
Abstract
Background
The essential factor for diagnosis and treatment of diseases in head and neck endoscopy is the visibility of the image. An anti-fogging agent can reduce this problem by minimizing surface tension to prevent the condensation of water in the form of small droplets on a surface. There is no report on the use of hibiscrub® or baby shampoo to reduce fogging in the literature. The objective of this study was to compare the efficacy between commercial anti-fogging agent, hibiscrub® and baby shampoo to reduce fogging for the use in head and neck endoscopy.
Methods
The study was conducted at the Department of Otorhinolaryngology, Faculty of Medicine, Khon Kaen University in August 2010. Commercial anti-fogging agent, baby shampoo and hibiscrub® were applied on rigid endoscope lens before putting them into a mist generator. The images were taken at baseline, 15 seconds, 30 seconds and 1 minute. The images' identifiers were removed before they were sent to two evaluators. A visual analogue scale (VAS) was used to rate the image quality from 0 to 10.
Results
The difference in mean VAS score between anti-fogging agent, baby shampoo and hibiscrub® versus no agent were 5.46, 4.45 and 2.1 respectively. The commercial anti-fogging agent and baby shampoo had most protective benefit and performed significantly better than no agent (P < 0.05).
Conclusions
Baby shampoo is an effective agent to prevent fogging during head and neck endoscopy and compares favourably with commercial anti-fogging agent.
Background
One of the important considerations when using an endoscope to aid diagnosis and treatment of diseases in head and neck is the quality of the image. When the endoscope is entering the upper airway cavity fogging usually occurs. Most accepted theories state that lens fogging occurs when there is an imbalance between the temperature of the front lens, temperature of the airway cavity1,2 and humid relatively to the environment. 3 Anti-fogging agents can reduce this problem by minimizing surface tension to prevent the condensation of water in the form of small droplets on the tip surface of the lens. The commercial anti-fogging agents are composed of surfactant, alcohol and water. 4 On this basis, any agent that contains surfactant may reduce fogging.
In our institute we usually use the hibiscrub® or baby shampoo as alternatives to the commercial anti-fogging agent. Hibiscrub® ingredients are polyoxyethylene-polyoxypropylene block copolymer, lauryl dimethyl amine oxide, glycerol, macrogol 7 glycerol cocoate, ponceau 4R (E124), isopropyl alcohol, herbacol 015393 TB, D-gluconolactone, sodium hydroxide. Baby shampoo ingredients are cocamidopropyl betaine, PEG-80 sorbitan laurate, sodium trideceth sulfate, PEG-150 distearate, fragrance, polyquaternium-10, tetrasodium EDTA, quaternium-15. Both agents have surfactant and moisturiser as the active ingredients.
There have been some reports on the prevention of lens fogging during endoscopy. Mohammadhosseini 5 reported the use of povidine scrub rubbing on the lens surface which can prevent the fogging for several minutes. Fraser 6 reported the use of patients' saliva to prevent the fogging during fiberoptic nasolaryngoscopy. There are, however, no reports on hibiscrub® or baby shampoo to reduce fogging in the literatures. However baby shampoo which has antiseptic properties 7 and does not produce mucosal irritation. 8 It has been used in patients with chronic rhinosinusitis and there have been no reports of major side-effects. 9 The objective of this study was to compared the efficacy of commercial anti-fogging agent, hibiscrub® and baby shampoo to reduce fogging during head and neck endoscopy.
Methods
The study was conducted at the Department of Otorhinolaryngology, Faculty of Medicine, Khon Kaen University in August 2010. Commercial anti-fogging agent (Ultrastop®), 4% chlorhexidine detergent solution (Hibiscrub®) and baby shampoo (Johnson's® No More Tears®) were applied to cotton wool and rubbed onto the Karl Stoz® rigid endoscope lens before approach to a mist generator which produces consistent condensation. The room temperature was set to 25 °C. The distance between the tip of the endoscope and the image was 3 centimetre during each session.
The images was photographed using Toshiba® 3CCD IK-TF5 camera at baseline, 15 seconds, 30 seconds and 1 minute. The images' identifiers were removed before they were sent to two evaluators who were therefore blinded. A visual analogue scale (VAS) was used to rate the image from 0 (clearest) to 10 (the worst).
Statistical analyses were conducted using Stata (version 10, StataCorp LP, Texas, USA). The mean score at each time point was calculated. The protective effects between agents were analysed using the unpaired t-test for continuous variable. For all tests, P < 0.05 was considered statistically significant.
Results
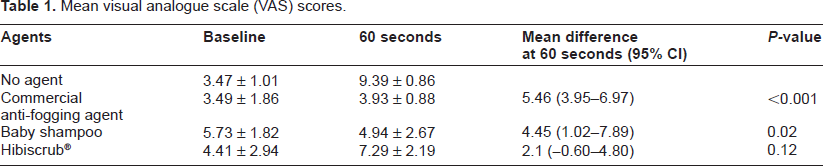
In the no agent group, the baseline score was 3.47 and gradually increased to 9.39 at 60 seconds. In the other groups, baseline score were ranged from 3.49 to 5.73 and increased to 3.93 to 7.29 at 60 seconds. Commercial anti-fogging agent received the best score at all points. The difference in mean VAS scores at 60 seconds between anti-fogging agent, baby shampoo and hibiscrub® versus no agent were 5.46, 4.45 and 2.1 respectively (Table 1). The commercial anti-fogging agent and baby shampoo had the most protective benefit and were significantly better than no agent (P < 0.05). The graphs of mean VAS score at each time point were shown in Figure 1.
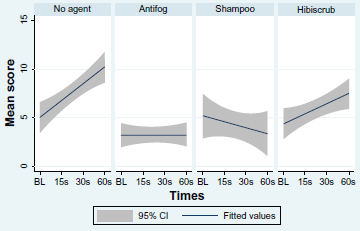
Graph of mean VAS score between agents at baseline, 15, 30 and 60 seconds with 95% confidence interval. Baby shampoo scores are most similar to commercial anti-fogging agent.
Mean visual analogue scale (VAS) scores.
Discussion
The major factors that affect the visibility during endoscopy are fogging, fluids and tissues passively encountered in the operative field (eg, blood, discharge) and the reaction of tissue to accidental or intentional injury (eg, smoke and eschar with thermal injury from diathermy).3,10 Anti-fogging agents are essential during head and neck endoscopy to eliminate one of these major problems.
In western countries, fogging in endoscopy is no longer a problem for otolaryngologist. Due to our limited resources, we try to find alternative agents that have preventing effect similarly to commercial agents. In our experience, baby shampoo and hibiscrub® are effective but there is no evidence of these agents in the literature. We designed the single blinded randomized controlled experimental study to compare the efficacy of baby shampoo and hibiscrub® versus commercial antifogging agent.
We found that commercial anti-fogging agent still provides the best image quality. Baby shampoo also has a protective effect which is significantly better than no agent. Our baseline scores of hibiscrub® and baby shampoo were slightly high perhaps owing to its' colour (pink and yellow respectively) and viscosity. Baby shampoo showed the largest standard deviation (SD) at baseline and 60 seconds indicating that there are the variations in different images for baby shampoo.
This in-vitro data will be used as the reference for the clinical study. We are planning to conduct the clinical trials comparing baby shampoo versus commercial anti-fogging agent to evaluate the effectiveness of baby shampoo in clinical practice.
Conclusions
Baby shampoo is an effective agent to prevent fogging during head and neck endoscopy and compares favourably with commercial anti-fogging agent.
Authors' Contributions
PP was a major contributor to the study. PK rated the score and wrote the discussion section. ST rated the score, and revised the manuscript. All authors read and approved the final manuscript.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgements
The authors thank the Faculty of Medicine, Khon Kaen University for the research grant. We appreciate the assistance received from Prof Robert Peter Mills in the editing of the manuscript.