
Abstract
Background
Surgical approaches to the jugular foramen are often complex and lengthy procedures associated with significant morbidity based on the anatomic and tumor characteristics. In addition to the risk of intra-operative hemorrhage from vascular tumors, lower cranial nerves deficits are frequently increased after intra-operative manipulation. Accordingly, modifications in the surgical techniques have been developed to minimize these risks. Preoperative embolization and intra-operative ligation of the external carotid artery have decreased the intraoperative blood loss. Accurate identification and exposure of the cranial nerves extracranially allows for their preservation during tumor resection. The modification of facial nerve mobilization provides widened infratemporal exposure with less postoperative facial weakness. The ideal approach should enable complete, one stage tumor resection with excellent infratemporal and posterior fossa exposure and would not aggravate or cause neurologic deficit. The aim of this study is to present our experience in handling jugular foramen lesions (mainly glomus jugulare) without the need for anterior facial nerve transposition.
Methods
In this series we present our experience in Kasr ElEini University hospital (Cairo–-Egypt) in handling 36 patients with jugular foramen lesions over a period of 20 years where the previously mentioned preoperative and operative rules were followed. The clinical status, operative technique and postoperative care and outcome are detailed and analyzed in relation to the outcome.
Results
Complete cure without complications was achieved in four cases of congenital cholesteatoma and four cases with class B glomus. In advanced cases of glomus jugulare (28 patients) (C and D stages) complete cure was achieved in 21 of them (75%). The operative complications were also related to this group of 28 patients, in the form of facial paralysis in 20 of them (55.6%) and symptomatic vagal paralysis in 18 of them (50%).
Conclusions
Total anterior rerouting of the facial nerve carries a high risk of facial paralysis. So it should be reserved for cases where the lesion extends beyond the vertical ICA. Otherwise, for less extensive lesions and less aggressive pathologies, less aggressive approaches could be adopted with less hazards.
Background
One of the most challenging problems for the otolaryngologist and the neurosurgeon is the treatment of large neoplasms involving the skull base and the inferolateral temporal bone. The intimate relationship of these tumors with the internal carotid artery and the dural venous sinuses might expose the patient to severe and life threatening intraoperative hemorrhage. The presence of the facial nerve in the middle of the operative field is responsible for technical difficulties in handling and achieving complete removal of the tumor and in controlling the bleeding without injuring the nerve. The intimate relation to the lower four cranial nerves might be responsible for postoperative handicapping functional problems as regarding the laryngeal competence. 1
Congenital cholesteatoma (CC 1 ) is thought to occur secondary to failure of normal involution of epidermoid formation within the middle ear cleft. 2
Glomus jugulare tumors are benign lesions located in the jugular foramen and may extend into the middle ear, petrous apex and upper neck and may invade intradurally. Their surgical management is a challenge to both neurosurgeons and skull base surgeons. Despite the advancement in non-surgical techniques the only treatment with proven efficacy is radical surgical removal. 3
Rosenwasser was the first to attempt radical surgical removal of the tumor. 4 Capps was the first author to perform anterior transposition of the facial nerve, occlusion of the sigmoid and ligature of the internal jugular vein in the neck in 1952. 5 Twenty six years later Fisch restored this approach giving a detailed description of what he called a type A approach for jugular foramen lesions and adding two more approaches (namely types B and C approaches) for more anteriorly situated lesions. The key elements in the Fisch type A approach, designed for glomus jugulare type C (according to Fisch classification) were anterior rerouting of the facial nerve and the permanent obliteration of the middle ear space.6,7 Despite the meticulous dissection, anterior facial nerve rerouting is frequently followed by transitory weakness postoperatively. 8
The facial nerve is supplied through three main arterial systems (from the labyrinthine, the middle meningeal, and the stylomastoid arteries). 9
Transposition requires skeletonization of the FN 2 in the fallopian canal, resection of attachments to the canal, and displacement of the FN in an anterior or posterior direction. Extrinsic and intrinsic blood supply are placed in jeopardy, especially with first genu rerouting. However, rerouting of the FN provides maximal jugular bulb and tumor exposure and facilitates tumor resection. 10
During the last decades several article have been addressed to discuss glomus jugulare tumors, however few of them put into question the real need to anteriorly transpose the facial nerve as a prerequisite for proper surgical removal of such tumor.
The aim of this retrospective study is to present our experience in handling jugular foramen lesions (mainly glomus jugulare) without the need for anterior facial nerve transposition.
Methods
This is a retrospective review of 36 patients, 23 females (63.9%) and 13 males (36.1%), 28 cases of glomus jugulare tumors classes C and D, 4 cases of glomus jugulare tumors Class B according to Fisch classification system, and 4 cases of congenital cholesteatoma of ME, surgically treated in Kasr ElEini University Hospital in Cairo, Egypt, from 1988 to 2008. Age range was 22 to 65 years (mean age 49 years).
Preoperative assessment
Included full clinical history taking and clinical examination of the patients as well as preoperative audiological evaluation by pure tone audiogram. Radiological evaluation included, contrast enhanced high resolution CT scan (HRCT 3 ) and/or MRI with gadolinium for the skull base and the posterior cranial fossa. Routine preoperative 4 vessels angiography and embolization of the feeding external carotid vessels, was done 48 hours prior to the preplanned surgery.
Staging
The Fisch classification system was adopted to classify the glomus jugulare cases. 11
Operative
The four congenital Cholesteatoma cases were treated by retrofacial approach according to Jackson et al. 12
The basic steps of the retrofacial approach (modified) in our practice were the following:
A regular post-auricular skin incision (the original Y-shaped parotidectomy-like incision was not adopted by our team seen not necessary) extending down to greater cornu of hyoid then the facial nerve was identified in the parotid. A cortical mastoidectomy was done followed by dissection of the facial recess that is then extended inferiorly till the meso and hypotympanum after cutting the chorda tympani. The sinus tympani was then opened. The drum and middle ear structures were removed except the stapes and its tendon. Then the postero-superior canal wall, mastoid tip and all bone lateral and anterior to jugular foramen and the bone covering the jugular bulb were all removed. The sternomastoid and digastric muscles were separated from mastoid tip. The cervical soft tissue component of the approach including vascular and neural components was not included in our approach since the cholesteatoma is non-vascular, non-adherent and readily resectable lesion macking this component of the approach unnecessary. The congenital cholesteatoma was then removed. The radical cavity was packed and the wound was closed in anatomical planes.
Three of the four glomus jugulare type B cases were treated by partial anterior rerouting technique according to Jackson. 13
The basic steps of the partial anterior rerouting technique in our practice were:
Previous steps as in retrofacial approach are repeated in addition to:
The vertical mastoid segment of the facial nerve is liberated and partially rerouted anteriorly pivoted at the 2nd genu, giving larger space to handle the vertical infra-labyrinthine ICA and the jugular bulb with the related tumor. Also the cervical soft tissue component previously not included in the retrofacial approach was performed in this approach including identification of the great vessels and last 4 cranial nerves, and the ECA 4 and ascending pharyngeal artery were both ligated. The Eustachian tube (ET 5 ) as well as the exteranal auditory canal (EAC 6 ) are all handled the same way as in the classic Fisch A approach (ie, middle ear ossicles removal except the stapes, ET block and closure of the EAC as blind ended pouch). The wound is closed in anatomical planes.
One case of glomus jugulare class B (according to Fisch classification) was treated by a combined extended recess and hypotympanotomy together with mobilization of the facial nerve at the stylomastoid foramen. This approach is actually a mixture of the extended recess described by McCabe et al 14 and the post-aural hypotympanotomy described by Farrior 15 and is not very much different from the trans-mastoid infralabyrinthine approach described by Gjuric M and Bilic M. 16
Its basic features are the same as in the previous approach with two differences:
The facial nerve was only freed at the stylomastoid foramen till below the chorda tympani but without mobilization of the whole vertical segment of the facial nerve. This was done through bone removal around the facial nerve till the level of chorda tympani only. The second difference is that the middle ear structures were not disturbed as well as the external auditory canal and the Eustachian tube.
The twenty eight glomus jugulare types C or D were treated by Fisch type A approach. The basic features of infratemporal fossa type A approach in our hands were identical to the literature.6,7 The main differences between our practice and the literature is that the sigmoid sinus is not ligated but packed from outside by surgicel and the IJV ligature in the neck is delayed as much as possible to avoid tumor congestion and bleeding.
Postoperative care
In the early post-operative period, all Fisch A cases were admitted to surgical ICU for 48 hours and all patients received intra and post-operative routine medical treatment in the form of IV 3rd generation cephalosporins, antacids, analgesics and steroids. Clinical post-operative care concentrated on the vagus nerve function, the healing process, monitoring of any wound infection or CSF 7 leak and the facial nerve function. A routine immediate tracheotomy operation was done and a NGT 8 was applied for all the 28 cases with Fisch A approach ie, C and D glomus jugulare cases. Then the vagus nerve function was evaluated after two days of full recovery. If the nerve function was found to be normal, the NGT and tracheotomy were eliminated. But if the vagal paralysis was symptomatic in the form of marked dysphonia and aspiration, the patient was provided with a tracheotomy tube with a speaking valve which was kept in place for three months to give a chance for spontaneous recovery and thereafter, if persistent symptoms, a type 1 thyroplasty medialization procedure was suggested. In case the paralysis was non-problematic for the patient, nothing further was done in relation to this aspect.
In relation to the facial nerve, in case of nerve sacriice due to tumor iniltration, a greater auricular immediate cable graft was done as well as a gold implant of the upper eye lid later. In case post-operative complete paralysis with preserved anatomical integrity, gold implant was done for ocular protection and the patient was given a chance of 6 months for recovery. If no recovery at all, the patient was offered XII-VII anastomosis.
In general, patients were followed for 6 months to 2 years period, clinically for recurrence, hearing (post-operative PTA 9 was done), swallowing, dysphonia and facial nerve function. Radiologically, CT and/or MRI with gadolinium, were performed for patients to detect recurrence at three and six months from surgery. If found to be free, the patients were considered cured, but if recurrence occurred the patients were referred for radiotherapy (this is because all our recurrences/residues were due to irresectable ICA 10 infiltrations at the time of surgery).
Results
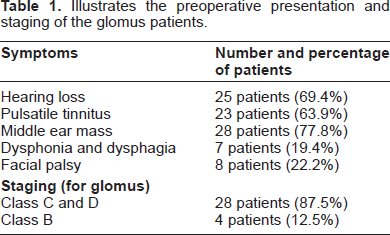
Thirty two cases of glomus (28 C and D and 4 B cases) (according to Fisch and Oldering classification system) and four cases of congenital tympanic and hypotympanic cholesteatoma (see Table 1) were operated in Kasr El Eini University hospital (Cairo–-Egypt) in the period from 1988 to 2008 with an overall complete resection rate of 80%. Table 2 illustrates the detailed resection rate in relation to each pathology and disease stage. The presenting features for all cases of congenital cholesteatoma were conductive hearing loss and middle ear mass. While the presenting features for glomus were–-in descending order of frequency: middle ear mass, hearing loss, pulsatile tinnitus, facial paralysis and finally vagal paralysis. Table 1 illustrates the presenting features for glomus cases.
Illustrates the preoperative presentation and staging of the glomus patients.
Illustrates the outcome of the operated patients in relation to the tumor resection.
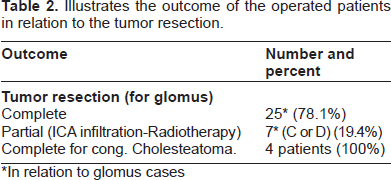
In relation to glomus cases
The outcome in the series was related to the type of pathology as well as the disease stage. Complete cure with complete pathology elimination without complications (100% success rate) could be achieved in the four cases of congenital cholesteatoma and the four cases with class B glomus ie, early disease (see Tables 2, 3 and 4). However in advanced cases of glomus jugulare (28 patients) (C and D stages) complete pathology resection could be achieved in 21 of them (75%) due to tumor adherence to ICA and those seven patients were referred to radiotherapy for complementary treatment but this didn't prevent the disease progression (see Table 2). The operative complications were also related to this group of 28 patients, in the form of facial paralysis in 20 of them (55.6%) and symptomatic vagal paralysis in 18 of them (50%). (See Tables 3 and 4 for the detailed rates and the management of the complication in each group). In the whole series there was one mortality in a young man in the 3rd decade of due to unexplained contra-lateral brain stem infarction. There was one case with persistent post-auricular sinus without evidence of infection and one 5th decade woman with auricular slough due to ischemia as a result of excessive extension of the pre-auricular limb of the incision (not adopted thereafter). For the post-operative morbidity other than the facial nerve, (see Table 4).
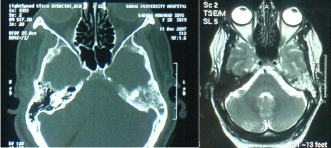
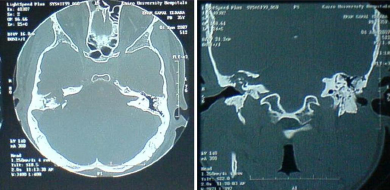
Preoperative CT of glomus jugulare.
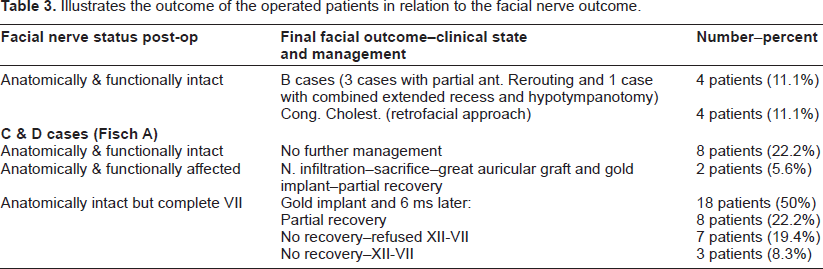
Illustrates the outcome of the operated patients in relation to the facial nerve outcome.
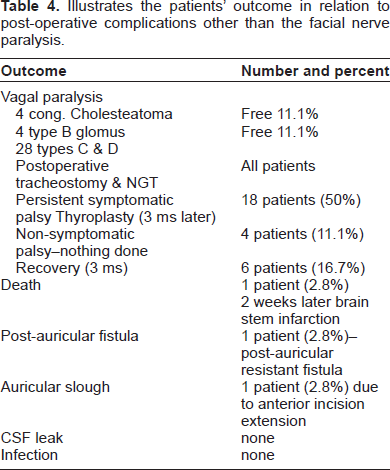
Illustrates the patients' outcome in relation to post-operative complications other than the facial nerve paralysis.
Discussion
The most common tumor in the jugular foramen is the hypervascular glomus jugulare tumor followed by the schwannomas of the cranial nerves within the foramen. Less common tumors are the meningiomas, the hemangiopericytoma, the chondrosarcoma, the plasmacytoma, metastases and malignant tumors arising in adjacent anatomic structures ie, the nasopharynx, the parotid and the temporal bone. 17
Glomus jugulare tumors present a formidable management problem because of their location and persistent invasive growth albeit usually slow and indolent. Surgical treatment of these tumors often causes considerable morbidity because of the extensive nature of skull-base procedures. With technical advancement in the surgical field, high speed drills and better microscopes, the focus of glomus jugulare tumor surgery has drifted away from the issue of resectability, virtually all of the glomus jugulare tumors are resectable (86%–94%).18–20 Anand et al 21 were able to claim complete resection of the tumor in 100% of cases. Nowadays the emphasis is towards the functional outcome.
Irrespective of the approach, a central problem in extirpating lesions of the lateral skull base is the location of FN. Because of its long and irregular route through the temporal bone, any attempt at petrous resection often forces the surgeon either to sacrifice the FN or, more commonly, to reroute it. 22
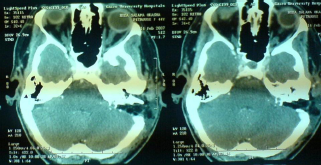
Postperative CT of glomus jugulare.
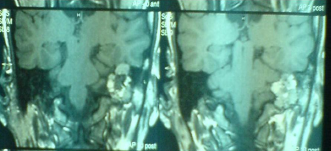
Preoperative MRI of glomus jugulare.
Historically, management of the FN required either anterior or posterior mobilization as described by Fisch 23 and House and Hitselberger, 24 respectively.
Anterior rerouting of the FN is a maneuver designed to enhance exposure of the jugular foramen and carotid canal during resection of cranial base tumors. At first it was described by Capps in 1952 however, despite mobilization, the tumor could not be removed completely. Because of postoperative facial weakness and spasm, Capps 5 expressed reluctance to repeat the procedure. The technique is used to preserve FN function and it has been widely reported and refined during the past 40 years. In 1964 Shapiro and Neues described microsurgical displacement of the FN supero-anteriorly after taking down the canal wall. After glomus tumor excision, the nerve was replaced, and temporary paralysis was resolved. Shapiro and Neues believed that this procedure was superior to the non-rerouting 25 . Selective approaches to preserve hearing were introduced, most notably by House and Farrior. During the latter part of the 1960s, McCabe et al 14 described the removal of glomus jugulare tumors with preservation of the osseus portion of the ear canal. Facial nerve trans-location was not performed, which allowed the use of the facial recess and exposure of the hypotympanum for tumor extirpation. In 1967, Farrior 15 modified the endaural hypotympanotomy of Shambaugh, 26 stressing a postauricular hypotympanotomy. This approach was very effective in small glomus tumors with medial extension, but it was not effective in tumors that involved the anterior and medial surfaces of the ICA. In 1971 Hilding and Greenberg described anterior rerouting from the first genu for a patient who had only a temporary facial paralysis after tumor removal 27 . One of the first systematic descriptions of management of the FN according to tumor anatomy was done by Fisch and Pillsbury in 1979. 7 They described three management strategies. For extensive tumors of the temporal bone and skull base, standard rerouting was done, which entailed first genu rotation with displacement of the nerve into a bony groove in the epitympanum. For tumors limited to the infra-labyrinthine space and pyramid tip, rerouting was not considered necessary. However, if the tumor extended into the nerve, the infiltrated portion was resected and later replaced with a nerve graft, maintaining the anterior transposition.
Glomus tympanicum pre operative CT & MRI.
Because of the unnecessary extensive FN manipulation risks of postoperative FN functional status, guidelines for selective use of rerouting techniques would be helpful. Transposition requires skeletonization of the FN in the fallopian canal, resection of the attachments to the canal, and displacement of the FN in an anterior or posterior direction. Extrinsic and intrinsic blood supply was placed in jeopardy, especially with first genu rerouting. However, rerouting of the FN provides maximal jugular bulb and tumor exposure so facilitates tumor resection. 10 According to Pensak and Jackler 22 when the surgeon approaches the jugular foramen, he must choose among three technical options: 1) Intact-canal-wall without FN rerouting (the so-called extended facial recess approach) 2) Canal-wall-down without FN rerouting, (the so-called Fallopian bridge technique or the retrofacial approach) and 3) Canal-wall-down with anterior FN rerouting (the classic Fisch A infratemporal fossa approach). The first option has the appeal of maintaining the structure and function of the ear canal and middle ear, but an intact-canal-wall procedure is not suitable for tumors with substantial anterior penetration. Use of a canal-wall-down procedure without FN rerouting is indicated when the ear canal wall is eroded or when tumor involvement of the middle ear is extensive. But unlike chronic ear surgery, the skull-base defect that created during a jugular foramen approach is too extensive for exteriorization. Furthermore, the highly skeletonized FN that bridges the surgical defect would be at risk of injury during routine cavity cleaning. Thus when the canal wall is taken down in jugular foramen surgery, the external auditory meatus must be sutured closed and the cavity is obliterated with either a free adipose tissue graft or a vascularized muscle graft. The third technical option, canal-wall-down with FN rerouting which was described by Fisch, 6 as the infratemporal fossa approach type A. This method is reserved for cases in which the tumor penetrates anteriorly with erosion of the carotid genu. In such cases, the added complexity of FN rerouting is justified by the need for unhindered exposure of the vasculature to avoid a potentially devastating carotid injury.
Congenital cholesteatoma preoperative CT axial and coronal.
Von Doersten and Jackler 10 detailed more the handling of the facial nerve in relation to approaches to the jugular foramen. They described three levels in handling the facial nerve in relation to its anterior rerouting through 20 cadavers dissection. Those were canal wall up–-second genu pivot point (CWU-2G 11 ) (or the intact canal wall technique); canal wall down–-second genu pivot point (CWD-2G 12 ) (or the partial anterior transposition of the facial nerve); and canal wall down–-first genu pivot point (CWD-1G 13 ) (or the classic Fisch A approach). And they claimed that- through anatomic study- the gain of the distance between the vertical facial nerve at the stylomastoid foramen and the lateral edge of the jugular foramen (a distance that is required for proper tumor and vascular control without damage to the facial nerve) varies considerably with those three choices. With the first technique the mean distance is 4.2 mm, with the second technique the distance becomes 10 mm and it increased to 14 mm for the third technique. According to them, with the first technique the jugular bulb only is exposed, with second the bulb and 6 mm of the posterior aspect of the carotid genu is exposed and the third approach allows total exposure of the entire carotid genu. And hence proper approach selection tailored to the lesion allows proper lesion removal with preservation of the facial nerve function without the need for unnecessary retractions and mobilization. Gjuric and Bilic 16 introduced what they called the transmastoid infralabyrinthine approach (TM-IL 14 ) for jugular paraganglimas, in which they preserved the structure and function of the external auditory canal and middle ear through an extended recess approach together with opening the retrofacial air cells and removing the bone anterior, posterior and medial to the facial nerve at the stylomastoid foramen and sepapration of the digastric muscle from the mastoid process. The facial nerve hence is liberated at the stylomastoid foramen which allows its mobilization at this level to expose the jugular bulb and by superior reflection of the tympanomeatal flap, they can expose the ICA up to the first genu. They claimed that through this approach surgical cure was achieved in (84%) of all the cases and in (73%) of the cases with IFT-A 15 approach, referring this to the fact that the IFT-A was selected to more aggressive disease form. Regarding their facial nerve outcome results, they got a postoperative House-Brackmann grade of I or II facial nerve function in 84% of TM-IL cases and in 56% of the IFT-A cases. They concluded that the TM-IL approach with individually tailored management of the facial nerve fulfills the long-term requirements of both keeping good postoperative facial function and obtaining adequate tumor resection.
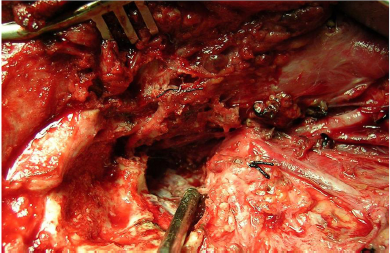
Operative view of Fisch A approach.

Preoperative angiography of glomus jugulare.
Going through this enormous cumulative literature, we can summarize the levels of dealing with facial nerve in jugular foramen surgery into the following levels:
The conductive hearing mechanism is also disturbed both functionally and anatomically due to removal of middle ear contents except the stapes and the stapedius, in addition to the occlusion of the Eustachian tube and the EAC.
For congenital cholesteatomas of the hypotymanum and the middle ear we selected the retrofacial approach. We believe that unlike glomus, this approach is applied to the extremely vascular and adherent tumor to the surrounding structures (specially the ICA) which entails a wide approach for proper vascular control, congenital non-vascular cholesteatoma, non-adherent and readily resectable lesion. In such technique we did not attempt to mobilize the facial nerve at all and we did not ligate nor expose cervical blood vessels or nerves although we selected a vast approach that allowed us to properly remove the disease without facial nerve affection.
For the glomus jugulare lesions class B (according to Fisch classification), we performed the partial anterior rerouting technique (the so-called canal wall down second genu pivot point) for three cases.
For one case of glomus jugulare class B (according to Fisch classification) we performed the transmastoid infralabyrinthine approach. The vertical mastoid segment of the facial nerve was partially rerouted at the middle of the vertical segment below the chorda tympani (neither at the stylomastoid foramen nor totally till the second genu). The limited mobilization was found to be sufficient to expose the jugular bulb and the posterior aspect of the ICA and to liberate the tumor from it since the tumor in this particular case was not markedly adherent to the ICA. This is a little bit similar to the CWU 2nd G pivot described by Von Doersten and Jackler 10 and to the transmastoid infralabyrinthine approach described by Gjuric and Bilic 16 with some differences regarding the level of facial nerve mobilization. In such approach the middle ear structure and function are not disturbed and the outcome of the facial nerve was excellent.
For larger glomus jugulare lesions (classes C or D according to Fisch), a classic Fisch infratemporal fossa type A approach 6 was selected (the so-called canal wall down first genu pivot point).
The facial nerve outcome was excellent at the first three approaches without facial nerve affection at all. But for the fourth approach (infratemporal fossa typeA) immediate postoperative complete facial paralysis was present in 20 cases (55.6%) despite the anatomical integrity in 18 of them (50%) but only 8 patients (22.2%) partially recovered their facial nerve function without further intervention (see Table 3).
Unfortunately, and despite the numerous literature in handling glomus jugulare tumor over the last decades, comparing the results is very difficult due to the marked difference between patients' groups regarding the disease stage, the approaches adopted, the follow up period and the grading of the facial nerve outcome. The literature is full of more general guide lines than precise protocol of management. This requires further research with this respect to try to unify the management strategies, however the rarity of the condition as well as the interested otologists and skull base surgeons, makes this hard to achieve one center and possibly a multi-center study may be more convenient.
Conclusion
We believe that total anterior rerouting of the facial nerve carries a high risk of facial paralysis postoperatively even if the anatomical integrity of the nerve was preserved possibly due to excessive handling and devascularization and may be fibrosis in the cavity. So it should be reserved for cases where the lesion extends beyond the vertical ICA to the horizontal ICA or the petrous apex and particularly in lesions known for their adherence and excessive vascularity. Otherwise, for less extensive lesions and less aggressive pathologies, less aggressive approaches in the previously described leveling could be adopted with less hazards.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Abbreviations
Acknowledgement
We would like to express our deep gratitude to our colleagues – both medical and paramedical – in the departments of ENT, anaesthesia and ICU in Cairo university hospital for their friendly and positive cooperation throughout our practice period in the last 20 years. The gratitude is also extended to our radiology team whom without their help this patient care could not have been achieved. Finally we are extremely thankful to our patients for their cooperation, patience and understanding.