine-needle biopsy in 16 cases (47%), lymph-node excision in 7 cases (21%) and neck dissection in 11 cases (32%). Extracapsular extension (ECE) was diagnosed by pathological examination or by imaging studies in 20 patients (59%). Signs of ECE on imaging studies included infiltration of adjacent structures. For detailed information about patient and tumor characteristics, see Table 1.
Patients’ and tumor characteristics.

Staging included contrast-enhanced CT or MRI scans and panendoscopy with several blind biopsies in all cases. 27 of 34 patients (79%) had bilateral tonsillectomy and 2 patients (6%) had unilateral tonsillectomy. The remaining 5 patients already had tonsillectomy prior to the diagnosis of CUP. All patients had cross-sectional imaging of the chest and 18 patients (53%) additional PET scans. Lymph node metastases were classified to be of unknown primary if the primary site could not be detected despite an extensive diagnostic work-up.
28 out of 34 patients (82%) underwent up-front neck dissection prior to radiotherapy. 2 of these 28 patients (7%) still had evidence of a gross tumor at the beginning of radiotherapy and 5 of 26 patients (18%) had positive margins on pathological evaluation.
The remaining 6 patients (18%) did not undergo up-front neck dissection and were treated with definitive combined radiochemotherapy. Neck dissection was omitted in these patients because of suspected carotid artery infiltration on imaging studies.
Radiotherapy and Chemotherapy
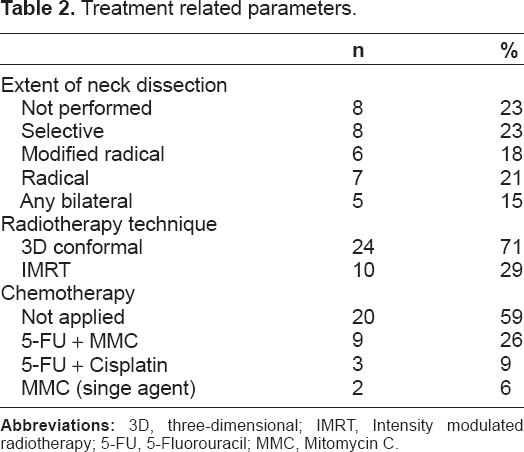
Radiotherapy was performed as conventional 3 -dimensional radiotherapy until 2007 (n = 24) and as intensity-modulated radiotherapy (IMRT) (n = 10) thereafter. The panpharynx (including the larynx and epipharynx) and bilateral neck were treated with single doses of 1.8–2.0 Gy to a median of 50 Gy (range 48.8 Gy–54 Gy), whereas areas with macroscopic disease were treated with 70–72 Gy. The median dose for areas previously harboring a lymph node was 60 Gy to 64 Gy, depending on the presence of extracapsular extension and resection status. The concurrent application of chemotherapy was considered for all patients with macroscopic disease at radiotherapy or in the presence of positive margins after neck dissection and ECE. In total, 14 of 34 patients (41%) received chemotherapy. 3 different chemotherapy protocols were applied. 9 patients received 5-flurouracil (600 mg/m2 of body surface area) as a continuous infusion for 120 hours during the first week of radiotherapy plus mitomycin C (10 mg/m2) on days 5 and 36 of treatment. 3 patients received 5-flurouracil (600 mg/m2) as describe above plus daily cisplatin (20 mg/m2) during the first and fifth week of treatment. 2 patients received single agent mitomycin C (10 mg/m2) on days 5 and 36 of treatment. Chemotherapy was omitted in 7 patients with ECE because of associated comorbidities. In general, patients with macroscopic disease received 5-flurouracil and/or mitomycin C, while platinum was administered to patients without residual gross tumor but with ECE or positive margins after neck dissection.
Treatment-related parameters are summarized in Table 2.
Treatment related parameters.
Patients were seen for first follow-up 6 weeks after the completion of radiotherapy. Follow-up included cross-sectional contrast enhanced imaging of the neck and flexible nasopharyngoscopy. On first follow-up, the need for surgical resection of persistent lymph nodes after radiotherapy was discussed. Follow-up was continued on a regular basis for 5 years.
Acute and late treatment related toxicity was graded according to the RTOG/EORTC toxicity criteria. 7 Statistical analysis was performed with commercial software (SPSS 19, IBM Inc., Armonk, NY, USA). Overall survival (OS), disease-free survival (DFS), distant-failure-free survival (DFFS) and local control (LC) rates were calculated from the day of diagnosis, using the Kaplan-Meier method. Differences between curves were evaluated by the 2-tailed log-rank test. Significant results (P < 0.05) were included in a multivariate analysis (Cox regression model). The Chi-square test was used to compare the frequency of toxicities within subgroups.
Results
Treatment Compliance and Toxicity
All but 1 patients completed radiotherapy and chemotherapy as prescribed. This 1 patient refused the last fraction of radiotherapy. No patient experienced grade IV toxicity of any kind. 9 of 34 patients (26%) required placement of a percutaneous endoscopic gastrostomy feeding-tube (PEG) during treatment because of grade III dysphagia. Acute grade III dysphagia was significantly more frequent in patients who received concomitant chemotherapy (54% vs. 11%, P = 0.03).
44% of patients reported grade II xerostomia on follow-up. With regard to late toxicity, no significant difference between patients who received chemotherapy or those who did not was observed.
Acute and late toxicity did not differ significantly between patients who were treated with IMRT or conventional 3-dimensional radiotherapy.
Table 3 provides detailed information about acute and late treatment related toxicity.
Acute and late treatment related toxicity.

Treatment Outcomes
At the time of evaluation, 13 of 34 (38%) patients had died. Median follow-up for patients alive was 67 months (range 13–131 months).
Local Control and Patterns of Recurrence
2- and 5-year estimated LC rates were 94% and 88% respectively.
At first follow-up, 2 patients had residual cervical lymph nodes on CT imaging. Both patients received salvage neck dissection. One of these 2 patients was disease-free until he died of sepsis and renal failure 3 years later. The other patient unexpectedly died at a rehabilitation facility 3 months after successful salvage surgery. These 2 cases were not considered as treatment failure.
2 of 34 patients (6%) developed ipsilateral lymph node recurrences. 1 of these was located in level 5, 6 months after radiotherapy. Due to synchronous pulmonary metastases, he received systemic treatment without local salvage therapy. The other patient had ipsilateral recurrence in level 2, 9 months after radiotherapy. This patient was treated according to a re-irradation protocol described elsewhere. 8 Both patients died of progressive disease.
Mucosal tumors and therefore the putative primary tumor emerged in another 2 of 34 patients (6%). 1 was seen at the base of the tongue (3 years after treatment) and 1 at the floor of the mouth (seven years after treatment). In the first case treatment was limited to best supportive care; the second patient had repeated salvage surgeries. Both patients died of the disease.
All 4 patients with nodal or mucosal recurrences had at least N2b disease on initial presentation. All local recurrences were located in field within radiotherapy volumes, which were covered by doses of at least 50 Gy.
2- and 5-year distant failure-free survival was 72% and 61%. A total of 8 patients developed distant failure, predominantly in the lung (5 of 8 patients, 63%). In 1 case, the pulmonary lesion was solitary and presented as a Pancoast tumor. On initial diagnosis, level 4 was affected in this patient. 7 of 8 patients with distant failure (88%) initially presented with ECE and N2b or a higher nodal stage. At the time of evaluation, all patients diagnosed with distant failure had died. Median survival after the diagnosis of distant metastases was 5 months (range 1–52 months).
Overall Survival and Disease Free Survival
2-year and 5-year estimates of overall survival were 78% and 63% respectively. 2-year and 5-year estimates of disease-free survival were 70% and 61%.
Prognostic Factors
The impact of following potential prognostic factors on OS, DFS, DMFS and LC was evaluated: ECE, extent of nodal disease (N1 and N2a vs. N2b and higher), involvement of lymph node levels IV and V and resection status (R1 vs. R0), Furthermore, the influence of concomitant chemotherapy on the endpoints described above was investigated.
On univariate analysis the presence of ECE was associated with significantly shorter OS, although 13/20 patients (65%) with ECE received intensified treatment with concomitant chemotherapy (5-year OS 92% vs. 44%, P = 0.004).
After 5 years, 100% of patients with N1 or N2a disease were alive and disease-free, whereas patients with an extensive nodal involvement (N2b/N3) exhibited a trend towards inferior prognosis in term of OS, DMFS, DFS and LC. Their estimated rates for OS, DMFS, DFS and LC survival after 5 years were 57% (P = 0.11), 54% (P = 0.08), 55% (P = 0.07) and 85% (P = 0.34) respectively.
Patient with lymph node metastases in level IV or V had a significantly shorter 5-year OS (74% vs. 42%, P = 0.019), DMFS (75% vs. 38%, P = 0.023) and DFS (76% vs. 38%, P = 0.05). For the whole cohort the concomitant use of chemotherapy was associated with a significantly worse OS (83% vs. 34% at 5 years, P = 0.019), DMFS (80% vs. 37% at 5 years, P = 0.04), Figure 1. However, within the prognostically unfavorable subgroup of patients with ECE, no difference between patients who received chemotherapy (13 of 20 patients) or not (7 of 20 patients) was observed (5-year OS 28% vs. 27%, P = 0.352; 5-year DMFS 31% vs. 57%, P = 0.61).

Overall survival for patients (
Resection status did not affect any of the endpoints. In a multivariate analysis including ECE, involvement of level 4 or 5 and chemotherapy, an independent prognostic factor for OS, DFS, DMFS or LC could not be identified.
Discussion
In this retrospective single institution study of 34 CUP patients, a comprehensive approach including radiotherapy of the bilateral neck and the panpharynx led to an excellent local control rate of 88% after 5 years. The estimated OS after 5 years was 63%. Both values are at least in line with or even superior to other published data.9–11
However, the optimal treatment for cervical CUP patients is still a matter of debate. In the absence of prospective data, treatment recommendations are based on retrospective data until now. Most approaches favor neck dissection followed by postoperative radiotherapy whenever surgery is feasible and may achieve at least R1 resection. But both the issue of adequate radiation portals and the application of concomitant chemotherapy in high-risk cases is a matter of debate. Currently, no reliable data is available showing that bilateral radiotherapy is superior to unilateral irradiation in patients with unilateral nodal involvement.12–14
In the largest study of CUP patients published so far, Grau et al report a 54% rate of emerging primaries after 5 years for patients treated with surgery alone without radiotherapy. In that study, both ipsilateral and comprehensive radiotherapy significantly lowered the incidence of primary mucosal tumors. However, there was no significant difference between radiotherapy approaches. 14
On the other hand, the idea that a more extensive radiotherapy approach might lower the risk for the emergence of primary mucosal tumors is supported by retrospective trials showing increased numbers of primary tumors developing in unirradiated mucosal sites.4,12 Yet despite significant improvements in radiotherapy techniques, treatment-related toxicity remains considerable and the potential benefits of more extensive radiotherapy might be outweighed by increased toxicity.15–17 Unfortunately, the only prospective study to randomize CUP patients to either comprehensive radiotherapy or unilateral radiotherapy of the neck was closed early because of slow accrual (EORTC 24001–22005).
As mentioned above, we observed local control and survival rates comparable to previous studies despite a high number of patients with advanced nodal disease. This might be interpreted as an argument for a comprehensive radiotherapy approach in patients with advanced features such as ECE and N2b or higher nodal stage.
On the other hand, a subgroup of patients that might be considered for a less comprehensive approach are patients with limited nodal disease. In our study, disease free survival for patients with N1 and N2a disease was of 100% after 5 years. In comparison, Coster et al observed an 89% local and distant control rate after surgery alone for patients with N1 disease without ECE. 18 Similarly, Fakhrian et al report only one local recurrence in 17 patients with N1-N2b disease treated with ipsilateral radiotherapy of the neck after surgery. 9
The limiting factor for survival in our study was not local but distant control with 8 of 34 patients (24%) presenting with distant metastases during follow-up. Both the frequency of distant failure and the identification of ECE and lymph node metastases in levels IV and V as the predominant predictors for distant failure are in line with previous trials.9,11,19 Lymph node metastases in levels IV or V are known to be associated with a poor prognosis due to their potential origin from infraclavicular sites, such as the lung or esophagus.20,21 In our study, 1 patient presented with a Pancoast tumor during follow-up, which can be interpreted as a demasking primary tumor below the clavicles.
Combined treatment of radiotherapy and chemotherapy improves survival for head and neck cancers in the primary setting or in high-risk adjuvant constellations. This benefit is mainly due to an increase of local control. None of the randomized landmark trials comparing radiotherapy with radiochemotherapy for head and neck cancers could detect a significant impact on distant metastases.22–24 In our trial, patients who received synchronous chemotherapy showed significantly worse OS and DMFS, confirming previous observations.25,26 At the same time, the addition of chemotherapy was associated with significant toxicity. The negative impact of chemotherapy on OS is likely to be reflecting a selection bias, as patients with risk factors like ECE, positive margins or advanced nodal disease are more likely to receive chemotherapy.
The presence of significant results in the univariate but not in the multivariate analyses is likely to be explained by the relatively low number of patients in each group. The low number of patients might as well explain the low difference of long term toxicities between patients treated with IMRT and conventional radiotherapy. Previous authors have reported very favorable long-term toxicity outcomes with the use of IMRT.10,27
In summary, we were able to show excellent local control for CUP patients treated with a comprehensive radiotherapy approach. This may indicate that radiotherapy of the panpharynx and bilateral lymphatic drain is justified at least for patients with high risk factors such as advanced nodal disease (N2b or higher), ECE, or close surgical margins. Distant failure is prognostically limiting, particularly for patients with ECE. Therefore, the intensification of the systemic component for selected CUP patients should be evaluated in the future.
Author Contributions
Conceived and designed the experiments: CG, MW. Analyzed the data: CG, MB, FE, MW. Wrote the first draft of the manuscript: CG, MW, JT, PSM, FE, ACM. Contributed to the writing of the manuscript: CG, MB, JT, PSM, ACM. Agree with manuscript results and conclusions: CG, FE, ACM, JT, PSM, MB, MW. Jointly developed the structure and arguments for the paper: CG, FE, ACM, JT, PSM, MB, MW. Made critical revisions and approved final version: CG, FE, ACM, JT, PSM, MB, MW. All authors reviewed and approved of the final manuscript.
Funding
We acknowledge support by Deutsche Forschungsgemeinschaft and Open Access Publishing Fund of Tuebingen University.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.