
Abstract
EGFR belongs to the ErbB family of receptor tyrosine kinases and is associated with worse prognosis in head and neck squamous cell carcinoma (HNSCC). Cetuximab is a monoclonal antibody to the extracellular domain of EGFR and inhibits its downstream actions via multiple mechanisms. Besides its proven efficacy in locally advanced and incurable HNSCC, cetuximab has the distinct advantage of having a relatively tolerable side effect profile and not potentiating radiation toxicity. Though therapies for advanced HNSCC are evolving, locoregional recurrence and/or distant metastases occur in a large percentage of patients. Though some patients can be salvaged with surgery or radiation therapy, the majority are incurable, and are treated palliatively with systemic therapy. In the setting of first line therapy for recurrent/metastatic HNSCC, the EXTREME trial provided level 1 evidence that cetuximab improves overall survival when combined with cisplatinum and 5 FU. Following progression on first line chemotherapy, several phase II trials suggest that cetuximab monotherapy is a reasonable choice in this setting. Future studies should concentrate on clinical and molecular markers that may allow more personalized approaches to treating HNSCC, and combining EGFR inhibitors with other agents in a synergistic approach.
Introduction
Worldwide, an estimated 12.7 million cancer cases and 7.6 million cancer deaths were expected in 2008. 1 In the US, an estimated 1.53 million new cases of cancer were expected be diagnosed, with over 569,000 deaths in 2010. Head and neck squamous cell carcinoma (HNSCC) accounts for 49,260 of these new cases with an estimated 11,480 deaths. 2 In addition to chronic tobacco and alcohol use, the emergence of human papillomavirus (HPV) as a risk factor for HNSCC has garnered considerable interest over the past decade.3,4 In a recent meta-analysis of 5681 patients with HNSCC, the prevalence of HPV-positive tumors was 22%. HPV-positive HNSCC is associated with better prognosis than HPV-negative HNSCC, especially for oropharyngeal primaries.5,6 HPV-positive patients had higher response rates after induction chemotherapy and chemoradiation, and better overall survival than HPV-negative patients. 7
Epidermal Growth Factor Receptor (EGFR)
The EGFR belongs to the ErbB family of receptor tyrosine kinases, which includes ErbB-1 (EGFR), ErbB-2 (HER2), ErbB-3 (HER3) and ErbB-4 (HER4). EGFR is composed of three distinct domains: an extracellular ligand-binding domain, a hydrophobic transmembrane domain involved in interaction between receptors, and an intracellular tyrosine kinase domain that phosphorylates various intracellular signaling proteins and the receptor itself. There is a high degree of homology amongst the tyrosine kinase domains in the ErbB family of receptors. In contrast, the extracellular binding domains do not share this uniformity. This disparity allows the ErbB receptors to bind various extracellular ligands, including EGF, transforming growth factor α (TGF-α), amphiregulin, heparin-binding EGF, the poxvirus mitogens, epiregulin and β-cellulin, resulting in the modulation of a multitude of downstream pathways.8–12 Of these ligands, EGF and TGF-α appear to be the most important in HNSCC. 13
Binding of a ligand to the EGFR induces receptor homodimerization or heterodimerization (with other ErbB receptors), which results in autophosphorylation of tyrosine residues on the tyrosine kinase domains. This event subsequently initiates a complex intracellular signaling cascade activating downstream proteins such as mitogen-activated protein kinase (MAPK), which is involved in cell proliferation; phosphotidylinositol-3 kinase (PI3K), which mediates cell cycle progression and survival; and the signal transducer and activator of transcription (STAT) family of proteins, which mediates cell division, survival, motility, invasion and adhesion. Heterodimerization of various ErbB receptor combinations allows for a wide array of signaling pathways that can potentially be activated by the binding of a single ligand to the extracellular domain.
EGFR activation leads to a cascade of cellular responses including cell cycle progression, proliferation, angiogenesis and inhibition of apoptosis. These downstream effects implicate dysregulated EGFR as a promoter of malignancy.14,15 Initial studies reporting the prognostic significance of EGFR expression in HNSCC noted that high levels of EGFR and TGF-α were associated with poor survival.16–19 A meta-analysis reviewing the relationship between EGFR expression and cancer prognosis revealed EGFR as a strong prognostic indicator in head and neck, ovarian, cervical, bladder and esophageal cancers. In these cancers, EGFR overexpression was associated with reduced recurrence-free or overall survival rates in 70% of the studies identified. In contrast, the relationship between EGFR expression and patient outcomes in NSCLC was found to be significant in only 30% of studies identified. 20 Activating EGFR mutations create ligand-independent pathways in lung adenocarcinoma; however this is uncommonly seen in HNSCC, which employs a ligand-dependent pathway.21,22
Variations in the expression of EGFR can be explained by polymorphisms of the gene encoding EGFR. Bandres et al described EGFR polymorphisms and their prognostic significance in HNSCC. The R497 K polymorphism in exon 13 as well as the (CA)n repeat polymorphism in intron 1 (n ≥ 17) were both found to be associated with a decrease in disease-specific mortality compared to the wild-type codon 497 and (CA)n where n < 17. Both polymorphisms have been shown to attenuate EGFR expression and function, leading to the conclusion that genetic variants of EGFR with inherently reduced expression levels correlate with improved survival in patients with HNSCC. 23 A Japanese study examining the molecular status of EGFR in HNSCC revealed that patients whose tumor samples showed hyperphosphorylated wild type EGFR had earlier recurrence at 1 year than those with non-hyperphosphorylated wild type EGFR (75% vs. <25%, respectively). Their results support EGFR's malignant potential and suggest hyperphosphorylated EGFR as a marker of poor prognosis in patients with HNSCC. 24 Similar conclusions have been made in esophageal squamous cell carcinoma, which is similar in pathophysiology to HNSCC, where phosphorylated EGFR correlates with TNM stage, lymph node metastasis and poor disease outcome. 25 Other studies implicate that along with EGFR overexpression from gene amplification, increased gene copy number may also have prognostic significance in HNSCC, as a high copy number was significantly associated with poor overall survival.26,27
EGFR-mediated activation of the PI3K/Akt pathway is essential for regulating apoptosis in a normal cell. EGFR-activated PI3K activates Akt, which regulates key elements in the apoptosis pathway, including Bad and caspase 9. Conversely, PTEN (phosphatase and tensin homolog deleted on chromosome 10) inhibits Akt, allowing PTEN to promote apoptosis and regulate cellular processes such as cell cycling and translation. PTEN inactivation resulting in constitutively activated Akt is a mechanism for tumor initiation and progression.28–30 Par-4, an anti-apoptotic protein, is essential for PTEN-mediated apoptosis, and inactivation of Par-4 by Akt promotes the survival of cancer cells. 31 mTOR is an essential downstream effector of the PI3K/Akt pathway that amplifies anabolic signals regulating the utilization of energy and G1 to S phase progression.32–34 A recent study has shown that inhibition of mTOR in HNSCC models suppresses lymphangiogenesis, preventing metastasis to locoregional lymph nodes. 35
EGFR also plays a role in the expression of nuclear proteins. Upon translocation to the nucleus, EGFR phosphorylates and activates DNA-dependent protein kinase, which is involved in repairing double-stranded DNA breaks caused by chemotherapy and radiation.36,37 In addition, increased expression of DNA repair proteins ERCC1 and XRCC1 is seen when EGF is introduced to cancer cells, implicating EGFR as a promoter for these enzymes. 38 EGFR also binds to the promoter regions of cyclin D1 and cyclin E, thereby increasing their expression and cellular proliferation.39,40
Cetuximab
Cetuximab (Erbitux, ImClone Systems) is a human-murine chimeric IgG1 monoclonal antibody (mAb) (65% human and 35% murine), which targets domain III of the extracellular region of EGFR.41,42 Cetuximab binds to and inhibits EGFR through multiple mechanisms. It competes with EGF for its binding site and thus prevents activation of the receptor through a ligand-dependent process. Cetuximab also inhibits EGFR from adopting the conformation required to dimerize with another receptor, thereby preventing initiation of the phosphorylation cascade. Additionally, cetuximab has been shown to inhibit cell growth by influencing cellular proliferation and apoptosis. In vitro exposure of HNSCC cells to cetuximab induces accumulation of cells in the G1 phase of the cell cycle with a subsequent decrease in the percentage of cells in S phase, reducing the number of cells that complete the cell cycle. The pro-apoptotic effects can be seen by the accumulation of hypophosphorylated retinoblastoma protein, increase in Bax expression and concurrent decrease in Bcl-2 expression in HNSCC cells exposed to cetuximab. 43
In addition to their inhibitory role on EGFR and influence on the cell cycle and apoptosis, it has been shown that mAbs decrease EGFR signaling through increased internalization and degradation of the receptor in HNSCC cells. 44 This internalization prevents EGFR from binding to its native ligands and disrupts the cascade. Cetuximab also displays an immune-mediated mechanism of action by recruiting natural killer (NK) cells and macrophages, mediating antibody-dependent cell-mediated cytotoxicity (ADCC) in HNSCC, NSCLC and metastatic colorectal cancer.45–48
The mechanism of radiosensitization in cetuximab was first described by Rodemann et al (2005). They noted that radiation-induced activation of DNA-dependent protein kinase, which is required for DNA damage repair, may be hampered by cetuximab and that this process is associated with radiosensitization. 49 Several other pre-clinical studies support the increased effectiveness of combining cetuximab with radiotherapy (RT) and/or chemotherapy.50–52
Other EGFR inhibitors
Other mAbs targeting EGFR have emerged recently. Matuzumab is the humanized form of murine mAb 425 that binds to an epitope on domain III of EGFR distinct from the cetuximab binding site on the same domain. It plays no role in inhibiting ligand-induced activation of the EGFR; however it blocks the formation of the stable conformation of EGFR required for dimerization. The non-competing actions of matuzumab and cetuximab and their separate binding sites suggest a potential benefit to combination therapy, however further research is required. 53 Nimotuzumab is another humanized mAb that also binds to domain III of the extracellular region of EGFR in an area overlapping both the cetuximab and EGF binding sites. Uniquely, nimotuzumab inhibits EGF from binding yet allows the receptor to adopt its active conformation, allowing a basal level of signaling. 54
Panitumumab is a fully human IgG2 mAb that blocks the binding of both EGF and TGF-α. It is potentially less immunogenic than cetuximab and rarely causes severe infusion reaction. Panitumumab also has a longer half-life and higher affinity for EGFR compared to other mAbs.55,56 Preclinical studies show that panitumumab augments radiation-induced DNA damage and apoptosis, and in combination with radiation, is superior to panitumumab or radiation alone. 57 A recent study investigated the use of panitumumab, carboplatin, paclitaxel and IMRT in the treatment of late-stage HNSCC and found that the combination therapy is highly active and well-tolerated. 58
Tyrosine kinase inhibitors (TKIs) antagonize EGFR signaling by inhibiting the tyrosine kinase activity of the receptor. TKIs such as erlotinib (Tarceva) reversibly inhibit the tyrosine kinase activity of EGFR, competing with adenosine triphosphate for its binding site. 59 The use of TKIs in HNSCC is currently limited to phase I and phase II trials, with erlotinib and gefitinib (Iressa) showing modest increases in overall survival and progression-free survival in these patients. 60 Studies of erlotinib used as a single agent as well as in combination with other drugs demonstrate its anti-malignant effects in HNSCC. 61 A phase III trial of gefitinib versus methotrexate in recurrent HNSCC revealed that gefitinib does not demonstrate an improvement in overall survival compared to methotrexate, and in fact has a higher rate of tumor hemorrhage. 62
Efficacy
Concurrent cetuximab in locally advanced HNSCC
The typical treatment paradigm for many locally advanced HNSCC, including nasopharynx, larynx, oropharynx and hypopharynx primaries, is concurrent chemotherapy plus external beam radiation therapy. This has been established by multiple randomized controlled trials in advanced larynx, nasopharyngeal, and oropharyngeal sites.63–65 In addition the Meta-analysis of chemotherapy in HNSCC (MACH NC) found a 6.5% overall survival benefit at 5 years for combining concurrent chemotherapy with radiation and the benefit appears superior for platinum monotherapy when compared to other chemotherapy regimens. In subgroup analysis, the benefit of adding chemotherapy to radiation diminished with advancing age, so that there was no significant advantage to concurrent chemotherapy for patients older than 70 years. 66
Bonner et al performed the seminal phase III randomized controlled trial that established the role of cetuximab in locally advanced HNSCC.67,68 They randomized 424 advanced HNSCC patients (oropharynx, hypopharynx and larynx primaries) to RT alone versus RT plus cetuximab (400 mg/m2 loading dose, followed by seven weekly doses at 250 mg/m2). Radiation therapy was administered for 6–7 weeks using once daily, twice daily, or concomitant boost techniques. They found that adding cetuximab to external beam radiation therapy improved median overall survival from 29.3 months (95% CI 20.6–41.4) to 49.0 months (32.8–69.5) (hazard ratio [HR] 0.73, 95% CI 0.56–0.95; P = 0.018) and 5-year overall survival from 36.4% to 45.6% (hazard ratio [HR] 0.73, 95% CI 0.56–0.95; P = 0.018). Cetuximab also improved median duration of locoregional control from 14.9 months to 24.4 months (hazard ratio for locoregional progression or death, 0.68; P = 0.005). In subgroup analysis, patients with oropharyngeal (as opposed to larynx or hypopharynx) primary tumors, lower T stage, concomitant boost radiation, advanced neck disease, high performance status and younger age had increased benefit, though these results should be interpreted cautiously as the trial was not powered for these subgroup analyses. The rate of grade 3/4 mucositis was not appreciably different for RT (51.9%) versus cetuximab RT (55.8%); grade 3/4 dysphagia was also similar for RT (29.7%) versus cetuximab RT (26%). That these serious toxicities were similar with or without cetuximab represents a significant advantage over typical chemotherapy regimens, which uniformly intensify radiation-caused mucositis and dysphagia. The cetuximab arm did have 17% grade 3/4 acneiform rash and 3% infusion reaction. Interestingly, of the patients receiving cetuximab, those who developed a grade 2+ acneiform rash had significantly longer overall survival compared to those who had a grade 0–1 rash (68.8 months vs. 25.6 months P = 0.002). This trial led to FDA approval in 2006 for cetuximab in conjunction with radiation therapy for locally advanced HNSCC.
With regard to whether concurrent cetuximab radiation is as effective as cisplatinum radiation, there is no randomized data, and the retrospective data is conflicting. Koutcher et al reported a retrospective study in advanced HNSCC patients treated with concurrent cisplatinum RT versus cetuximab RT. They noted 2 year locoregional failure of 5.7% in the cisplatinum patients versus 40% in the cetuximab patients. However, the cetuximab patients were clearly older than the cisplatinum group (40% versus 5% older than 70). 69 On the other hand, Caudell et al also reported a retrospective study of cisplatinum RT versus cetuximab RT, and noted no significant differences in locoregional control or overall survival. Significantly, all the patients treated with cetuximab were treated on protocol, so there were no significant differences in age or performance status between the two groups. 70 Despite a lack of randomized data, cisplatinum RT is typically considered first line treatment for locally advanced HNSCC, with cetuximab RT often reserved for patients who are older, unable to tolerate cisplatinum, or with a poor performance status.
RTOG 0522 asked whether adding cetuximab to concurrent cisplatinum RT is beneficial. Though the data are not yet mature, at median follow up of 2.4 years, adding cetuximab to cisplatinum RT appears to have no advantage over cisplatinum RT in terms of progression free survival (2 year rates: 63% vs. 64%, P = 0.66), or overall survival (2 year rates: 83% vs. 80% P = 0.17). 71
Cetuximab with re-irradiation for recurrent HNSCC with curative intent
Though radiation techniques continue to evolve, locoregional recurrence after radiation (chemoradiation) is still a major concern, developing in about 20% of patients treated for advanced larynx cancer, 72 or after postoperative chemoradiation for high risk features,73,74 and up to 50% treated for locally advanced unresectable HNSCC. 75 While salvage surgery after radiation failure is the primary curative option, only a small minority of patients will be candidates due to extent of recurrence, medical fitness for surgery, or patient preference. 76 In unresectable patients, the only remaining potentially curative option is reirradiation with or without concurrent chemotherapy. However, reirradiation comes with a significant risk of serious acute and late toxicity. RTOG 9610 treated eighty six previously radiated patients with a second primary/ recurrence with concurrent 5FU, hydroxyurea and reirradiation. They noted significant grade 3/4 mucositis, pharyngeal toxicity, neutropenia and six treatment related deaths, including two who died of hemorrhage from the primary site. Recently, Janot et al reported a phase III randomized controlled trial of 130 previously radiated patients with recurrent HNSCC who were randomized to salvage surgery versus salvage surgery plus full dose reirradiation with concurrent 5 FU and hydroxyurea. Disease free survival was improved in the reirradiated arm vs. observation (hazard ratio of 1.68, 95% CI, 1.13 to 2.50; P = 0.01), but this came at the cost of increased acute and late toxicity. At 2 years, 39% of patients in the RT arm versus 10% in the observation arm experienced grade 3/4 late toxicities, including sclerosis, trismus, and osteoradionecrosis. 77
Given the high rate of grade 3/4 toxicity associated with chemotherapy reirradiation, cetuximab reirradiation would seem to be an attractive option, especially since the toxicity of cetuximab is not typically additive to radiation. Several small series have explored this paradigm. Zwicker et al reirradiated ten patients (with assorted primary tumors) with recurrent HNSCC using IMRT to a median dose of 50.4 Gy and cetuximab (loading dose 400 mg/m2 and weekly dose 250 mg/m2. The median overall survival time after initiation of reirradiation was 7 months and the 1-year locoregional control (LRC) rate was 44%.
Severe acute toxicity included one fatal infield arterial bleed and one flap necrosis. Severe late toxicities were noted in 2 patients, including fibrosis of the temporomandibular joint and esophageal stenosis. 78 Balermpas conducted a similar trial with seven patients (two oral cavity and 5 oropharynx primaries) and similar radiation/cetuximab doses. They note that two patients achieved a complete response after 7 months, one remained stable, three progressed, and one died from pneumonia prior to restaging. There were no treatment related deaths and no acute grade 3 mucositis. After treatment one patient developed a grade 2 trismus, another grade 3 abacterial salivary gland inflammation. An alternative method of reirradiation is using stereotactic body radiotherapy (SBRT) which treats using a small number of radiation fractions (fraction size is larger than in typical HNSCC radiation) often to a smaller treatment area. Heron et al reported a matched case control series of recurrent HNSCC patients treated with SBRT versus SBRT plus cetuximab. 79 The most common radiation scheme was 44 Gy in 5 fractions in 9 to 14 days. The cetuximab group received 400 mg/m2 loading dose 1 week prior to SBRT followed by weekly cetuximab at 250 mg/m2 weekly for the duration of SBRT. The 1- and 2-year local control rates were promising at 53.8% and 33.6% for SBRT patients, and 78.6% and 49.2% for SBRT plus cetuximab. Significantly, there were no grade 4 or 5 toxicities in either arm, and in fact there were only three grade 3 toxicities in the study: 1 in SBRT only had xerostomia, 2 in SBRT plus cetuximab had dysphagia and xerostomia. Though the evidence for cetuximab in reirradiation is clearly very preliminary, this paradigm deserves further investigation, given the often devastating toxicity associated with concurrent chemotherapy reirradiation, and the encouraging early results with concurrent cetuximab.
Cetuximab in first line therapy of incurable (recurrent or metastatic) HNSCC
Depending on initial therapy and extent of disease, recurrent HNSCC may occasionally be treated with curative intent ie salvage surgery or radiation (or reirradiation). But all too often, recurrent disease (like metastatic HNSCC) is incurable, and treated palliatively with systemic therapy or best supportive care. The prognosis for recurrent or metastatic HNSCC is poor, with overall survival of about 5–7 months.80,81 Untreated recurrent/metastatic HNSCC has a median overall survival of about 4 months. 82 Historically, many single agent chemotherapy compounds have been examined in this setting, with the most active and extensively used agents being single agent cisplatinum, methotrexate, 5 FU, and bleomycin. 83 Several randomized trials have demonstrated an improvement in response rate to a cisplatinum + 5FU (PF) doublet compared to single agent chemotherapy. Three studies by Forastiere, Clavel, and Jacobs demonstrate a 31%–32% response rate to PF versus a 10%–17% response to single agent chemotherapy, but no significant improvement in overall survival.84–86
Burtness et al randomized 117 patients with recurrent/metastatic HNSCC to cisplatin every 4 weeks or the same regimen with weekly cetuximab. Following progression on the cisplatinum arm, cross-over to cetuximab was allowed. The primary end point was progression free survival. Objective response rate was 26% versus 10% (P = 0.03) in favor of cetuximab, but median progression free survival (4.2 versus 2.7 months) and overall survival (9.2 versus 8 months) were not significantly different. As in the Bonner trial, there was a survival advantage among the cetuximab patients for development of skin rash. 87
The EXTREME trial expanded upon these results and established the role of cetuximab in first line treatment of incurable HNSCC. 88 The EXTREME trial randomized 442 patients with recurrent/ metastatic HNSCC who were ineligible for local therapy to platinum (cisplatinum or carboplatinum) plus 5FU versus the same regimen plus cetuximab (400 mg/m2 initially, followed by weekly doses of 250 mg/m2). The patients received either cisplatin (100 mg/m2 on day 1) or carboplatin (at an area under the curve of 5 mg per milliliter per minute on day 1) and an infusion of fluorouracil (1000 mg/ m 2 per day for 4 days) every 3 weeks. Whether to give the patient cisplatin versus carboplatin was at the discretion of the investigator; approximately one third of patients did receive carboplatin (which is associated with worse response rates than cisplatinum). Patients received a maximum of six cycles of chemotherapy. Patients with unacceptable toxicity to one of the study drugs received only the tolerated drugs until disease progression. After a minimum of six cycles of chemotherapy, patients in the cetuximab arm who had at least stable disease continued on cetuximab monotherapy until disease progression or unacceptable toxicity. Patients in the chemotherapy-alone group received no further treatment (no cross-over from the chemotherapy-alone arm to cetuximab following progression). The cetuximab arm had significantly prolonged median overall survival (10.1 mo vs. 7.4 months; hazard ratio for death, 0.80; 95% confidence interval, 0.64 to 0.99; P = 0.04), median progression-free survival (5.6 mo vs. 3.3 mo; hazard ratio for progression, 0.54; P < 0.001) and response rate (36% vs. 20%; P < 0.001). Interestingly, in subgroup analysis, there appeared to be more benefit for patients with oral cavity primary tumors (unlike the Bonner study). Cetuximab was not associated with increased risk of overall grade ¾ toxicity (82% versus 76%), or hematologic toxicity, specifically, neutropenia (22% vs. 23%), anemia (13% vs. 19%) or thrombocytopenia (11% vs. 11%). However, the cetuximab arm did have 9 cases of sepsis versus 1 for the chemotherapy alone arm, and also appeared to increase the risk of potassium, magnesium and calcium electrolyte disorders. In addition, 9% of the cetuximab patients developed grade 3 skin reactions and 3% had grade 3 or 4 infusion reactions. This trial established a new standard for first line therapy in incurable HNSCC, and led in November 2011 to FDA approval for cetuximab in combination with platinum-based therapy plus 5-FU for the first-line treatment of patients with recurrent/metastatic HNSCC.
There is some preliminary evidence for the addition of cetuximab to taxanes in the first line setting. Hitt et al treated 46 recurrent/metastatic patients with paclitaxel (80 mg/m2) and cetuximab (400/250 mg/m2), weekly, until disease progression or unacceptable toxicity. The overall response rate was 54% with 22% complete responses. Median progression-free and overall survival times were 4.2 and 8.1 months. The most common grade ¾ toxicities were acne like rash (24%), asthenia (17%) and neutropenia (13%). The relatively high response rate and reasonable toxicity profile make this paradigm an attractive area for future studies, especially in those patients who cannot tolerate further platinum therapy. 89
Cetuximab in second line therapy of incurable (recurrent or metastatic) HNSCC
Unfortunately, most patients will not respond to first line platinum based chemotherapy, and even those who do will eventually progress. Once patients have progressed through first line chemotherapy, the prognosis is extremely poor. Patients who have progressed on cisplatinum based chemotherapy have a response rate to further chemotherapy of about 3%. 90 Furthermore, patients are often debilitated and less able to tolerate further chemotherapy. Overall survival is likewise extremely poor- in a retrospective study Leon et al reported a median survival of 2 months for best supportive care, and 3.5 months for second line chemotherapy. 91
Shin performed a phase IB study of weekly cetuximab in combination with cisplatin (100 mg/m2 every 3 weeks) in patients with recurrent HNSCC (4/12 having received previous chemotherapy) to determine the optimal safe biological dose of cetuximab. They found that a loading dose of cetuximab at 400 mg/m2 with a maintenance dose at 250 mg/m2 achieved near complete saturation of EGFR and recommended this regimen for future studies. Though not the main objective, they noted that six of nine evaluable patients achieved major responses, including two who had a complete response. Among the toxicities attributable to cetuximab were one grade 2 and one grade 3 allergic reaction (shortness of breath) and grade 3 folliculitis-like rashes in two patients. 92
Expanding on Shin's work, Vermorken, Herbst, and Baselga all performed phase II trials of cetuximab alone (n = 103) or in combination with cisplatinum/carboplatinum (n = 96) in recurrent patients who had already progressed though first line cisplatinum or carboplatinum based regimens. In all three studies, cetuximab was given at an initial dose of 400 mg/m2 followed by subsequent weekly infusions of 250 mg/m2. In the cetuximab chemotherapy studies, cetuximab was followed by platinum chemotherapy either at the same dose that they were at during disease progression prior to entry into the study or at 75–100 mg/m2 (cisplatin). After a minimum of 2–4 cycles, patients with at least stable disease (SD) continued until disease progression or unacceptable toxicity. Outcomes for the three trials were remarkably consistent. Collectively, they report response rates between 10%–13%, median time to progression of 2.2–2.8 months, and median OS between 5.2–6.1 months. Notably, in the cetuximab monotherapy trial, patients progressing on cetuximab then received cetuximab cisplatinum. In these patients, no one who progressed on cetuximab alone responded afterwards to cisplatinum. There appeared to be no significant difference whether patients were treated with cetuximab alone or with cisplatinum/carboplatinum. In the collective paper, the authors compare their results to a retrospective cohort consisting of 151 patients, 45% receiving best supportive care, 28% receiving chemotherapy, 17% receiving radiotherapy, 10% receiving chemoradiotherapy (CRT). The cetuximab patients' overall survival compared favorably to the retrospective patients who had a median OS of only 3.4 months, though it should be noted the median KPS for the retrospective patients (KPS 70) was worse than the cetuximab patients (KPS 80).
Grade 3/4 side effects were relatively rare, with 3% developing significant rash. One patient in the cetuximab monotherapy study died due to infusion reaction.93–96
Based on the similar response rate whether cetuximab was combined with cisplatinum or not in these phase II studies, and the fact that no patients who progressed on cetuximab monotherapy in the Vermorken trial then had a response to cisplatinum afterwards, there is no evidence that cisplatinum therapy adds anything to cetuximab in these second line patients. This, combined with the favorable toxicity profile of cetuximab in these often-debilitated patients, makes cetuximab monotherapy a very attractive choice as second line therapy. Cetuximab was FDA approved as a single agent in second line therapy after platinum-based failure in March 2006.
Safety
In general, cetuximab is associated with a favorable toxicity profile compared to many other chemotherapies typically used in advanced HNSCC. Toxicities particular to cetuximab appear to be acneiform rash, infusion reactions, and electrolyte disturbances.
In the locally advanced HNSCC setting, toxicities associated with chemoradiotherapy (CRT) include xerostomia, dietary restrictions, dysphagia, taste disturbances and pain. 97 With the use of intensity-modulated radiotherapy (IMRT) as one of the therapeutic standards in HNSCC, the incidence of radiation-related adverse events has been significantly reduced compared to conventional or three-dimensional techniques. In particular, salivary gland sparing leads to a significant reduction of xerostomia, attenuating the oral biological effects of local treatment.98–101 Relying on this evidence, Merlano et al attributed an increased occurrence of stomatitis (65% of study population with grade 3 or 4 stomatitis) to the addition of cetuximab in their trial of alternating radiotherapy and chemotherapy in combination with cetuximab in the treatment of advanced HNSCC. However, they mentioned that the stomatitis was manageable with total parenteral or enteral nutrition, and therefore, does not preclude treatment. 102 Curran et al studied the QOL in patients with advanced HNSCC treated with radiation alone or radiation with cetuximab. They found that the incidence of adverse events, including mucositis, xerostomia, dysphagia, weight loss and performance status deterioration, between the two groups was comparable, with the exception of acneiform rash and infusion-related events. 103 In the EXTREME trial, there was no significant difference in the rate of overall grade 3/4 toxicities with the addition of cetuximab to cisplatinum 5FU. The individual toxicities that were significantly increased were skin reaction (<0.001), anorexia (0.05), hypomagnesia (0.05), and sepsis (0.02). Of 219 patients receiving cetuximab in the EXTREME trial, 9% had grade 3 skin reactions (no grade 4) and 3% had severe infusion-related reactions. 104
Acneiform rash is the most common toxicity associated with cetuximab. EGFR inhibitors are associated with various skin reactions, including a macular, papular, pustular rash, commonly referred to as acne-like rash (or folliculitis); xerosis; fissures; telangiectasia; hyperpigmentation and hair and nail changes. The most common skin reaction is the acne-like rash, which is generally distributed in areas rich in sebaceous glands, such as the face, neck and retroauricular area, the shoulders, the upper trunk (V-shaped) and the scalp. 105 A recent expert panel recommended that when radiation and EGFR inhibitor caused grades 2/3 radiation dermatitis, it should be treated by cleaning and drying the affected area (even when ulcerated) and possibly topical applications including drying gels, hydrophilic dressings, anti-inflammatory emulsion (eg, trolamine, hyaluronic acid cream), zinc oxide paste, Silver sulfadiazine or beta glucan cream. They recommended that Grade 4 radiation dermatitis defined as skin necrosis or ulceration of full thickness dermis or spontaneous bleeding from the involved site be treated primarily by a wound specialist. 106
Interestingly, severe infusion reactions to cetuximab are particularly common in the southeast United States, as prevalent as 22% in one study. 107 Chung et al found that 17/25 patients who had a hypersensitivity reaction had IgE antibodies against cetuximab in pretreatment serum samples. The IgE antibodies were specific for the oligosaccharide, galactose-α-1,3-galactose, which is present on the Fab portion of the cetuximab heavy chain. All humans have IgG antibodies specific for galactose-α-1,3-galactose, which is closely related to substances in the ABO blood group, but why some patients developed IgE antibodies and why this happens more often in certain regions is unknown. 108
Hypomagnesia occurs with anti-EGFR antibodies, and the mechanism may be related to inhibition of magnesium reabsorption in the ascending loop of Henle. It occurs shortly after starting cetuximab and resolves within weeks of discontinuation. Therefore, magnesium and potassium must be routinely monitored and repleted as necessary. 109
Future Directions
Though the Bonner and EXTREME trials represent the tremendous progress that has been made in the use of anti-EGFR therapy in HNSCC, there are some clear avenues of research for the future.
Mechanisms of resistance to cetuximab
Both these randomized trials demonstrate that many HNSCC patients do not respond to cetuximab, despite HNSCC being overwhelmingly EGFR-positive. In HNSCC there is currently no corollary to k-ras in metastatic colorectal cancer, which has been shown to predict response to cetuximab. In colorectal cancer, cetuximab improves overall and progression free survival in patients with wild type k-ras and does not in patients with k-ras mutations. 110 In HNSCC, the mutations and alternate pathways theorized to possibly contribute to anti-EGFR resistance are numerous, including mutations in the extracellular domain (EGFRvIII) and tyrosine kinase domain, K-ras and H-ras, mutations in epithelial-mesenchymal transition such as increased vimentin expression, decreased E-Cadherin expression, decreased Claudins 4 and 7 expression, alternate pathways such as Cyclin D1 upregulation, PTEN mutations, PI3KCA mutations, Akt Amplification. 111 Elucidating these mutations and alternate pathways will be vital going forward in order to 1) combine anti-EGFR therapy synergistically with other agents and 2) predict who will respond to anti-EGFR therapy ie begin to personalize HNSCC treatment.
Table 1 displays ongoing research into multi-targeted therapeutic approaches that aim to enhance EGFR inhibition and/or inhibit EGFR escape pathways. For example, the Toll-like receptor (TLR) family are phylogenetically conserved mediators of innate immunity, essential for microbial recognition. TLR9 mediates a cellular response to unmethylated CpG dinucleotides, which are common in bacterial, but not mammalian DNA. TLR9 triggers a cascade responsible for activating macrophages, dendritic cells and natural killer cells, as well as inducing the secretion of inflammatory cytokines (interleukin-12, interleukin-6, tumor necrosis factor-α).112–114 Damiano et al tested whether the addition of TLR9 agonists to EGFR antagonist (cetuximab or gefitinib) affected growth of cetuximab sensitive (GEO) or cetuximab resistant (GEO-CR) colon cancer xenografts. They demonstrated that TLR9 agonist had a synergistic effect on GEO inhibition when combined with either cetuximab or gefitinib. Importantly, it also decreased downstream proliferation of activated pAkt, pMAPK, as well as cyclooxygenase-2, bcl-2 and VEGF, suggesting its potential role in preventing cetuximab resistance. In the GEO-CR xenografts, TLR9 agonist had minimal effect on its own, but boosted the non-EGFR dependent cetuximab activity (likely immune in nature). 115 An ongoing phase II trial is studying the efficacy of a TLR9 agonist (EMD 1201081) with cetuximab in patients with recurrent or metastatic HNSCC (Table 1).
Current trials combining cetuximab and other agents in the treatment of recurrent or metastatic head and neck squamous cell carcinoma (HNSCC).
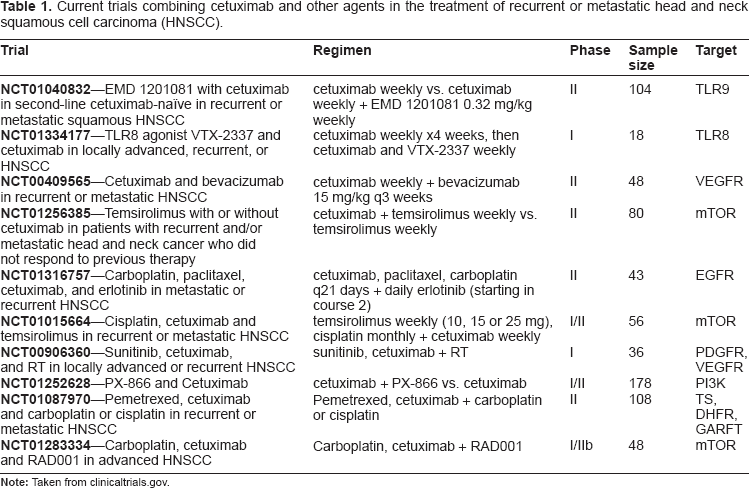
Dual inhibition of EGFR and VEGF has also emerged as an attractive treatment paradigm, as it appears that their actions are interrelated. Viloria-Petit developed resistant carcinoma xenografts in nude mice by progressively treating with cetuximab. While cell lines developed from these resistant tumors retained high EGFR expression, 5/6 of these cell lines had more than twice the VEGF mRNA and protein of the parent line. 116 Bianco et al demonstrated that silencing of VEGFR-1 in resistant cells restored sensitivity to anti EGFR therapy and that conversely, exogenous VEGFR-1 overexpression in wild type cells resulted in increased resistance. 117 The mechanism whereby EGFR status affects VEGF is not completely clear, but a possible link is STAT3, which is involved in signal transduction downstream of EGFR and also binds to the VEGF promoter region. 118 A phase I/II study of bevacizumab, an anti-VEGF antibody, with erlotinib in recurrent or metastatic HNSCC revealed a response rate of 15% with 4 complete responses. Of the patients in the phase II aspect of the protocol, 3/48 had serious grade 3 or higher bleeding toxicities, including death. Higher ratios of tumor-cell phosphorylated VEGF receptor-2 (pVEGFR2) over total VEGFR2 and endothelial-cell pEGFR over total EGFR in pretreatment biopsies were associated with complete response and tumor shrinkage in a subset of 11 patients with available tissue. 119 Preliminary results from an ongoing trial of bevacizumab and cetuximab in recurrent or metastatic HNSCC have shown a positive response to the combination of both drugs, with no hemorrhagic events. 120
In vitro inhibition of mTOR in HNSCC cell lines has been shown to have detrimental effects on the transmission of proliferative signals in the PI3K/Akt pathway. Inhibition of this pathway, and more specifically mTOR, can mediate antiproliferative and apoptotic effects in HNSCC cells, as was shown by Aissat et al with rapamycin. Concomitantly, in vivo inhibition of mTOR with rapamycin inhibits cell proliferation and induces apoptosis in HNSCC cells.121,122 Jimeno et al showed that temsirolimus, another mTOR inhibitor, had greater in vivo antitumor activity than erlotinib alone in HNSCC, but had a synergistic anti-tumor effect when used in combination with the EGFR inhibitor, implicating mTOR as a target for a multi-drug approach. 123 A recent French study showed that in combination with cetuximab, bevacizumab and RT, temsirolimus showed synergistic antiproliferative activity in HNSCC cells. 124 A number of currently ongoing phase I/II and II trials are studying the effects of temsirolimus in various combinations with cetuximab and platinum-based chemotherapeutic agents (Table 1).
Another potential cause of cetuximab resistance is the EGFR variant III (EGFRvIII) a mutation found in 42% of HNSCC tumors which results in a ligand-independent activation of the receptor. 125 EGFRvIII is not required to dimerize with another receptor for activation and signals downstream only through the PI3K pathway, unlike wild-type EGFR (wtEGFR). 126 The binding affinity of cetuximab to EGFRvIII is much lower compared to wtEGFR, providing an explanation for resistance of some HNSCC tumors to cetuximab. Furthermore, EGFRvIII mediates tumor cell migration and invasion by increased STAT3 activation and induction of HIF1-α, contributing to cetuximab resistance in HNSCC. Targeting this unique structure of EGFRvIII has recently become the focus of study in overcoming this resistance.127,128
Interestingly, to this point the most consistent marker of response to EGFR inhibitors is clinical: development of acneiform rash. In the Bonner trial, at 5-year follow up, patients in the cetuximab arm with a prominent acneiform rash (grade 2–4) had a significantly longer overall survival than those with a mild rash (68.8 vs. 25.6 months). This may implicate the acneiform rash as a biomarker for optimal outcome with cetuximab. 129 In addition to the aforementioned Bonner trial, numerous authors have reported a correlation between development of rash and response to EGFR inhibitors in various cancers including HNSCC, colorectal cancer, gynecologic and lung cancer.130–132
Cetuximab in HPV-positive HNSCC
Another direction of future research is how best to use EGFR inhibitors in the setting of HPV-positive HNSCC. HPV16 (the most commonly implicated HPV subtype in HNSCC) is thought to cause HNSCC via E6 and E7 genes, which encode oncoproteins that bind and degrade tumor suppressors p53 and retinoblastoma (pRb). 133 Several studies have implicated HPV tumor status as a strong and independent prognostic factor for survival in HNSCC.134–136 With regard to the relationship between HPV and EGFR, Kumar et al studied tissue samples from patients with oropharyngeal SCC cancer treated with induction chemotherapy followed by combination chemoradiotherapy. They found that tumors with low EGFR expression, regardless of HPV status, had the best disease-specific survival, whereas those with high EGFR expression and HPV-negative status had the poorest survival. 137 They concluded that low EGFR expression and high HPV titer are markers of good response to organ-sparing therapy in advanced oropharyngeal cancer. 138 Hong et al verified that patients with HPV-negative/EGFR-positive cancers had an adjusted 13-fold increased risk of having a loco-regional failure, and more than a 4-fold increased risk of dying of any cause relative to those with HPV-positive/EGFR-negative cancers. 139
The susceptibility of HPV-positive HNSCC tumors to conventional treatment modalities has been highlighted in recent studies. A Danish study of patients with HNSCC treated with conventional radiotherapy found that at 5-year follow-up, those with HPV16-positive tumors had better locoregional tumor control (58% vs. 28%), disease-specific survival (72% vs. 34%), and OS (62% vs. 26%) compared to those with HPV-negative tumors. 140 Oropharyngeal primaries are known to be more commonly HPV-positive than other subsites, and their prognosis is favorable compared to tobacco-related SCC.7,137,138,141,142 Kies et al showed that in HNSCC tumors treated with induction chemotherapy (ICT) (paclitaxel, carboplatin and cetuximab) followed by either radiation, concurrent CRT, or surgery, HPV-positivity correlated with superior progression-free survival and OS compared to HPV-negative tumors. Of note, all HPV-positive tumors were of oropharyngeal origin and 75% of HPV-positive patients with T1-2 primaries received single modality radiation after ICT. This suggests that ICT (including cetuximab) followed by radiotherapy may be particularly beneficial to patients with stage T0-2 HPV-positive tumors. 143 Another study using cetuximab in both ICT and subsequent concurrent CRT in patients with locally advanced HNSCC found that at 3 years the progression-free survival and OS was 70% and 74%, respectively. Subgroup analysis of HPV-positive and HPV-negative tumors did not reveal a significant difference in outcomes in this trial. 144 Subgroup analysis from the Bonner trial, where patients with oropharyngeal primaries appeared to respond better to cetuximab than other sites, might suggest that perhaps HPV-positive HNSCC are especially amenable to cetuximab. However, tumor specimens were not available for HPV determination in this trial, so direct testing of this hypothesis is not possible. Interestingly, a similar subgroup analysis of the EXTREME trial indicates that the oral cavity (not oropharynx) derived the most benefit from the addition of cetuximab.
In the near future, there should be randomized data from at least two phase III trials involving anti EGFR therapy and HPV-positive HNSCC. RTOG 1016 is an ongoing non-inferiority trial asking whether overall survival with cetuximab RT is equivalent to cisplatinum RT in patients with HPV-positive oropharyngeal SCC patients. The NCIC-CTG HN.6 chose a fully humanized anti-EGFR monocloncal antibody (panitumumab) that is thought to have similar activity as cetuximab, but without the potential allergic side effects. This is a phase III study of standard fractionation EBRT with concurrent cisplatinum versus accelerated fractionation EBRT with concurrent panitumumab in advanced HNSCC. It is stratified by anatomic subsite, includes HPV testing and completed target accrual in November 2011.
Conclusion
Cetuximab is an exciting treatment modality in metastatic/recurrent HNSCC because it has proven efficacy and at the same time, a relatively gentle toxicity profile compared to most chemotherapeutic agents. In the first line setting for incurable HNSCC, where several trials over the last few decades have demonstrated improvements in response rates but not overall survival, cetuximab improved median overall survival by 3 months in the EXTREME trial. Following progression on first line chemotherapy, there is no level 1 evidence for using cetuximab, though several phase II trials suggest that cetuximab monotherapy is a reasonable choice in this setting. Current research often involves novel combinations of drugs aimed at enhancing EGFR inhibition and/ or suppressing escape pathways. More intricate knowledge of the mechanisms of resistance to anti-EGFR therapy may someday lead to more targeted, more personalized therapies for our HNSCC patients.
Author Contributions
Wrote the first draft of the manuscript: AP. Contributed to the writing of the manuscript: JM, SK. Agree with manuscript results and conclusions: AP, JM, SK. Jointly developed the structure and arguments for the paper: AP, JM, SK. Made critical revisions and approved final version: AP, JM, SK. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.
Footnotes
Acknowledgements
We would like to thank Kelli VanNosdall for her help in preparing this manuscript.